

Abstract
Molecular Pathology (MP) is at the heart of modern diagnostics and translational research, but the controversy on how MP is best developed has not abated. The lack of a proper model or trained pathologists to support the diagnostic and research missions makes MP a rare commodity overall.
Here we analyse the scientific and technology areas, in research and diagnostics, which are encompassed by MP of solid tumours; we highlight the broad overlap of technologies and analytical capabilities in tissue research and diagnostics; and we describe an integrated model that rationalizes technical know‐how and pathology talent for both. The model is based on a single, accredited laboratory providing a single standard of high‐quality for biomarker discovery, biomarker validation and molecular diagnostics.
Keywords: Molecular pathology, Molecular diagnostics, Translational research
Highlights
Modern medicine is dictated by two main developments: molecular medicine and technical advances.
Molecular Pathology aims to achieve the integration of a research and diagnostic activities.
Academic molecular pathology, at the interface between diagnostics and research, drives such integration.
An integrated model has a synergistic effect in molecular diagnostics and translational research.
1. Introduction
The future of modern medicine is likely to be dictated by two main pillars: molecular medicine and technical advances. A key component of the former is personalised medicine and therapeutic pathology, i.e. the development of a new generation of drugs targeting specific genes and pathways, coupled with biomarkers that predict the individual patient's response to those drugs (Ozdemir et al., 2006). In this context, the discovery, validation and clinical application of novel biomarkers become a cornerstone of medical advancement. At the heart of biomarker‐related work is molecular pathology (MP) (Harris and McCormick, 2010).
It has become evident that, to advance in the translation of biomarker discovery into diagnostic and therapeutic application (depicted in Figure 1), the interface between basic research and diagnostics is the weakest link. This is the area that MP should be addressing. This cliché is usually accompanied by another truism, namely that MP is one of the most important, and yet less structured and developed areas in translational and clinical research.
Figure 1.
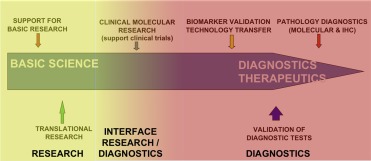
Pipeline to deliver basic science discoveries into diagnostic and therapeutic end‐points.
The purpose of this article is to review all the different components of what we call MP. By doing so, we would like to suggest an integrated model of provision of MP at all levels, from biomarker discovery to molecular diagnostics. To focus further on this exercise, we will concentrate on tissue molecular pathology of solid tumours and, hence, on the area of molecular onco‐pathology. This analysis of MP will illustrate the transition from traditional tissue‐based interpretation of morphology to advanced high‐throughput molecular technologies, and from biomarker discovery to molecular diagnostics (Dietel et al., 2013). It is our view that the integration of traditional and molecular pathology within a single laboratory management and delivery infrastructure is essential and that the perception of translational research and diagnostics is a continuum rather than two distinct entities. These facts are basic requirements for the future rationalisation and improvement of pathology services within the context of academic medicine.
2. Molecular pathology – translational research & molecular diagnostics
Why are pathologists needed in translational research, patient stratification and the delivery of personalized medicine? What can pathologists contribute as members of comprehensive, multidisciplinary research teams? There are indeed some aspects in research that can only be provided by pathologists who can interpret tissue phenotype underpinned by a deep understanding of the biological basis of disease, and have the inclination to be involved in research/academic duties. These capabilities can be presented as an integrated pipeline that would take the human tissue sample through different levels of traditional and molecular pathological interrogation (see Figure 2). These activities can be translated into specific techniques and technologies (see Table 1). While other scientists could fulfil some of these needs, it is perceived that only those able to integrate the morphological, clinical and molecular dimensions of the disease would be able to deliver them in an optimal fashion. These subspeciality areas with Molecular Pathology are discussed below.
Figure 2.
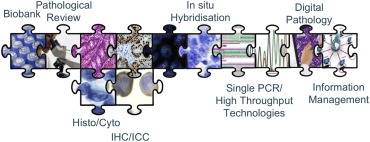
The integrated puzzle of pathology activities and technologies.
Table 1.
