

Abstract
Background
It has been reported that internet gaming disorder (IGD) and smokers with nicotine dependence (SND) share clinical characteristics, such as over-engagement despite negative consequences and cravings. This study is to investigate the alterations in the resting-state functional connectivity (rsFC) of the dorsolateral prefrontal cortex (DLPFC) observed in SND and IGD. In this study, 27 IGD, 29 SND, and 33 healthy controls (HC) underwent a resting-state functional magnetic resonance imaging (rs-fMRI) scan. DLPFC connectivity was determined in all participates by investigating the synchronized low-frequency fMRI signal fluctuations using a temporal seed-based correlation method.
Results
Compared with the HC group, the IGD and SND groups showed decreased rsFC with DLPFC in the right insula and left inferior frontal gyrus with DLPFC. Compared with SND group, the IGD subjects exhibited increased rsFC in the left inferior temporal gyrus and right inferior orbital frontal gyrus and decreased rsFC in the right middle occipital gyrus, supramarginal gyrus, and cuneus with DLPFC.
Conclusion
Our results confirmed that SND and IGD share similar neural mechanisms related to craving and impulsive inhibitions. The significant difference in rsFC with DLPFC between the IGD and SND subjects may be attributed to the visual and auditory stimulation generated by long-term internet gaming.
Keywords: Functional magnetic resonance imaging, Internet gaming disorder, Nicotine dependence, Resting-state functional connectivity, Dorsolateral prefrontal cortex
Background
Internet gaming disorder (IGD), also known as problematic internet use, is the excessive and recurrent use of online internet games [1]. IGD is different from substance abuse or drug addiction such that no substance or chemical intake is involved; however, excessive internet use may lead to physical dependence similar to that observed in other addictions [2]. Currently, IGD has become a serious mental health issue around the world, thereby requiring additional investigation, as exemplified by its inclusion as a condition for further study in Section 3 of the Diagnostic and Statistical Manual of Mental Disorders (5th Edition, DSM-5) [3]. The following diagnostic criteria for IGD were suggested: time distortion, time spent longer than initially intended and planned time, use of internet activity to cope with or escape problems, compulsive behavior, deception about the extent of use, failure to stop or control use, and preoccupation with internet use when offline [4–6]. Notably, many of these behavioral symptoms resemble substance-related disorders [7–9].
Currently the precise pathogenesis of IGD remains unclear. A few studies suggested that the risk factor of IGD is related to the increased prevalence of substance dependence [10–12]. Numerous studies found that IGD and substance dependence shared similar neural mechanisms, such as nicotine dependence [9, 13, 14]. On the basis of behavioral addiction, researchers have been attempting to associate IGD with other behavioral problems that can lead to addiction, such as drug abuse, alcohol abuse, and nicotine dependence [7, 15]. Our previous study revealed that smokers with IGD exhibited decreased resting-state functional connectivity (rsFC) in the right rectus gyrus and increased rsFC in the left middle frontal gyrus with post cingulate cortex (PCC), compared with nonsmokers with IGD. Furthermore, negatively correlation was found in the PCC connectivity with the right rectus gyrus with Chen’s internet addiction score (CIAS) of smokers with IGD before correction. The results suggested that, compared with the nonsmokers with IGD, smokers with IGD had alterations of function in brain regions related to executive motivation and function [9]. However, Vergara et al. [16] delineated a general pattern of hypoconnectivity in the precuneus, insula, postcentral gyrus, and visual cortex of substance consumers. In addition, connectivity reduction between postcentral and one resting state networks covering right fusiform and lingual gyri showed their significant association with severity of hazardous drinking. In smokers, hypoconnectivity between the thalamus and putamen was observed. By contrast, the angular gyrus showed hyper-connectivity with the precuneus linked to smoking and significantly correlated with the severity of nicotine dependence. These results suggested that particular effects of alcohol and nicotine can be separated and identified. Han et al. [8] found IGD subjects and alcohol dependence (AD) have positive rsFC values in the dorsolateral prefrontal cortex (DLPFC) and cingulate, cerebellum, as well as negative rsFC values between the DLPFC and orbitofrontal cortex. The AD group was found to have positive rsFC values between the DLPFC, striatal areas, and temporal lobe, whereas the IGD group shows negative rsFC values among these areas. They concluded that the both groups may have deficits in executive function.
In this study, we attempted to detect the difference between the rsFC of individuals with IGD and those of smokers with nicotine dependence (SND), and explore the mechanism of this difference. According to Han et al. [8], cravings induced by particular substances such as alcohol are closely associated with DLPFC activity [17]. Furthermore, DLPFC is thought to play key roles in mediating clinical symptoms of executive dysfunction, alcohol dependence, including impulsivity, and aggravation of abuse potential [18]. The present study aims to assess DLPFC-seeded rsFC in IGD and SND.
Methods
Participants
The current study was approved by the Research Ethics Committee of Ren Ji Hospital and School of Medicine, Shanghai Jiao Tong University, China No.[2016]079k(2) with written informed consent from all subjects. All participants were informed of the aims of our study before MRI examination. Of the 86 participants included in the study and were evaluated by brain MRI from Jan 2016 to Dec 2016, 27 had IGD, 29 SND, and 30 healthy controls (HC). As described in our previously study [9], the IGD subjects who met the diagnostic questionnaire for internet addiction (i.e., YDQ) test modified by Beard and Wolf [19] were recruited from the psychological outpatient clinic at the Shanghai Mental Health Center. While, the SND and HC groups were recruited through advertisements. The IGD group played internet game approximately 42–70 h (mean ± SD: 44.31 ± 10.27) per week. The appropriate questions from the Structured Clinical Interview for DSM-IV [20] was used to assess nicotine dependence. The participant from the IGD and HC groups had never smoked, and no participant self-reported daily alcohol consumption or other substance use disorder (SUD). All the SND subjects began smoking 2–10 years before the current study onset. They are all daily smokers, and they smoke approximately 10–45 cigarettes (mean ± SD: 21 ± 1.76) per day. CIAS [21], self-rating anxiety scale (SAS) [22], self-rating depression scale (SDS) [23], Barratt impulsiveness scale-11 (BIS-11) [24], and Fagerstrom test of nicotine dependence (FTND) [25] were performed to assess the clinical characteristics of the participants. CIAS is a self-reported measure with good reliability and validity and has been used to measure the severity of internet addiction [26]. The FTND is a six-item self-report questionnaire used to assess the severity of nicotine dependence [25]. All questionnaires were initially written in English and then translated into Chinese.
