

Abstract
Posttraumatic facial pain is due to an injured nerve, most often a branch of the trigeminal nerve. While surgical approaches to injuries of the supraorbital, supratrochlear, infraorbital, and inferior alveolar nerves have been reported, an injury to the anterior superior alveolar nerve (ASAN) has not been reported. An algorithm is proposed for the diagnosis of injury to the ASAN versus the infraorbital nerve itself. A case is reported in which pain relief was achieved by dividing the ASAN within the maxillary sinus, leaving the proximal end exposed within the sinus at the level of the orbital floor.
Keywords: anterior superior alveolar nerve, infraorbital nerve, neuroma
Posttraumatic facial pain is most often due to an injured nerve, and usually this is a branch of the trigeminal nerve. Based on improving knowledge of the anatomical pathways, 1 2 3 4 surgical approaches to the supraorbital/supratrochlear, 5 6 7 8 infraorbital, 6 9 10 11 and inferior alveolar nerves have been reported. 12 13 14 These surgeries have included neurolysis, neuroma resection, and nerve reconstruction. To our knowledge, an injury to the anterior superior alveolar nerve (ASAN) has not been reported, and indeed, the anatomic pathway of the ASAN has only recently been well described. 15 16 Here, we report an endoscopic transantral approach to ASAN neurectomy that is not a Le Fort I osteotomy. An algorithm for diagnosis is formulated based on nerve blocks and quantitative sensory testing to distinguish between an ASAN injury and an injury to the infraorbital nerve.
Case Report
A 52-year-old man presented with 15 years of intense burning pain in the gingiva overlying the left central and lateral maxillary incisors, teeth numbers 9 and 10 ( Fig. 1 ). He previously underwent an extensive array of procedures that all failed to relieve his pain. These included two posterior fossa microsurgical decompressions of the trigeminal nerve, “gamma knife” treatment, and a peripheral nerve stimulator placed alongside the infraorbital nerve for “atypical facial pain.” He also had root canal treatments to teeth numbers 9 and 10, and these teeth were subsequently extracted in an attempt to relieve the pain.
Fig. 1.

Site of pain, in the gingiva of the left central and lateral incisor.
Deeper questioning elicited a history of a sport-related injury (high-school level football) with a football helmet striking the left cheek. CT imaging demonstrated an old injury to the left canalis sinuosis ( Fig. 2 ), the bony canal within the medial maxillary wall that houses the ASAN along its course from the infraorbital nerve to the anterior maxillary teeth. The sensation of the upper lip was normal. A local anesthetic block of the ASAN gave complete pain relief, confirming a diagnosis of neuroma of the ASAN.
Fig. 2.

CT coronal image demonstrating normal canalis sinuosis (yellow arrow) on the right with damaged canalis sinuosis on the left.
At surgery, the ASAN was identified through a transantral approach. The portion of the ASAN in the horizontal position and entering the canalis sinuosis was translucent and without bands of Fontana, whereas the ASAN more proximally, just after leaving the infraorbital nerve, had a normal appearance ( Fig. 3 ). The bands of Fontana are an indicator of the pathophysiological condition of the nerve. The banding pattern frequently is not present during compression injuries to nerves. 17 18 19 It was elected to resect a portion of the damaged nerve, and leave the proximal end to regenerate into the maxillary sinus.
Fig. 3.
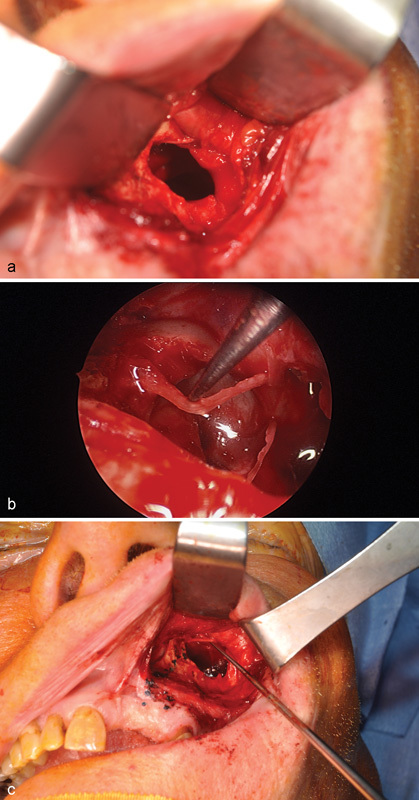
Intraoperative views: ( a ) incision in the left upper lip sulcus, with first view of the anterior superior alveolar nerve (ASAN) exiting inferior to the infraorbital nerve following maxillary antrotomy. ( b ) Antrotomy view of the ASAN in its horizontal course, being held by a nerve hook. ( c ) Brilliant green dye marking the anatomic pathway of the ASAN from the antrum to the tooth origins.
