

Introduction
Metastatic carcinoma to the eye and ocular adnexa from pancreas are extremely rare as a first indication of such a disease. Majority of these cases arise subsequent to the discovery of the primary tumour. Metastatic orbital tumour are further less frequently encountered than intraocular metastases [1]. We present a case of a unilateral proptosis in an apparently healthy middle aged male without any symptom suggestive of pancreatic malignancy.
Case Report
A 52-year-old-male presented with one month history of gradually increasing proptosis and impaired vision of the left eye. On examination a small smooth surfaced firm mass was palpated over the medial canthus displacing the left eye ball downward and outward. It was slightly tender and vision was 6/18. Fundoscopy revealed papilloedema. Routine biochemical and haematological investigations were within normal limits except marginally high total leucocyte count of 12,800 per cmm with 74% neutrophils in differential count. A clinical diagnosis of inflammatory orbitopathy was made and the patient was treated with a course of antibiotic and steroid to which he partially responded. He reported after two months with further deterioration of his vision and progressively protruding left eye ball. Computerised tomography scan of left orbit revealed a retrobulbar mass almost of the size of an eye ball [Fig 1]. The possibility of secondaries from a malignancy elsewhere was entertained. FNAC of the mass revealed poorly differentiated adenocarcinoma.
Fig. 1.

CECT scan of orbit showing a homogeneously enhancing extraocular intraorbital mass with an irregular margin and associated proptosis.
Detail ultrasound studies of the abdomen revealed a small well defined hypodense mass near head of the pancreas and a solitary metastasis in the liver. However radiography of the chest was normal. Ultrasound guided FNAC from the pancreaic lesion revealed loosely cohesive and dissociated neoplastic cells in richly cellular aspirate with a few inflammatory cells in the background [Fig 2]. Cellular features showed high nuclear cytoplasmic ratio, anisonucleosis, presence of extreme nuclear enlargement with nuclear contour irregularities in the crowded cells [Fig 3]. Prominent nucleoli and unevenly distributed chromatin viewed with overall context was in favour of poorly differentiated adenocarcinoma pancreas. Subsequent investigations revealed direct positive serum bilirubin level 2 mg/dl and alkaline phosphatase 30 KA unit/dl. Carcinoembryonic antigen level was raised, however no lesion was seen in the gastrointestinal tract.
Fig. 2.

Photomicrography of the pancreatic aspirate showing loosely cohesive and dissociated neoplastic cells of poorly differentiated adenocarcinoma
Fig. 3.
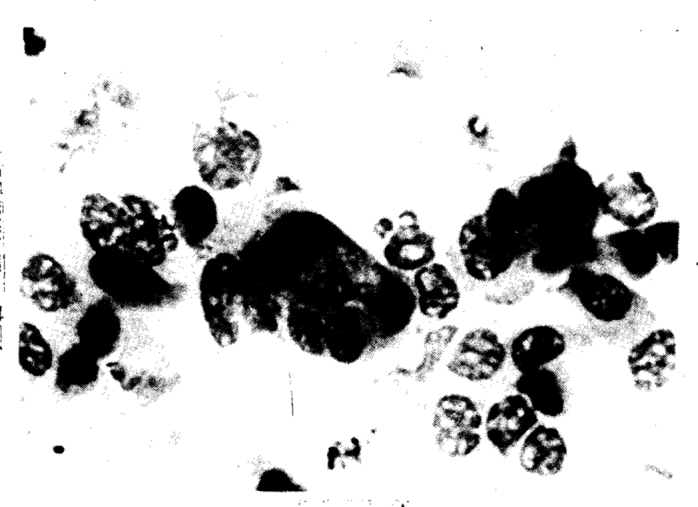
Photomicrography of the same aspirate shown in Fig. 2 in higher magnification (x 60) showing extreme nuclear enlargement with irregular nuclear contours, anisonucleosis, prominent nucleoli and unevenly distributed chromatin
Discussion
The most common primary lesion in cases of metastatic carcinoma to the eye and orbit are reported from the breast in female and the lung in male [2, 3, 4]. The pancreatic carcinoma are known to show distant metastases and sometimes manifest as secondaries from unknown primary site. Distant metastases include blood borne tumour emboli carried by the branches of internal carotid to ophthalmic artery and subsequently embolisation to the eye [5]. Sometimes the pulmonary metastases escape the detection due to the small sized tumour emboli which bypass the lungs as it happened in this case.
The earliest sign of metastasis to the eye is usually the development of unilateral proptosis. Bilateral involvement is sometimes reported in cases of metastases from carcinoma breast [1, 5]. Proptosis may be associated with periorbital oedema, impaired vision or pain. Presenting symptom of pain occurs in cases with tumour necrosis simulating inflammatory orbitopathy which misleads and delays further investigations [6] as occurred in our case. Papilloedema, ophthalmoplegia and secondary glaucoma are the rare manifestations due to the pressure effect of the tumour in the orbit and involvement of the optic nerve. In 46% of the patients in a clinicopathological study conducted by Ferry and Fond [5] ocular symptoms developed before it was recognised that the patients were harbouring the primary tumour elsewhere in the body.
Metastatic carcinoma to the eye and ocular adnexa from the pancreas are undoubtedly rare clinical entity as the tumour cells get arrested in the pulmonary capillaries before reaching the eye.
REFERENCES
- 1.Duke-Elder S, MacFaul PA. The Ocular adnexa (Vol XIII) In: Sir Duke-Elder. System of Ophthalmology. London: Henry Kipton. 1974:1144–1146. [Google Scholar]
- 2.Rosai J. Eye and ocular adnexa. In: Ackerman S, editor. Surgical Pathology. 18th ed. Mosby-Year Book Inc.; New York: 1996. p. 2502. [Google Scholar]
- 3.Merrill CF, Kaufman DI, Dimitrov NV. Breast cancer metastases to the eye is a common entity. Cancer. 1991;68:623–627. doi: 10.1002/1097-0142(19910801)68:3<623::aid-cncr2820680330>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 4.Freedman MI, Folk JC. Metastatic tumours to the eye and orbit. Patient survival and clinical characteristics. Arch Ophthalmol. 1987;105:1215–1219. doi: 10.1001/archopht.1987.01060090073031. [DOI] [PubMed] [Google Scholar]
- 5.Ferry A, Font R. Carcinoma metastatic to the eye and orbit. Arch Ophthalmol. 1974;92:276–286. doi: 10.1001/archopht.1974.01010010286003. [DOI] [PubMed] [Google Scholar]
- 6.Ferry AP. Metastatic carcinoma of the eye and ocular adnexa. Int Ophthalmol Clin. 1967;7:615–658. [PubMed] [Google Scholar]