Pathology‐centred activities in the research endeavour.
| Molecular diagnostics in the context of clinical trials |
| Analysis of tissues ahead of molecular analyses |
| Tissue biobanking |
| Digital pathology |
| Pathology informatics |
| Data manager |
| Biomarker validation |
| Integration of validated biomarkers into routine diagnostics |
2.1. Molecular pathology and molecular diagnostics in the context of clinical trials
Clinical trials are at the true interface between science and clinical care. While they represent a research exercise strictly speaking, they also provide potential healthcare to patients and thus need to be carried‐out with strict clinical and diagnostic rigour (Simon and Roychowdhury, 2013). Typically, there are 2 levels of biomarker analysis in clinical trials, namely a) specific biomarker analysis to decide the stratification of patients within the trial, i.e. a priori testing, and b) general biomarker analysis to identify a biomarker (single or multiple) to predict patient response, i.e. a posteriori testing. Both are equally important. The biomarkers used in a priori testing may already be standard‐of‐care (for instance, a clinical trial aiming to provide alternative therapeutic avenues to cetuximab for KRAS mutant patients would need KRAS mutation analysis upfront), while others may represent a more experimental endeavour (such as detecting cMET status in trials using cMET inhibitors). In general, the predominant view is that these tests should be performed by practising diagnostic pathologists in accredited laboratories. A posteriori testing is increasingly performed with high‐throughput technologies (Simon and Roychowdhury, 2013). Again, although it is a discovery exercise, there is increasing consensus that this analysis should be driven by molecular pathologists, in accredited laboratories for that purpose (CAP, CPA, CLIA, etc) (Wheler et al., 2013), and with patterns of test validation, quality control and quality assurance (QA/QC) as close as possible to fully established clinical testing. Only then will any piece of discovery work be reliable for future use in the clinical context, should the trial lead to positive results.
2.2. Analysis of tissues ahead of molecular testing
Despite the predictions that molecular biology would substitute traditional microscopic morphological assessment of the disease, the reality is that genotype and phenotype are not mutually exclusive, but complementary (Muley et al., 2012). It would appear that high‐quality microscopy is a condition sine qua non for high‐quality molecular diagnostics. Indeed, the accurate morphological analysis ahead of the testing itself is essential to confirm that a) the sample is of the right histological type for analysis; b) that the ratio of malignant to non‐malignant cells is sufficient to attend to the sensitivity of the test; c) the sample is representative of the disease; d) there are no features to suggest that the pre‐analytical steps were not adequate (e.g. autolysis due to long ischaemia prior to fixation); e) there is no significant pathological process that might interfere with molecular profiling (e.g. such as a strong inflammatory component accompanying the malignant cells); f) there is no strong morphological heterogeneity that may introduce molecular heterogeneity and analytical bias; g) the staging of the cancer is adequate for the therapeutic approach intended. These and many other aspects of morphological interpretation of tissue samples represent an essential first step for the accurate understanding of the subsequent downstream molecular profiling of tissue samples. This would be best provided by those who are trained to interpret tissue morphology, understand the molecular basis of the disease and the molecular performance of the tests.
2.3. Tissue biobanking
The advancement of translational science requires access to large numbers of clinical biosamples that have been collected and stored with the highest of quality standards in ways that will allow molecular analysis (Simeon‐Dubach et al., 2012). Biobanks provide the infrastructure and the standards for these high‐quality sample collections. Not only is the quality of the tissue sample important but so too is the associated clinic‐pathological metadata that allows the correlation of molecular data with pathological taxonomy, therapeutic response and clinical outcomes. This dual pursue of quantity and quality may only be reached by integration of resources by several biobanks in “tissue research syndicates” for single, coordinated studies, and by the administration of biobanks not only of prospective fresh‐frozen collections, but also the retrospective, formalin‐fixed and paraffin‐embedded collections accumulated in the pathology archives. Very specific schemes for QA/QC of these cases, as well as the expansion of tissue biobanking services to include, for instance, the specific sample collection for the generation of cell lines or patient‐derived tumour xenografts, are again better driven by those who sit at both ends of the morpho‐molecular continuum. Indeed, this dual use of tissue biobanking facilities, as described before (Stanta et al. 2011), namely a) a resource of residual pathology tissues for translational research; and b) purpose‐developed xenograft tissue banking, are essential for translational cancer research.
One of the aspects that dictates the use of tissue bank collections for research purposes is the ethical framework that governs the use of such materials. As described before (Stanta et al. 2008), the use of clinical materials in research falls in between two often “colliding interests”, namely the greater good of this research to society and the right of the individual to “genetic anonymity”. While a careful analysis of the breath of international and national legislation on the subject is outside the remits of this opinion article, it is important to take into account, when evaluating a research project proposing specific use of patient samples, the ethical aspects of the objectives of the research, the methods to be used, the type of research or the type of biological material (Stanta et al. 2008).