Operative Technique
The patient was placed in a supine position following nasoendotracheal intubation and prepped and draped in the standard sterile condition. Lidocaine 1% with 1:100,000 epinephrine solution was infiltrated into the left gingiva-buccal sulcus. A sublabial incision was performed. A subperiosteal dissection proceeded to identify the left infraorbital nerve. At the infraorbital nerve foramen, a branch of the infraorbital nerve, believed to be the ASAN, was visualized ( Fig. 3 ). The nerve was dissected distally into the maxillary bone to confirm the ASAN had been correctly identified ( Fig. 4 ). A maxillary antrostomy (Caldwell-Luc) was performed under the infraorbital nerve. While visualizing the infraorbital nerve using an endoscope, an osteotome was used to carefully release the infraorbital nerve from its bony foramen into the maxillary sinus. The ASAN could be seen directly branching from the infraorbital nerve. The nerve was divided at its take off from the infraorbital nerve and the proximal end was placed into the maxillary sinus. A distal segment of the nerve was sent for histopathological diagnosis, which confirmed resection of the ASAN. The incision was next closed in the standard fashion after replacing the maxillary bone pieces back into the maxillary antrostomy site as free bone grafts. The patient was observed overnight and sent home the following day without complication. Relief from the original pain was immediately achieved following resection of the ASAN. The patient, now 4 months out of surgery, no longer suffers from the original pain.
Fig. 4.

Schematic showing the surgical plan and anatomic course of anterior superior alveolar nerve in yellow.
Discussion
For a person to have symptoms due to isolated injury to the ASAN, other branches of the infraorbital nerve must be without symptoms. A history from the patient should include ipsilateral pain only in the labial gingiva about the central and lateral maxillary incisors. Gingival pain further lateral toward the bicuspids and molars must include branches of the medial and posterior superior alveolar nerve, while gingival pain involving the buccal gingiva must include branches of the greater palatine nerve. The most important diagnostic approach is to do a local anesthetic block of the nerves, the techniques for which are well described. 20 21 22
Documentation of infraorbital, nerve-innervated skin involvement with nerve injury can be done with quantitative sensory testing, and has also been well described. 9 23 24 25 Normal neurosensory testing of the upper lip, with a positive response to local anesthetic block of the ASAN, documents injury to the ASAN branch of the infraorbital nerve, and suggests the location of the nerve injury in the region found in the patient in the case reported here. Temporary pain relief was achieved through local blocks into the upper left gingival region of the central incision.
An algorithm for the management of facial pain due to an injury to the trigeminal nerve was suggested by Rosson et al in 2010. 11 That algorithm relies on first treating the patient with medical management, then consideration of which trigeminal nerve branch is involved by the history and anatomic location of the pain, then documentation of the involved branch by quantitative sensory testing, and finally confirming that role of that branch by local anesthetic nerve block. This is the approach used in the patient presented here, and which we suggest for future facial pain patients.
References
- 1.Konofaos P, Soto-Miranda M A, Ver Halen J, Fleming J C. Supratrochlear and supraorbital nerves: an anatomical study and applications in the head and neck area. Ophthal Plast Reconstr Surg. 2013;29(05):403–408. doi: 10.1097/IOP.0b013e318295fa09. [DOI] [PubMed] [Google Scholar]
- 2.Massey N D, Galil K A, Wilson T D. Determining position of the inferior alveolar nerve via anatomical dissection and micro-computed tomography in preparation for dental implants. J Can Dent Assoc. 2013;79:d39. [PubMed] [Google Scholar]
- 3.Matani J D, Kheur M G, Kheur S M, Jambhekar S S. The anatomic inter relationship of the neurovascular structures within the inferior alveolar canal: a cadaveric and histological study. J Maxillofac Oral Surg. 2014;13(04):499–502. doi: 10.1007/s12663-013-0563-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Eren E, Zeybek G, Ecevit C, Arslanoğlu S, Ergur I, Kiray A. A new method of identifying the posterior inferior nasal nerve: implications for posterior nasal neurectomy. J Craniofac Surg. 2015;26(03):930–932. doi: 10.1097/SCS.0000000000001504. [DOI] [PubMed] [Google Scholar]
- 5.Ramirez O M, Pozner J N.Endoscopically assisted supraorbital nerve neurolysis and correction of eyebrow asymmetry Plast Reconstr Surg 199710003755–758., discussion 759–760 [DOI] [PubMed] [Google Scholar]