All the participants were right handed, and none of participants had (1) previous hospitalization for a history of major psychiatric disorders or psychiatric disorders; (2) a substance use disorders other than nicotine addiction; (3) mental retardation; (4) neurological illness or injury; (5) intolerance to MRI.
MRI acquisition
Images were obtained using a 3.0T MRI scanner (GE Signa HDxt 3T, USA) with a standard head coil. Restraining foam pads was used to reduce head motion and earplugs were used to reduce scanner noise. The SND group was required to abstain from smoking 1 h before scanning. Resting-state functional MRI data were acquired using a gradient-echo echo-planar sequence as described in our previously study [9]. Afterward, 34 transverse slices (repetition time [TR] = 2000 ms, echo time [TE] = 30 ms; field of view [FOV] = 230 × 230 mm2; 3.6 × 3.6 × 4 mm3 voxel size) were obtained aligned along the anterior commissure-posterior commissure line. Each fMRI scan lasted 440 s. During the scanning, the participants were instructed to stay awake with their eyes closed and do not think any specific subjects. After scanning, the subjects were asked to confirm they remain awake during the scan. In addition, high-resolution T1-weighted anatomical images (TR = 6.1 ms, TE = 2.8 ms, TI = 450 ms, slice thickness = 1 mm, gap = 0, flip angle = 15°, FOV = 256 × 256 mm2, number of slices = 166, 1 × 1 × 1 mm3 voxel size) using a 3D fast spoiled gradient recalled sequence images.
Statistical analysis
The demographic and clinical measures of the groups were compared. One-way ANOVA tests were carried out using Statistical Package for the Social Sciences software (version 18) to assess the differences among the 3 groups. Bonferroni post hoc tests were then performed to assess the differences between each pair of groups. A 2-tailed p value of 0.05 was considered statistically significant for all analyses.
Functional MRI preprocessing was performed using a toolbox for data processing and analysis for brain imaging (http://rfmri.org/dpabi) [27]. After discarding the first 10 volumes of each functional time series, the remaining 210 images were preprocessed. Slice-timing correction, realignment, and spatial normalization, as well as smoothing (6 mm full width at half maximum), were conducted. Nuisance covariates, including time-series predictors for global, cerebrospinal fluid, white matter and six movement parameters were regressed out to improve the signal-to-noise ratio and minimize the motion artifact. No participant in this study exhibited movement greater than 1.5 mm with maximum translation in x, y, or z, axes or maximum rotation of 1.5° in the 3 axes. Moreover, the mean framewise displacement (FD) was computed by averaging the FDi of each subject from each time point [28]. No difference among the mean FD values of the groups (p = 0.71). Then, we applied temporal filtering (0.01–0.08 Hz) to the time series of each voxel to reduce the influence of high-frequency noise and low-frequency drift [29–32]. DLPFC was used as the region of interest (ROI) seed in the current study, and the DLPFC template was made as described in previous research [8].
Then, the blood-oxygen-level-dependent signal time series of the in each voxel within the seed region were averaged to generate the reference time series. A correlation map for each subject was produced by computing the correlation coefficients between the reference time series and time series from the other brain voxels. Z values were converted from the correlation coefficients by Fisher’s z-transform to improve the normality of the distribution [31]. Afterwards, the individual z-scores were entered into SPM8 for the one-sample t test in a voxel-wise manner, which was performed to determine the brain regions with significant positive or negative correlation with the DLPFC within each group. Individual scores were entered into SPM8 for random effect analysis, and then one-way ANOVA were performed.
Differences with regard to age, sex, education, SAS scores, SDS scores, and BIS-11 scores were regressed for each rsFC along the subject dimension. Multiple comparison corrections were performed using the AlphaSim program in the Analysis of Functional Neuroimages (AFNI) software package (NIMH, Bethesda, MD USA; available at http://afni.nimh.nih.gov/afni) [33], as determined by Monte Carlo simulations. Significant differences were defined as those which survived a threshold of p < 0.05, AlphaSim corrected (a combined threshold of p < 0.001 for each voxel and a cluster size >11 voxels, yielding a corrected threshold of p < 0.05). Group interaction analyses were then carried out with two-sample t-tests. The differences were obtained according to the results of ANOVA by applying the mask to limit the t-tests to the significant brain areas. AlphaSim corrected threshold p < 0.05 (a combined threshold of p < 0.001 and a cluster size >11 voxels) was performed as multiple comparison correction. Brain regions exhibiting significant differences were then masked on the MNI brain templates.
Results
Demographic and clinical characteristics
Table 1 listed the demographic and clinical measures for each group. No significant difference was observed between the IGD and HC groups in terms of age and years of education. However, significant differences were found between the IGD and SND groups and between the HC and SND groups. Difference with respect to sex was obtained because no female smoker participated in the study. The IGD subjects had higher CIAS, SAS, SDS, and BIS-11 compared with other 2 groups.
Table 1.