2.4. Digital pathology
In biomarker discovery, part of the value of immunohistochemistry is because of its interpretative nature, in this context, the counter‐stain that provides an indication of the complex histological context is as important as the antibody or the probe that targets a specific protein or gene in the hybridization process. This allows us to recognize the cellular and subcellular localization of the expression or amplification, and provides meaningful insights on the molecular mechanism of diseases, as well as specific criteria for the adequacy of the test. However, in biomarker diagnostic testing, and particularly in the area of personalized medicine, the scoring of the biomarker should not be interpretative, but highly quantitative (Bai et al., 2013). This is one of the many functions of digital pathology (see Table 2). Understandably, tissue pathologists need to reach a balance of what is best delivered, for diagnostics and discovery, as a subjective interpretative opinion, and what is necessary to be digitalized and quantitated. Eventually, digital pathology may not only be a way to deliver better pathology services, but also a vehicle to remove some highly time‐consuming tasks carried‐out by pathologists, who would be playing a supervisory role in the digital pathology outcome and thus would have more time for other activities.
Table 2.
Digital pathology.
| Automated digitalization of images for storage and multi‐site discussion |
| Automated scoring of IHC |
| Automated counting of hybridization signals |
| Automated identification of tumour in sections for subsequent microdissection |
2.5. Pathology informatics and integromics
Bioinformatics is a term that describes a rapidly expanding field of statistical, machine learning and algorithmic developments that are needed to cope with the massive data sets generated in genomics research. The exploitation of genomic data in the context of tissues, patients, patient populations requires the extension of skills and technology to integrate clinical, pathological, therapeutic and outcome data from clinical records with underlying genomics to determine correlates, identify potential therapeutic targets and develop companion biomarkers. For the purpose of this review, Pathology Informatics refers to the in silico analysis and computer‐driven understanding of information derived from tissues samples (Park et al., 2013). This currently represents one of the main challenges in translational science and in molecular diagnostics but also needs to be driven with strong input by pathologists. How we integrate multi‐faceted data sets for biomarker discovery, translation and application is likely to dictate the pace of scientific discovery and the speed at which many new technologies are adopted in diagnostics. Table 3 summarizes the areas in which bioinformatics plays a pivotal role in Pathology. As with any other discipline that is beginning to find a space in diagnostics, it is now recognized that the validation of digital bioinformatics and/or high‐throughput bioinformatic approaches requires the same level of validation and accreditation as any other activity in molecular testing.
Table 3.
Pathology bioinformatics.
| Digital imaging |
| Pathology integration of pathological data, clinical data and biomarker analytical results |
| Translation of high‐throughput analysis to biomarkers with meaningful diagnostic/clinical relevance |
| Translation of high‐throughput analysis to pathology reports |
2.5.1. Digital imaging
The fundamental role of whole slide imaging, digital pathology and image analysis in biomarker analysis and validation has been argued before. The capability of creating interpretative algorithms able to translate digital patterns and intensities into quantitative, reproducible scores is fundamental to establish the credibility of tissue hybridization‐based techniques (immunohistochemistry, in‐situ hybridization, etc) in the context of personalized therapeutics. Computer enhanced approaches aiming to bring quantitation and objectivity to functions such as the recognition of tumour areas within a slide, the automated counting of hybridization signals or the quantitation of staining intensity will soon be part of our everyday diagnostic reporting, and are already receiving the necessary level of validation and regulatory approval to make this a reality.
2.5.2. Pathology integration of pathological data, clinical data and biomarker analytical results
Comprehensive translational research programmes will generate a plethora of information from clinical and pathological information of patient cohorts, as well as single/multiple biomarker testing for research and diagnostic. Those groups able to interoperate between data systems, integrate diverse data sets and interrogate the information to derive meaning, will have an enormous advantage in biomarker discovery. This demands a combination between modern bioinformatics and traditional biostatistics, and indeed a different set of skills than those involved in image analysis.
2.5.3. Analysis of high‐throughput tissue omics data
The area of bioinformatics applied to analysis of cDNA gene expression arrays, high‐throughput methylation, high‐throughput gene copy number and massive parallel sequencing, among others, has developed significantly in the last years. And, yet, the precise applications to diagnostics and the integration of all these platforms are still relatively rare. Those groups able to bring objectivity and rigour to these multi‐faceted, high‐throughput analyses, and able to deal with the ethical and practical barriers of translating these results into routine pathology reporting, will be in a stronger position to deliver single patient management based on an understanding of their genomic signature.