- 6.Williams C G, Dellon A L, Rosson G D. Management of chronic facial pain. Craniomaxillofac Trauma Reconstr. 2009;2(02):67–76. doi: 10.1055/s-0029-1202593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lee K W, Kang S Y, Yang W Y. A case report of surgical treatment for relief of intractable pain developed after browlift surgery. J Korean Soc Plast Reconstr Surg. 2011;38(01):81–84. [Google Scholar]
- 8.Lee D. Treatment strategy for post-traumatic supraorbital and supratrochlear neuroma. J Trauma Treat. 2014;3(04):213. [Google Scholar]
- 9.Fogaça W C, Fereirra M C, Dellon A L. Infraorbital nerve injury associated with zygoma fractures: documentation with neurosensory testing. Plast Reconstr Surg. 2004;113(03):834–838. doi: 10.1097/01.prs.0000105335.41930.41. [DOI] [PubMed] [Google Scholar]
- 10.Rosenberg A, Sailer H F. A prospective study on changes in the sensibility of the oral mucosa and the mucosa of the upper lip after Le Fort I osteotomy. J Craniomaxillofac Surg. 1994;22(05):286–293. doi: 10.1016/s1010-5182(05)80078-2. [DOI] [PubMed] [Google Scholar]
- 11.Rosson G D, Rodriguez E D, George P, Dellon A L. Surgical algorithm for treatment of post-traumatic trigeminal nerve pain. Microsurgery. 2010;30(08):614–621. doi: 10.1002/micr.20793. [DOI] [PubMed] [Google Scholar]
- 12.Crawley W A, Dellon A L. Inferior alveolar nerve reconstruction with a polyglycolic acid bioabsorbable nerve conduit. Plast Reconstr Surg. 1992;90(02):300–302. [PubMed] [Google Scholar]
- 13.Evans G R, Crawley W, Dellon A L. Inferior alveolar nerve grafting: an approach without intermaxillary fixation. Ann Plast Surg. 1994;33(02):221–224. doi: 10.1097/00000637-199408000-00019. [DOI] [PubMed] [Google Scholar]
- 14.Robert R C, Bacchetti P, Pogrel M A.Frequency of trigeminal nerve injuries following third molar removal J Oral Maxillofac Surg 20056306732–735., discussion 736 [DOI] [PubMed] [Google Scholar]
- 15.Olenczak J B, Hui-Chou H G, Aguila D J, III, Shaeffer C A, Dellon A L, Manson P N. Posttraumatic midface pain: clinical significance of the anterior superior alveolar nerve and canalis sinuosus. Ann Plast Surg. 2015;75(05):543–547. doi: 10.1097/SAP.0000000000000335. [DOI] [PubMed] [Google Scholar]
- 16.von Arx T, Lozanoff S. Anterior superior alveolar nerve (ASAN) Swiss Dent J. 2015;125(11):1202–1209. doi: 10.61872/sdj-2015-11-01. [DOI] [PubMed] [Google Scholar]
- 17.Zachary L S, Dellon E S, Nicholas E M, Dellon A L. The structural basis of Felice Fontana's spiral bands and their relationship to nerve injury. J Reconstr Microsurg. 1993;9(02):131–138. doi: 10.1055/s-2007-1006661. [DOI] [PubMed] [Google Scholar]
- 18.Haninec P. Undulating course of nerve fibres and bands of Fontana in peripheral nerves of the rat. Anat Embryol (Berl) 1986;174(03):407–411. doi: 10.1007/BF00698791. [DOI] [PubMed] [Google Scholar]
- 19.Merolli A, Mingarelli L, Rocchi L. A more detailed mechanism to explain the “bands of Fontana” in peripheral nerves. Muscle Nerve. 2012;46(04):540–547. doi: 10.1002/mus.23422. [DOI] [PubMed] [Google Scholar]
- 20.Acharya A B, Banakar C, Rodrigues S V, Nagpal S, Bhadbhade S, Thakur S L. Anterior middle superior alveolar injection is effective in providing anesthesia extending to the last standing molar in maxillary periodontal surgery. J Periodontol. 2010;81(08):1174–1179. doi: 10.1902/jop.2010.100109. [DOI] [PubMed] [Google Scholar]
- 21.Bali R K, Nautiyal V P, Sharma P, Sharma R. Infra-orbital nerve block anesthesia-extended coverage using intra-oral ‘molar approach’. J Oral Biol Craniofac Res. 2011;1(01):53–54. doi: 10.1016/S2212-4268(11)60014-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Al Amoudi N, Feda M, Sharaf A, Hanno A, Farsi N. Assessment of the anesthetic effectiveness of anterior and middle superior alveolar injection using a computerized device versus traditional technique in children. J Clin Pediatr Dent. 2008;33(02):97–102. doi: 10.17796/jcpd.33.2.d666m2l43334274p. [DOI] [PubMed] [Google Scholar]
- 23.Poort L J, van Neck J W, van der Wal K G. Sensory testing of inferior alveolar nerve injuries: a review of methods used in prospective studies. J Oral Maxillofac Surg. 2009;67(02):292–300. doi: 10.1016/j.joms.2008.06.076. [DOI] [PubMed] [Google Scholar]
- 24.Dellon A L, Andonian E, DeJesus R A. Measuring sensibility of the trigeminal nerve. Plast Reconstr Surg. 2007;120(06):1546–1550. doi: 10.1097/01.prs.0000282097.75302.2a. [DOI] [PubMed] [Google Scholar]
- 25.Kim Y K, Yun P Y, Kim J H, Lee J Y, Lee W. The quantitative sensory testing is an efficient objective method for assessment of nerve injury. Maxillofac Plast Reconstr Surg. 2015;37(01):13. doi: 10.1186/s40902-015-0013-5. [DOI] [PMC free article] [PubMed] [Google Scholar]