Demographic and clinical characteristics of the three groups
| IGD (n = 27) | HC (n = 33) | SND (n = 29) | F value (p value) | p1-2 | p1-3 | p2-3 | |
|---|---|---|---|---|---|---|---|
| (Mean ± SD) | (Mean ± SD) | (Mean ± SD) | |||||
| Age (years) | 20.78 ± 2.20 | 20.78 ± 2.51 | 22.58 ± 2.41 | 5.56 (0.005) |
1 | 0.02 | 0.01 |
| Sex (F/M) | 8/19 | 6/27 | 0/33 | 12.091 (0.001) |
0.30 | 0.001 | 0.02 |
| Education (years) | 11.26 ± 1.67 | 12.67 ± 2.58 | 13.03 ± 2.06 | 5.19 (0.007) |
0.43 | 0.01 | 1 |
| Chen Internet Addiction Scale (CIAS) | 75.15 ± 9.95 | 44.27 ± 9.81 | 46.76 ± 8.34 | 98.29 (<0.001) |
<0.001 | <0.001 | 0.45 |
| Self-Rating Anxiety Scale (SAS) | 51.33 ± 10.16 | 39.61 ± 6.39 | 44.48 ± 8.96 | 14.09 (<0.001) |
<0.001 | 0.01 | 0.08 |
| Self-rating depression scale (SDS) | 54.56 ± 10.80 | 43.12 ± 8.85 | 47.44 ± 9.13 | 10.66 (<0.001) |
<0.001 | 0.02 | 0.24 |
| Barratt Impulsiveness Scale-11 (BIS-11) | 61.22 ± 8.44 | 52.82 ± 6.64 | 52.41 ± 7.50 | 12.36 (<0.001) |
<0.001 | <0.001 | 1 |
| FTND | 6.52 ± 2.11 |
p 1-2 for IGD group versus HC group, p 1-3 for IGD group versus SND group, p 2-3 for HC group versus SND group
SD standard deviation, HC healthy control, IGD internet gaming disorder, SND smokers with nicotine dependence, FTND Fagerstrom test of nicotine dependence
DLPFC connectivity analysis
One-way ANOVA analysis in three groups
Significant differences were observed among the rsFC with the DLPFC in the left side of inferior temporal gyrus, insula, inferior frontal gyrus, right side of the middle temporal gyrus, supramarginal gyrus, cuneus, superior orbital frontal gyrus, insula, inferior orbital frontal gyrus, and superior frontal gyrus (Table 2; Fig. 1).
Table 2.
Significant differences in functional connectivity of different brain regions with DLPFC changes among the three groups
| Peak MNI coordinate region | Peak MNI coordinates | Number of cluster voxels | Peak F value | |||
|---|---|---|---|---|---|---|
| x | y | z | ||||
| 1 | Left inferior temporal gyrus (BA20) | −51 | −15 | −27 | 29 | 15.69 |
| 2 | Left insula (BA48) | −36 | 16 | −11 | 20 | 8.46 |
| 3 | Left inferior frontal gyrus (BA45) | −51 | 27 | 6 | 22 | 14.70 |
| 4 | Right middle temporal gyrus (BA19) | 42 | −72 | 0 | 47 | 21.28 |
| 5 | Right supramarginal gyrus (BA40) | 63 | −48 | 27 | 30 | 11.32 |
| 6 | Right cuneus (BA19) | 15 | −84 | 30 | 75 | 13.43 |
| 7 | Right superior orbital frontal gyrus (BA11) | 15 | 54 | −21 | 39 | 13.96 |
| 8 | Right insula (BA47) | 27 | 21 | −18 | 22 | 13.61 |
| 9 | Right inferior orbital frontal gyrus (BA38) | 48 | 27 | −12 | 61 | 10.56 |
| 10 | Right superior frontal gyrus (BA9) | 24 | 42 | 42 | 15 | 9.68 |
MNI Montreal Neurological Institute, BA Brodmann’s area, DLPFC dorsolateral prefrontal cortex
p < 0.05, AlphaSim-corrected
Fig. 1.
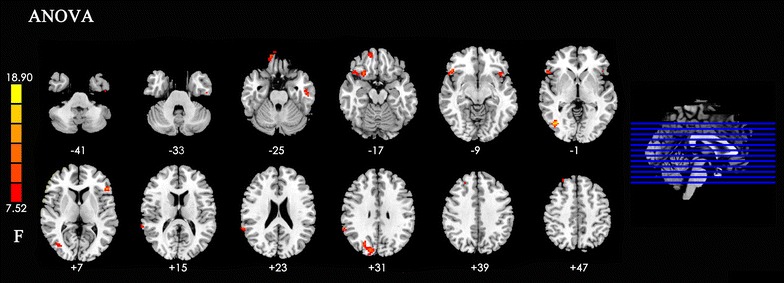
Significant differences in functional connectivity of different brain regions with DLPFC changes among the three groups. Note: The left part of figure represents the participant’s right side, and right represents the participant’s left side. DLPFC dorsolateral prefrontal cortex
Between-group analysis of DLPFC connectivity: IGD versus HC
The IGD group exhibited significantly increased rsFC in left inferior temporal gyrus, right superior temporal gyrus, and right middle frontal gyrus with the DLPFC, compared with the HC group. In addition, decreased rsFC was found in the left inferior frontal lobe, right side of the medial frontal orbital gyrus, insula, middle occipital gyrus, superior temporal gyrus, and cuneus with the DLPFC (Table 3; Fig. 2).
Table 3.
Summary of functional connectivity with DLPFC changes in IGD compared with the HC group
| Peak MNI coordinate region | Peak MNI coordinates | Number of cluster voxels | Peak t value | |||
|---|---|---|---|---|---|---|
| x | y | z | ||||
| 1 | Left inferior temporal gyrus (BA20) | −54 | −21 | −27 | 29 | 4.14 |
| 2 | Right superior temporal gyrus (BA38) | 48 | 24 | −21 | 14 | 2.51 |
| 3 | Right middle frontal gyrus (BA9) | 27 | 42 | 42 | 15 | 3.15 |
| 4 | Left inferior frontal gyrus (BA45) | −45 | 24 | 0 | 22 | −2.81 |
| 5 | Right medial frontal orbital lobe (BA11) | 18 | 57 | −18 | 16 | −1.88 |
| 6 | Right insula (BA48) | 27 | 15 | −18 | 21 | −2.22 |
| 7 | Right middle occipital gyrus (BA19) | 39 | −75 | 3 | 47 | −2.26 |
| 8 | Right superior temporal gyrus (BA22) | 65 | −45 | 24 | 30 | −3.62 |
| 9 | Right cuneus (BA19) | 18 | −84 | 27 | 67 | −3.67 |
t > 0 indicates IGD group >HC group in functional connectivity, t < 0 indicates IGD group <HC group in functional connectivity with DLPFC
MNI Montreal Neurological Institute, BA Brodmann’s area, DLPFC dorsolateral prefrontal cortex, IGD internet gaming disorder, HC healthy control
p < 0.05, AlphaSim-corrected
Fig. 2.