2.6. Biomarker validation and integration of validated biomarkers into routine diagnostics
One of the most puzzling aspects in molecular medicine is the large time gap between the initiation of modern molecular biology (with the discovery of the structure of the DNA around 1953), and the application of these discoveries in cancer diagnostics and in the decision of therapeutic interventions. Several reasons have been given for this including the lack of real knowledge of the biology of the biomarkers discovered, the lack of robust technology able to deliver these biomarkers in a consistent manner in molecular diagnostic laboratories and, more recently, the poorly designed and inadequately statistically powered biomarker studies to allow the results to be translated into diagnostic or clinical care (Drucker and Krapfenbauer 2013). The latter is essential. A new generation of pathologists is required to design and carry out these studies with the best chances of success. Biomarker discovery and validation in retrospective and prospective cohorts, understanding of the confounding effects of all the components of the biomarker study (from technology to sample choice), attention to basic aspects of validations such as sensitivity, specificity, precision, accuracy, detection limits or reportable range, or clear definition of diagnostic and clinical values, are areas in which specific training is required, and prerequisites for a successful biomarker study. Similarly, the final stages of this biomarker into routine diagnostics is likely to need industry support for the manufacturing of kits and reagents, and a multi‐centre final analysis to define the adequate protocols to ensure reproducibility in multiple laboratories.
2.7. Molecular diagnostics
The broader discipline of pathology and laboratory medicine has embraced molecular diagnostics in different way and with varying degrees of enthusiasm. Some laboratory areas have evolved into an almost full molecular discipline (such as virology or clinical genetics) and others have integrated molecular diagnostics upfront (e.g. haematology). Disappointingly, anatomic (surgical) pathologists are not always involved in the generation of FFPE‐related molecular testing. The reasons can be multiple and have been discussed before (Chan and Salto‐Tellez 2012). It is therefore imperative to fully train new generations of tissue and cellular pathologists in molecular diagnostics (Lauwers et al., 2010). Numerous molecular tests are at the core of tissue diagnostics. These include Sarcoma Translocation Detection, Lymphoma Translocation Detection, Clonality Testing, Microsatellite Instability Testing, Mismatch Repair Protein Expression, KRAS/NRAS Mutation Testing, BRAF Mutation Testing, EGFR Mutation Testing, ALK Protein Expression and EML4‐ALK Translocation Detection, Multiple Central Nervous System Molecular Testing, ER, PR and Her2 Protein Expression, Her2 Amplification, c‐KIT Mutation Analysis and PDGFRA Mutation Analysis. These are just some of the many emerging tests that, in the authors' opinion, should be in the hands of “molecular tissue pathologists”. The core competencies that would allow tissue pathologists to engage in this endeavour have been described elsewhere (Flynn et al., 2014), and can be easily incorporated into training programmes.
3. An integrated model for molecular tissue pathology of cancer – what does it mean?
Many years back there was a need to clearly separate the activities of molecular diagnostic laboratories and research operations. This was essential to introduce laboratory rigour into diagnostic practice (Dorsey 1989) and to delineate clearly the budgets for academic research and healthcare service laboratories. Almost 30 years later, we may wish to redefine the degree of synergy that academia and healthcare require. As we have tried to argue so far, that high‐end molecular diagnostics and translational research share similar qualities and demands. The technology involved, the technical know‐how, the need for laboratory quality (accredited by key agencies), the need to empower biomarker testing with a downstream diagnostic translation, and perform diagnostic‐standard testing in clinical trials. The interfaces are too many to continue an artificial division in these two endeavours. In the last three decades, we should have learnt to delineate research and diagnostic budgets and maintain laboratory quality, while enjoying the advantages of a single vision for MP. The more integrated this vision can be, even up to the point of sharing a single laboratory operation with both diagnostic and research capabilities, the easier it will be to bridge the world of discovery and diagnostics, and better serve the interest of cancer patients.
4. The current challenges in the provision of molecular tissue pathology of cancer
Regardless of the model of molecular pathology adopted, there are significant challenges and opportunities in the area of molecular testing of cancer. The opportunity is generated by the application of Next Generation Sequencing (NGS) technologies that are able to detect multiple, potentially “actionable” targets with increasing sensitivity in single clinical samples. The challenge is derived from: a) the relatively small number of targets with strong clinical utility proven in randomized trials; and b) the increase cost of these new technologies (Salto‐Tellez and de Castro, 2014). Molecular Pathology operations deal in different ways with the dichotomy between willingness to perform broad and comprehensive testing (particularly in academic oncology centres) and the need to maintain costs within a manageable framework. In the back of this dichotomy there is an uncomfortable feeling: only those who begin to learn how to deal with the complexities of multiple genomic information in the clinic with individual patients will be able to enter the era of contemporary molecular oncology.
The questions are multiple and the answers are unclear:
Should we perform high‐throughput mutation analysis to all patients? Perhaps only on those entering clinical trials? Or should these technologies be used exclusively within the realm of research?
How comprehensive should the testing be? Should we target only those actionable targets that are standard‐of‐care (perhaps a handful)? Should we test for all potential actionable targets (current “cancer panels” can include more than 400 genes)? Or should we perform wider testing that will provide information on other pathways that eventually may be of help?
Who should pay for the testing? Is it still the responsibility of health insurance companies, or government‐supported healthcare schemes? Should this follow exclusively within the realm of research? How much responsibility has industry in this exercise?
Regardless of the answers, these questions are already announcing a change of paradigm: the interface between diagnostics and research is not as clear‐cut as it used to be. It is difficult to decide nowadays if the use of a 400‐gene test in a patient with advance cancer is a clinical need, a research endeavour, a go‐in‐between, or all of the above. In this context, the molecular pathology hybrid model suggested before may facilitate the answer to some of these questions. For instance, in our laboratory we started the use of NGS technology as a research activity, but validating the analysis as close as possible to a diagnostic test as we could (McCourt et al., 2013). Because of this, we are confident that our results with a limited panel can be of clinical use, regardless of the original reason for testing. Similarly, testing that is performed in the context of a research study on a so‐called “cancer of unmet clinical needs”, is generating results in key genes that can dictate standard‐of‐care, opening new therapeutic avenues beyond conventional testing. The impact that this is currently having in our patients globally is difficult to quantitate, but is possibly more related to the number of routine patients with sufficient DNA quality for analysis than any other technical consideration. However, those of us performing NGS testing with a therapeutic intention know that we need to do so if we want to enter the future of molecular diagnostics and oncology treatment. In acting like this, we operate in the interface between diagnostics and research, stressing the fact that this hybrid approach may be the best way academic molecular pathology will be able to attend not only to the patients of today, but also to the patients of tomorrow.
Acknowledgements
The Northern Ireland – Molecular Pathology Laboratory is supported by Cancer Research – UK, the Experimental Cancer Medicine Centre Network and the Northern Ireland Friends of the Cancer Centre.
Salto-Tellez Manuel, James Jacqueline A., Hamilton Peter W., (2014), Molecular pathology – The value of an integrative approach, Molecular Oncology, 8, doi: 10.1016/j.molonc.2014.07.021.
References
- Bai, Y. , Cheng, H. , Bordeaux, J. , Neumeister, V. , Kumar, S. , Rimm, D.L. , Stern, D.F. , 2013. Comparison of HER2 and phospho-HER2 expression between biopsy and resected breast cancer specimens using a quantitative assessment method. PLoS One. 8, (11) e79901 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chan, J.Y. , Salto-Tellez, M. , 2012. Opinion: molecular gestalt and modern pathology. Adv. Anat. Pathol. 19, (6) 425–426. [DOI] [PubMed] [Google Scholar]