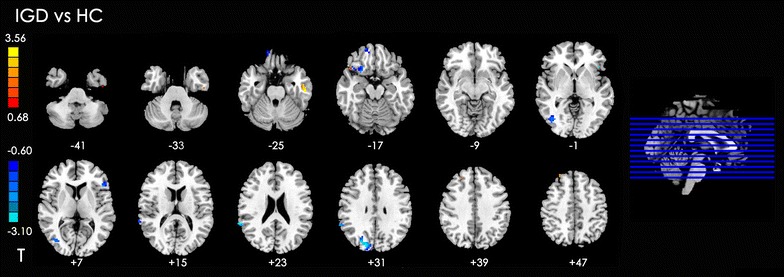
Significant between-group differences in functional connectivity of different brain regions with DLPFC between the IDG with HC subjects. The t-score bars are shown on the left. Red indicates IGD > HC, and blue indicates IDG < HC. Note: The left part of figure represents the participant’s right side, and right represents the participant’s left side. DLPFC dorsolateral prefrontal cortex, IGD internet gaming disorder, HC healthy control
Between-group analysis of DLPFC connectivity: SND versus HC
The SND group showed significantly decreased rsFC in bilateral insula, left inferior frontal gyrus, and right inferior orbital frontal gyrus with the DLPFC (Table 4; Fig. 3).
Table 4.
Summary of functional connectivity with DLPFC changes in SND group compared with the HC group
| Peak MNI coordinate region | Peak MNI coordinates | Number of cluster voxels | Peak t value | |||
|---|---|---|---|---|---|---|
| x | y | z | ||||
| 1 | Left inferior frontal gyrus (BA45) | −51 | 27 | 6 | 20 | −5.47 |
| 2 | Left insula (BA48) | −42 | 15 | −9 | 13 | −4.10 |
| 3 | Right insula (BA47) | 27 | 21 | −18 | 21 | −5.41 |
| 4 | Right inferior orbital frontal gyrus (BA38) | 48 | 27 | −12 | 27 | −5.70 |
t < 0 indicates SND group <HC group in functional connectivity with DLPFC
MNI Montreal Neurological Institute, BA Brodmann’s area, DLPFC dorsolateral prefrontal cortex, SND smokers with nicotine dependence, HC healthy control
p < 0.05, AlphaSim-corrected
Fig. 3.

Significant between-group differences in functional connectivity of different brain regions with DLPFC between SND and HC subjects. The t-score bar is shown on the left. Blue indicates SND group < HC. Note: The left part of figure represents the participant’s right side, and right represents the participant’s left side. DLPFC dorsolateral prefrontal cortex, SND smokers with nicotine dependence, HC healthy control
Between-group analysis of DLPFC connectivity: IGD versus SND
Compared with the SND group, the IGD subjects had increased rsFC in the left inferior temporal gyrus and right inferior orbital frontal gyrus and decreased rsFC in the right side of the middle occipital gyrus, supramarginal gyrus, and cuneus with the DLPFC (Table 5; Fig. 4).
Table 5.
Summary of functional connectivity with DLPFC changes in IGD group compared with the SND group
| Peak MNI coordinate region | Peak MNI coordinates | Number of cluster voxels | Peak t value | |||
|---|---|---|---|---|---|---|
| x | y | z | ||||
| 1 | Left inferior temporal gyrus (BA20) | −51 | −15 | −27 | 12 | 5.17 |
| 2 | Right inferior orbital frontal gyrus (BA38) | 48 | 27 | −12 | 27 | 5.01 |
| 3 | Right middle occipital gyrus (BA19) | 42 | −73 | 0 | 39 | −6.70 |
| 4 | Right supramarginal gyrus (BA48) | 63 | −48 | 27 | 26 | −4.54 |
| 5 | Right cuneus (BA19) | 12 | 86 | 30 | 46 | −4.58 |
t > 0 indicates IGD group >SND group in functional connectivity with DLPFC, t < 0 indicates IGD group <SND group in functional connectivity with DLPFC
MNI Montreal Neurological Institute, BA Brodmann’s area, DLPFC dorsolateral prefrontal cortex, IGD internet gaming disorder, SND smokers with nicotine dependence
p < 0.05, AlphaSim-corrected
Fig. 4.
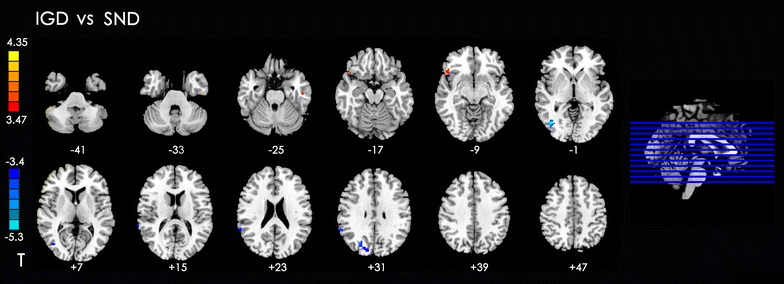
Significant between-group differences in functional connectivity of different brain regions with DLPFC between IGD and SND groups. The t-score bars are shown on the left. Red indicates IGD > SND, and blue indicates IGD < SND. Note: The left part of figure represents the participant’s right side, and right represents the participant’s left side. DLPFC dorsolateral prefrontal cortex, IGD internet gaming disorder, SND smokers with nicotine dependence
Correlation between DLPFC connectivity and CIAS of IGD, DLPFC connectivity, and FTND of SND
Compared with the HC group, the IGD and SND both had decreased rsFC in the left inferior frontal gyrus and right insula with DLPFC. The rsFC strength values (mean zFC values) were extracted and averaged within a spherical ROI (radius of 10 mm) centered on the difference peak of the rsFC group (Tables 2, 3) in the IGD and SND groups. Pearson correlations were performed between the rsFC values with CIAS of the IGD group and the FTND score in SND group. However, no significant correlation was found.
Discussion
In this study, we observe both similar and different brain connectivities in IGD group related to SND group. We detected that both the SND and IGD groups had decreased rsFC with DLPFC in the right insula and left inferior frontal gyrus. Furthermore, the IGD subjects exhibited different rsFC with DLPFC in the orbital frontal cortex and temporal, occipital, and parietal lobes.
Evidence revealed that many of the behavioral symptoms, even the neural mechanisms underlying IGD, resemble SUD [14, 34]. SUD involves a chronic, recurrent pattern of drug, nicotine, or alcohol use, and nicotine dependence is one of its most common forms. SUD could result in neurological alterations, particularly in frontal lobe structures implicated in cognitive-behavioral control. The network of cortical regions dysfunction, including the DLPFC, anterior cingulate cortex and lateral parietal cortex, relates to deficits in behavioral inhibition. This dysfunction has been linked to the loss of control over substance intake, which could be a critical step in the progression of SUD pathology [35, 36]. IGD is different from SUD in that no chemical or substance intake is involved; however, excessive internet use may also lead to physical dependence similar to that observed in other addictions [2]. Particularly, the hypo-activation of the inhibition circuit is a shared neural mechanism in SUD and behavioral addiction. Impaired function of the prefrontal cortex may relate to high impulsivity, which in turn, may contribute to impaired cognitive control and development of IGD [37]. Although the exact mechanism of IGD requires further investigation, its cognitive–behavioral model has been proposed. The model focuses on three domains including motivational drives related to reward-seeking and stress-reduction, behavioral control relating to executive inhibition, and decision-making that involves weighing the pros and cons of engaging in motivated behaviors [38].
Based on previous studies, both functional and structural abnormalities of the DLPFC have been commonly observed in IGD [39, 40]. Complex cognitive functions have usually been associated with activations in DLPFC [41] such as conflict-induced behavioral adjustment, attention, working memory, and inhibitory control [42–44]. DLPFC is connected with other cortical areas and links current sensory experiences to memory of past experiences to direct and generate properly goal-directed action [13, 45]. Therefore, the DLPFC may contribute to the coordination and keeping of the representations accepted from the other brain regions during the craving response when substance cues are present and a positive expectancy has been generated [46].
We detected that both the SND and IGD groups had decreased rsFC in the right insula and left inferior frontal gyrus with DLPFC. The insula has been implicated in cue-induced craving and relapse in nicotine-dependent tobacco cigarette smokers [47]. And the orbitofrontal cortex is involved in the evaluation of the reward of stimuli and explicit representation of reward expectancy for the substance [7]. Our results were consistent with the previous studies, which emphasized the brain regions, such as ventromedial prefrontal cortex, insula, thalamus, and cerebellum, which was critically linked with cigarette smoking. Structural MRI studies revealed that the integrities of the gray matters in the prefrontal cortex, anterior cingulate cortex, insula, thalamus, and cerebellum were reduced in smokers [48–50]. Liu et al. [51] investigated the brain function of IGD individuals using task-state fMRI. The IGD group showed increased activation in the right side of superior parietal lobule, insular lobe, precuneus, cingulated gyrus, superior temporal gyrus, and left side of brainstem. Internet video games activate the space, attention, vision, and execution centers located in the temporal, parietal, occipital, and frontal gyri. Abnormal brain function was noted in IGD subjects with hypofunction of the frontal cortex. Liu et al. detected IGD subjects that showed laterality activation of the right cerebral hemisphere, and they found that most areas were located in the right hemisphere. Neuroimaging studies in healthy subjects reported that the right hemisphere, especially in the right inferior frontal gyrus, is activated following successful response inhibition [52, 53]. During failed response inhibitions (i.e., trials that erroneously generated motor responses), the midline frontal structures, particularly the dorsomedial prefrontal cortex (dmPFC) encompassing pre-supplementary motor area and dorsal anterior cingulate cortex, are usually activated [54]. Consequently, the right inferior frontal gyrus is critical for response inhibition, whereas dmPFC is associate with response monitoring, particularly conflict and error monitoring [14].
The IGD subjects exhibited different rsFC with DLPFC in the orbital frontal cortex and temporal, occipital, and parietal lobes. Our result was partly similar with the result of a previous research compared rsFC with DLPFC in alcohol dependence with those in IGD [8]. They suggested that the connectivity observed in alcohol dependence is different from that in IGD because of the different comorbid diseases, early prevalence age, and visual and auditory stimulations in the former. Visual and auditory attentions are the results of the main sensory system inputs in response to internet game play [55]. Visual acuity loss or hearing problems may cause by extreme internet gaming [56]. Increased cortical volume within the parietal cortex was related to long-term gaming in pro-gamers, and thus may be related to increased visuospatial attention [57, 58].
Naturally, this study also comes with limitations. First, the cross-sectional design prevented us from determining whether the group differences in the rsFC are vulnerability factors for IGD and nicotine dependence. Second, the group sizes were unbalanced in our study, and the parameters such as sex, age, and education were not matched in the three groups. The unbalance group sizes might have influenced the results even though the variety was controlled during the statistical analysis. Third, the mean FTND in the SND group was 6.5, and thus the severity of nicotine dependence was not sufficiently high. Thus, increasing the number of participants is necessary.
Conclusion
The rsFC is a very powerful tool for exploring multifaceted neuropsychiatric diseases, such as substance and non-substance addiction at system level. Our results confirmed that nicotine dependence and IGD may share similar mechanisms related to craving and impulsive inhibition. The observed difference between the rsFC of subjects with IGD and those of SND may be attributed to the impairments in audiovisual information processing by long-term internet gaming.
Acknowledgments
Authors’ contributions
Conceptualization: YZ and JX; Formal analysis: YS, MC, YW, and YZ; Investigation: XG, YS, WD, MC, YD, and XH; Methodology: YW and YZ; Visualization: YS; Writing—original draft: XG, YS, and YZ; Writing—review and editing: YZ. All authors have read and approved the final version.
Acknowledgements
Not applicable
Competing interests
The authors declare that the research was conducted in the absence of commercial and financial relationships that can be construed as potential conflicts of interest.
Availability of data and material
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
The current study was approved by the Research Ethics Committee of Ren Ji Hospital and School of Medicine, Shanghai Jiao Tong University, China No.[2016]079k(2). All participants were informed of the aims of our study before MRI examination. Each participant submitted a written informed consent.