- Dietel, M. , Jöhrens, K. , Laffert, M. , Hummel, M. , Bläker, H. , Müller, B.M. , Lehmann, A. , Denkert, C. , Heppner, F.L. , Koch, A. , Sers, C. , Anagnostopoulos, I. , 2013. Predictive molecular pathology and its role in targeted cancer therapy: a review focussing on clinical relevance. Cancer Gene Ther. 20, (4) 211–221. [DOI] [PubMed] [Google Scholar]
- Dorsey, D.B. , 1989. Evolving concepts of quality in laboratory practice. A historical overview of quality assurance in clinical laboratories. Arch. Pathol. Lab. Med. 113, (12) 1329–1334. [PubMed] [Google Scholar]
- Drucker, E. , Krapfenbauer, K. , 2013. Pitfalls and limitations in translation from biomarker discovery to clinical utility in predictive and personalised medicine. E.P.M.A. J. 4, (1) 7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flynn, C. , James, J. , Maxwell, P. , McQuaid, S. , Ervine, A. , Catherwood, M. , Loughrey, M.B. , McGibben, D. , Somerville, J. , McManus, D.T. , Gray, M. , Herron, B. , Salto-Tellez, M. , 2014. Integrating molecular diagnostics into histopathology training: the Belfast model. J. Clin. Pathol. 67, (7) 632–636. 10.1136/jclinpath-2014-202176 [DOI] [PubMed] [Google Scholar]
- Harris, T.J. , McCormick, F. , 2010. The molecular pathology of cancer. Nat. Rev. Clin. Oncol. 7, (5) 251–265. [DOI] [PubMed] [Google Scholar]
- Lauwers, G.Y. , Black-Schaffer, S. , Salto-Tellez, M. , 2010. Molecular pathology in contemporary diagnostic pathology laboratory: an opinion for the active role of surgical pathologists. Am. J. Surg. Pathol. 34, (1) 115–117. [DOI] [PubMed] [Google Scholar]
- McCourt, C.M. , McArt, D.G. , Mills, K. , Catherwood, M.A. , Maxwell, P. , Waugh, D.J. , Hamilton, P. , O'Sullivan, J.M. , Salto-Tellez, M. , 2013. Validation of next generation sequencing technologies in comparison to current diagnostic gold standards for BRAF, EGFR and KRAS mutational analysis. PLoS One. 8, (7) e69604 10.1371/journal.pone.0069604 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muley, T. , Herth, F.J.F. , Schnabel, P. , Dienemann, H. , Meister, M. , 2012. From tissue to molecular phenotyping: pre-analytical requirements Heidelberg Experience. Transl. Lung Cancer Res. 1, (2) 111–121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ozdemir, V. , Williams-Jones, B. , Glatt, S.J. , Tsuang, M.T. , Lohr, J.B. , Reist, C. , 2006. Shifting emphasis from pharmacogenomics to theranostics. Nat. Biotechnol. 24, (8) 942–946. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Park, S. , Parwani, A.V. , Aller, R.D. , Banach, L. , Becich, M.J. , Borkenfeld, S. , Carter, A.B. , Friedman, B.A. , Rojo, M.G. , Georgiou, A. , Kayser, G. , Kayser, K. , Legg, M. , Naugler, C. , Sawai, T. , Weiner, H. , Winsten, D. , Pantanowitz, L. , 2013. The history of pathology informatics: a global perspective. J. Pathol. Inform. 30, (4) 7 10.4103/2153-3539.112689 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salto-Tellez, M. , de Castro, D.G. , 2014. Next generation sequencing: a change of paradigm in molecular diagnostic validation. J. Pathol. 10.1002/path.4365 [DOI] [PubMed] [Google Scholar]
- Stanta, G. , Cescato, A. , Bonin, S. , Barbazza, R. , 2008. Bioethics considerations for medical research in human archive tissues: the point of view of the researcher. Virchows Arch. 453, (1) 117–119. [DOI] [PubMed] [Google Scholar]
- Stanta, G. , Bonin, S. , Machado, I. , Llombart-Bosch, A. , 2011. Models of biobanking and tissue preservation: RNA quality in archival samples in pathology laboratories and “in vivo biobanking” by tumor xenografts in nude mice-two models of quality assurance in pathology. Biopreserv. Biobank. 9, (2) 149–155. [DOI] [PubMed] [Google Scholar]
- Simeon-Dubach, D. , Burt, A.D. , Hall, P.A. , Oct 1 2012. Quality really matters: the need to improve specimen quality in biomedical research. J. Pathol. 10.1002/path.4117 [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- Simon, R. , Roychowdhury, S. , 2013. Implementing personalized cancer genomics in clinical trials. Nat. Rev. Drug Discov. 12, (5) 358–369. [DOI] [PubMed] [Google Scholar]
- Wheler, J. , Hong, D. , Swisher, S.G. , Falchook, G. , Tsimberidou, A.M. , Helgason, T. , Naing, A. , Stephen, B. , Janku, F. , Stephens, P.J. , Yelensky, R. , Kurzrock, R. , 2013. Thymoma patients treated in a phase I clinic at MD Anderson Cancer Center: responses to mTOR inhibitors and molecular analyses. Oncotarget. 4, (6) 890–898. [DOI] [PMC free article] [PubMed] [Google Scholar]