Funding
This research was supported by the National Natural Science Foundation of China (No. 81571650), and Shanghai Science and Technology Committee Medical Guide Project (western medicine) (No. 17411964300). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- IGD
internet gaming disorder
- SND
smokers with nicotine dependence
- rsFC
resting-state functional connectivity
- DLPFC
dorsolateral prefrontal cortex
- HC
healthy controls
- rs-fMRI
resting-state functional magnetic resonance imaging
- PCC
post cingulate cortex
- CIAS
Chen’s internet addiction score
- AD
alcohol dependence
- SUD
substance-related disorders
- SAS
self-rating anxiety scale
- SDS
self-rating depression scale
- BIS-11
Barratt impulsiveness scale-11
- FTND
Fagerstrom test of nicotine dependence
- TR
repetition time
- TE
echo time
- FOV
field of view
- FD
framewise displacement
- ROI
region of interest
- AFNI
Analysis of Functional Neuroimages
- dmPFC
dorsomedial prefrontal cortex
Footnotes
Xin Ge and Yawen Sun have contributed equally to this work
Contributor Information
Xin Ge, Email: yaner1475@163.com, Email: gexinrenji@126.com.
Yawen Sun, Email: cjs1119@hotmail.com.
Xu Han, Email: hanxu_ygritte@163.com.
Yao Wang, Email: wangyao852204526@163.com.
Weina Ding, Email: dingmeina1987@163.com.
Mengqiu Cao, Email: caomengqiu0@163.com.
Yasong Du, Email: 2283494193@qq.com.
Jianrong Xu, Phone: +86 21 68383545, Email: xujianr@hotmail.com.
Yan Zhou, Phone: +86 21 68383257, Email: clare1475@sina.com, Email: clare1475@hotmail.com.
References
- 1.Meng Y, Deng W, Wang H, Guo W, Li T. The prefrontal dysfunction in individuals with internet gaming disorder: a meta-analysis of functional magnetic resonance imaging studies. Addict Biol. 2015;20(4):799–808. doi: 10.1111/adb.12154. [DOI] [PubMed] [Google Scholar]
- 2.Dong G, Hu Y, Lin X. Reward/punishment sensitivities among internet addicts: implications for their addictive behaviors. Prog Neuropsychopharmacol Biol Psychiatry. 2013;46:139–145. doi: 10.1016/j.pnpbp.2013.07.007. [DOI] [PubMed] [Google Scholar]
- 3.Potenza M. Perspective: behavioural addictions matter. Nature. 2015;522(7557):S62. doi: 10.1038/522S62a. [DOI] [PubMed] [Google Scholar]
- 4.Young KS. Psychology of computer use: XL. Addictive use of the internet: a case that breaks the stereotype. Psychol Rep. 1996;79(3 Pt 1):899–902. doi: 10.2466/pr0.1996.79.3.899. [DOI] [PubMed] [Google Scholar]
- 5.Atmaca M. A case of problematic internet use successfully treated with an SSRI-antipsychotic combination. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(4):961–962. doi: 10.1016/j.pnpbp.2007.01.003. [DOI] [PubMed] [Google Scholar]
- 6.Shapira NA, Lessig MC, Goldsmith TD, Szabo ST, Lazoritz M, Gold MS, Stein DJ. Problematic internet use: proposed classification and diagnostic criteria. Depress Anxiety. 2003;17(4):207–216. doi: 10.1002/da.10094. [DOI] [PubMed] [Google Scholar]
- 7.Ko CH, Liu GC, Yen JY, Yen CF, Chen CS, Lin WC. The brain activations for both cue-induced gaming urge and smoking craving among subjects comorbid with internet gaming addiction and nicotine dependence. J Psychiatr Res. 2013;47(4):486–493. doi: 10.1016/j.jpsychires.2012.11.008. [DOI] [PubMed] [Google Scholar]
- 8.Han JW, Han DH, Bolo N, Kim B, Kim BN, Renshaw PF. Differences in functional connectivity between alcohol dependence and internet gaming disorder. Addict Behav. 2015;41:12–19. doi: 10.1016/j.addbeh.2014.09.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chen X, Wang Y, Zhou Y, Sun Y, Ding W, Zhuang Z, Xu J, Du Y. Different resting-state functional connectivity alterations in smokers and nonsmokers with internet gaming addiction. Biomed Res Int. 2014;2014:825787. doi: 10.1155/2014/825787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lee YS, Han DH, Kim SM, Renshaw PF. Substance abuse precedes internet addiction. Addict Behav. 2013;38(4):2022–2025. doi: 10.1016/j.addbeh.2012.12.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Padilla-Walker LM, Nelson LJ, Carroll JS, Jensen AC. More than a just a game: video game and internet use during emerging adulthood. J Youth Adolesc. 2010;39(2):103–113. doi: 10.1007/s10964-008-9390-8. [DOI] [PubMed] [Google Scholar]
- 12.Aj VANR, Kuss DJ, Griffiths MD, Shorter GW, Schoenmakers MT. D VDM: the (co-)occurrence of problematic video gaming, substance use, and psychosocial problems in adolescents. J Behav Addict. 2014;3(3):157–165. doi: 10.1556/JBA.3.2014.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ko CH, Liu GC, Hsiao S, Yen JY, Yang MJ, Lin WC, Yen CF, Chen CS. Brain activities associated with gaming urge of online gaming addiction. J Psychiatr Res. 2009;43(7):739–747. doi: 10.1016/j.jpsychires.2008.09.012. [DOI] [PubMed] [Google Scholar]
- 14.de Ruiter MB, Oosterlaan J, Veltman DJ, van den Brink W, Goudriaan AE. Similar hyporesponsiveness of the dorsomedial prefrontal cortex in problem gamblers and heavy smokers during an inhibitory control task. Drug Alcohol Depend. 2012;121(1–2):81–89. doi: 10.1016/j.drugalcdep.2011.08.010. [DOI] [PubMed] [Google Scholar]
- 15.Sung J, Lee J, Noh HM, Park YS, Ahn EJ. Associations between the risk of internet addiction and problem behaviors among Korean Adolescents. Korean J Fam Med. 2013;34(2):115–122. doi: 10.4082/kjfm.2013.34.2.115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Vergara VM, Liu J, Claus ED, Hutchison K, Calhoun V. Alterations of resting state functional network connectivity in the brain of nicotine and alcohol users. Neuroimage. 2017;151:45–54. doi: 10.1016/j.neuroimage.2016.11.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.George MS, Anton RF, Bloomer C, Teneback C, Drobes DJ, Lorberbaum JP, Nahas Z, Vincent DJ. Activation of prefrontal cortex and anterior thalamus in alcoholic subjects on exposure to alcohol-specific cues. Arch Gen Psychiatry. 2001;58(4):345–352. doi: 10.1001/archpsyc.58.4.345. [DOI] [PubMed] [Google Scholar]
- 18.Jasinska AJ, Stein EA, Kaiser J, Naumer MJ, Yalachkov Y. Factors modulating neural reactivity to drug cues in addiction: a survey of human neuroimaging studies. Neurosci Biobehav Rev. 2014;38:1–16. doi: 10.1016/j.neubiorev.2013.10.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Beard KW, Wolf EM. Modification in the proposed diagnostic criteria for internet addiction. Cyberpsychol Behav. 2001;4(3):377–383. doi: 10.1089/109493101300210286. [DOI] [PubMed] [Google Scholar]
- 20.First MBSR, Gibbon M, Williams JBW. Structured clinical interview for DDS-IV axis I disorders, clinician version (SID-CV) Washington, DC: American Psychiatric Press; 1996. [Google Scholar]
- 21.Chen SHWL, Su YJ, Wu HM, Yang PF. Development of Chinese Internet Addiction Scale and its psychometric study. Chin J Psychol. 2003;45(3):279–294. [Google Scholar]
- 22.Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi: 10.1016/S0033-3182(71)71479-0. [DOI] [PubMed] [Google Scholar]
- 23.Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12:63–70. doi: 10.1001/archpsyc.1965.01720310065008. [DOI] [PubMed] [Google Scholar]
- 24.Patton JH, Stanford MS, Barratt ES. Factor structure of the Barratt impulsiveness scale. J Clin Psychol. 1995;51(6):768–774. doi: 10.1002/1097-4679(199511)51:6<768::AID-JCLP2270510607>3.0.CO;2-1. [DOI] [PubMed] [Google Scholar]
- 25.Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom KO. The Fagerstrom test for nicotine dependence: a revision of the Fagerstrom Tolerance Questionnaire. Br J Addict. 1991;86(9):1119–1127. doi: 10.1111/j.1360-0443.1991.tb01879.x. [DOI] [PubMed] [Google Scholar]
- 26.Ko CH, Yen JY, Yen CF, Chen CC, Yen CN, Chen SH. Screening for internet addiction: an empirical study on cut-off points for the Chen Internet Addiction Scale. Kaohsiung J Med Sci. 2005;21(12):545–551. doi: 10.1016/S1607-551X(09)70206-2. [DOI] [PubMed] [Google Scholar]
- 27.Yan CG, Wang XD, Zuo XN, Zang YF. DPABI: data processing & analysis for (resting-state) brain imaging. Neuroinformatics. 2016;14(3):339–351. doi: 10.1007/s12021-016-9299-4. [DOI] [PubMed] [Google Scholar]
- 28.Power JD, Barnes KA, Snyder AZ, Schlaggar BL, Petersen SE. Spurious but systematic correlations in functional connectivity MRI networks arise from subject motion. NeuroImage. 2012;59(3):2142–2154. doi: 10.1016/j.neuroimage.2011.10.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Greicius MD, Krasnow B, Reiss AL, Menon V. Functional connectivity in the resting brain: a network analysis of the default mode hypothesis. Proc Natl Acad Sci USA. 2003;100(1):253–258. doi: 10.1073/pnas.0135058100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Biswal B, Yetkin FZ, Haughton VM, Hyde JS. Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magn Reson Med. 1995;34(4):537–541. doi: 10.1002/mrm.1910340409. [DOI] [PubMed] [Google Scholar]
- 31.Lowe MJ, Mock BJ, Sorenson JA. Functional connectivity in single and multislice echoplanar imaging using resting-state fluctuations. Neuroimage. 1998;7(2):119–132. doi: 10.1006/nimg.1997.0315. [DOI] [PubMed] [Google Scholar]
- 32.Rogers P. The cognitive psychology of lottery gambling: a theoretical review. J Gambl Stud. 1998;14(2):111–134. doi: 10.1023/A:1023042708217. [DOI] [PubMed] [Google Scholar]
- 33.Cox RW. AFNI: software for analysis and visualization of functional magnetic resonance neuroimages. Comput Biomed Res Int J. 1996;29(3):162–173. doi: 10.1006/cbmr.1996.0014. [DOI] [PubMed] [Google Scholar]
- 34.Baggio S, Dupuis M, Studer J, Spilka S, Daeppen JB, Simon O, Berchtold A, Gmel G. Reframing video gaming and internet use addiction: empirical cross-national comparison of heavy use over time and addiction scales among young users. Addiction. 2016;111(3):513–522. doi: 10.1111/add.13192. [DOI] [PubMed] [Google Scholar]
- 35.Motzkin JC, Baskin-Sommers A, Newman JP, Kiehl KA, Koenigs M. Neural correlates of substance abuse: reduced functional connectivity between areas underlying reward and cognitive control. Hum Brain Mapp. 2014;35(9):4282–4292. doi: 10.1002/hbm.22474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.George O, Koob GF. Individual differences in prefrontal cortex function and the transition from drug use to drug dependence. Neurosci Biobehav Rev. 2010;35(2):232–247. doi: 10.1016/j.neubiorev.2010.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Weinstein A, Livny A, Weizman A. New developments in brain research of internet and gaming disorder. Neurosci Biobehav Rev. 2017;75:314–330. doi: 10.1016/j.neubiorev.2017.01.040. [DOI] [PubMed] [Google Scholar]
- 38.Dong G, Potenza MN. A cognitive-behavioral model of internet gaming disorder: theoretical underpinnings and clinical implications. J Psychiatr Res. 2014;58:7–11. doi: 10.1016/j.jpsychires.2014.07.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Du X, Yang Y, Gao P, Qi X, Du G, Zhang Y, Li X, Zhang Q. Compensatory increase of functional connectivity density in adolescents with internet gaming disorder. Brain Imaging Behav. 2016. doi:10.1007/s11682-016-9655-x. [DOI] [PubMed]
- 40.Yuan K, Qin W, Wang G, Zeng F, Zhao L, Yang X, Liu P, Liu J, Sun J, von Deneen KM, et al. Microstructure abnormalities in adolescents with internet addiction disorder. PLoS ONE. 2011;6(6):e20708. doi: 10.1371/journal.pone.0020708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Naghavi HR, Nyberg L. Common fronto-parietal activity in attention, memory, and consciousness: shared demands on integration? Conscious Cogn. 2005;14(2):390–425. doi: 10.1016/j.concog.2004.10.003. [DOI] [PubMed] [Google Scholar]
- 42.Scherf KS, Sweeney JA, Luna B. Brain basis of developmental change in visuospatial working memory. J Cogn Neurosci. 2006;18(7):1045–1058. doi: 10.1162/jocn.2006.18.7.1045. [DOI] [PubMed] [Google Scholar]
- 43.Oldrati V, Patricelli J, Colombo B, Antonietti A. The role of dorsolateral prefrontal cortex in inhibition mechanism: a study on cognitive reflection test and similar tasks through neuromodulation. Neuropsychologia. 2016;91:499–508. doi: 10.1016/j.neuropsychologia.2016.09.010. [DOI] [PubMed] [Google Scholar]
- 44.Mansouri FA, Buckley MJ, Tanaka K. Mnemonic function of the dorsolateral prefrontal cortex in conflict-induced behavioral adjustment. Science. 2007;318(5852):987–990. doi: 10.1126/science.1146384. [DOI] [PubMed] [Google Scholar]
- 45.Vanderschuren LJ, Everitt BJ. Behavioral and neural mechanisms of compulsive drug seeking. Eur J Pharmacol. 2005;526(1–3):77–88. doi: 10.1016/j.ejphar.2005.09.037. [DOI] [PubMed] [Google Scholar]
- 46.Bonson KR, Grant SJ, Contoreggi CS, Links JM, Metcalfe J, Weyl HL, Kurian V, Ernst M, London ED. Neural systems and cue-induced cocaine craving. Neuropsychopharmacology. 2002;26(3):376–386. doi: 10.1016/S0893-133X(01)00371-2. [DOI] [PubMed] [Google Scholar]
- 47.Moran-Santa Maria MM, Hartwell KJ, Hanlon CA, Canterberry M, Lematty T, Owens M, Brady KT, George MS. Right anterior insula connectivity is important for cue-induced craving in nicotine-dependent smokers. Addict Biol. 2015;20(2):407–414. doi: 10.1111/adb.12124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Fritz HC, Wittfeld K, Schmidt CO, Domin M, Grabe HJ, Hegenscheid K, Hosten N, Lotze M. Current smoking and reduced gray matter volume—a voxel-based morphometry study. Neuropsychopharmacology. 2014;39(11):2594–2600. doi: 10.1038/npp.2014.112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Kuhn S, Romanowski A, Schilling C, Mobascher A, Warbrick T, Winterer G, Gallinat J. Brain grey matter deficits in smokers: focus on the cerebellum. Brain Struct Funct. 2012;217(2):517–522. doi: 10.1007/s00429-011-0346-5. [DOI] [PubMed] [Google Scholar]
- 50.Franklin TR, Wetherill RR, Jagannathan K, Johnson B, Mumma J, Hager N, Rao H, Childress AR. The effects of chronic cigarette smoking on gray matter volume: influence of sex. PLoS ONE. 2014;9(8):e104102. doi: 10.1371/journal.pone.0104102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Liu J, Li W, Zhou S, Zhang L, Wang Z, Zhang Y, Jiang Y, Li L. Functional characteristics of the brain in college students with internet gaming disorder. Brain Imaging Behav. 2016;10(1):60–67. doi: 10.1007/s11682-015-9364-x. [DOI] [PubMed] [Google Scholar]
- 52.Forman SD, Dougherty GG, Casey BJ, Siegle GJ, Braver TS, Barch DM, Stenger VA, Wick-Hull C, Pisarov LA, Lorensen E. Opiate addicts lack error-dependent activation of rostral anterior cingulate. Biol Psychiatry. 2004;55(5):531–537. doi: 10.1016/j.biopsych.2003.09.011. [DOI] [PubMed] [Google Scholar]
- 53.Hampshire A, Chamberlain SR, Monti MM, Duncan J, Owen AM. The role of the right inferior frontal gyrus: inhibition and attentional control. Neuroimage. 2010;50(3):1313–1319. doi: 10.1016/j.neuroimage.2009.12.109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Modirrousta M, Fellows LK. Dorsal medial prefrontal cortex plays a necessary role in rapid error prediction in humans. J Neurosci. 2008;28(51):14000–14005. doi: 10.1523/JNEUROSCI.4450-08.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Dong G, Huang J, Du X. Alterations in regional homogeneity of resting-state brain activity in internet gaming addicts. Behav Brain Funct. 2012;8:41. doi: 10.1186/1744-9081-8-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Bovo R, Ciorba A, Martini A. Environmental and genetic factors in age-related hearing impairment. Aging Clin Exp Res. 2011;23(1):3–10. doi: 10.1007/BF03324947. [DOI] [PubMed] [Google Scholar]
- 57.Hyun GJ, Shin YW, Kim BN, Cheong JH, Jin SN, Han DH. Increased cortical thickness in professional on-line gamers. Psychiatry Investig. 2013;10(4):388–392. doi: 10.4306/pi.2013.10.4.388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Song WH, Han DH, Shim HJ. Comparison of brain activation in response to two dimensional and three dimensional on-line games. Psychiatry Investig. 2013;10(2):115–120. doi: 10.4306/pi.2013.10.2.115. [DOI] [PMC free article] [PubMed] [Google Scholar]