

Introduction
Tuberculous peritonitis is a common form of abdominal tuberculosis. It is quite common in developing countries and its incidence is increasing in western countries. Also being seen is an increase in the atypical forms of tuberculosis, exotic presentations and rare clinical patterns of tuberculosis. Here we report one such presentation of peritoneal tuberculosis (TB) detected for the first time in a hernial sac.
Case History
A 60-year-old male presented with a painless, progressive swelling in the right groin of 6 months duration, which was reducible manually and on lying down. There were no features of obstruction or incarceration at any time. There were no abdominal or any other systemic complaints. He gave history of painful swelling in the right groin in his childhood, which had been incised leading to a purulent discharge for a few days, followed by gradual healing. No other relevant past or personal history was obtained. There was no history suggestive of pulmonary tuberculosis.
On general examination he was found to be moderately built and nourished, there was no pallor, clubbing or lymphadenopathy and the vitals were normal.
Local Examination revealed a 6 × 6 cm spherical swelling over the lateral half of the right inguinal ligament, 2 cm medial to the anterior superior iliac spine, extending upto the mid inguinal point. The consistency was soft and the surface was smooth. The swelling was reducible, with prominent cough impulse. A puckered scar was visible over the swelling. On lying down and reducing the swelling, a 3 x3 cm well defined defect was palpable lateral to the midinguinal point.
The abdomen was soft, nontender. There was no palpable organomegaly and no free fluid in the abdomen. Examination of the scrotum was normal. Rest of the systemic examination was normal.
Investigations revealed Haemoglobin of 12.6 gm/dl. TLC 8600/cmm. Blood sugar F: 90 mg/dl PP:133 mg/dl, ECG:WNL, ESR:22mm in 1 hr (Westergren method). Chest radiograph did not show any abnormality.
A diagnosis of incisional hernia in the right groin was made and he was taken up for anatomical repair of the hernial defect.
An 8 cm incision was made parallel to and above the inguinal ligament. The old scar was excised. The hernial sac was identified and freed all around from the external oblique aponeurosis and the conjoint muscles. The deep ring was identified just medial to the neck of the sac. The sac was freed till the defect was well delineated all around. The sac was opened. The inner surface of the sac was studded with multiple small yellowish white tubercles. A similar appearance was noted on the visible bowel serosal surfaces. The redundant sac was excised and the neck closed. Double breasting using No 1 Prolene was used to close the musculoaponeurotic defect and the skin closed with interrupted silk sutures.
Postoperatively patient developed a seroma, which required prolonged and repeated aspiration before it finally cleared up.[1
Histopathological examination of the excised sac revealed active tuberculous granulomas and a diagnosis of tuberculous peritonitis was made (Fig-1).
Fig. 1.
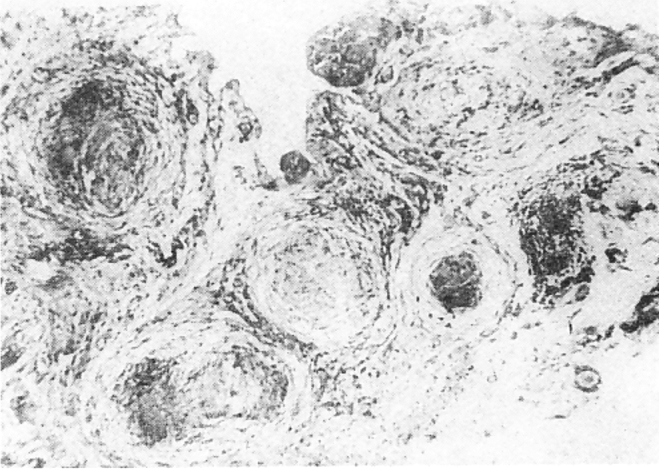
Photomicrograph showing infiltration of excised hernial sac by numerous tubercular granulomas.
Patient was started on standard antituberculous treatment. His condition improved and he was asymptomatic with well-healed operative scar at two months of follow-up.
Discussion
Tuberculous peritonitis is a common clinical problem in India and other developing countries. It is generally associated with a focus of tuberculosis elsewhere and is usually secondary to hematogenous dissemination. It can also occur as a-form of reactivation tuberculosis [2].
It is usually a disease of the young, average age at diagnosis being 36.5 yrs while our patient presented at 60 yrs of age [3]. Symptoms may rarely be subtle. Usually 70% of patients may have had symptoms for 4 months or more. Fever is present in nearly 66% of patients. Abdominal pain, swelling and weight loss are other common features. Our patient was unusual in presenting only with an indolent groin swelling. Common physical findings are abdominal distention, doughy feel of abdomen, omental mass and ascitis, none of which were found in our patient. Chest X-ray is abnormal in 80% of patients. Biopsy of peritoneum usually confirms the diagnosis.
In one study of 820 patients of abdominal tuberculosis, peritoneum was involved in nearly 30% of all patients [4]. Inspite of extensive investigational facilities available, diagnosis of abdominal tuberculosis can still be elusive and many patients are subjected to a laparotomy and other lesser procedures for definitive diagnosis [5].
TB peritonitis discovered for the first time in a hernial sac is an extremely rare presentation. Extensive literature search revealed only anecdotal report [6]. A case of incarcerated inguinal hernia due to underlying intestinal tuberculosis has been reported from Sao Paulo, Brazil [7].
In the case under discussion the first operation in childhood was perhaps an incision and drainage for an inguinal abscess. The postoperative seroma was a feature of the underlying tuberculous peritonitis, which resolved promptly with initiation of anti-tuberculous drugs. In this otherwise asymptomatic old man, there was no clue to suggest a preoperative diagnosis of peritoneal tuberculosis. What seemed to be a straightforward case of an incisional hernia was revealed at surgery to be lurking, otherwise unmanifest peritoneal tuberculosis. This highlights the fact once again, that abdominal tuberculosis, though so common in India, continues to present in myriad ways and at times takes the surgeon by surprise.
REFERENCES
- 1.Hiyama DT, Bennion RS. Peritonitis and intraperitoneal abscess. In: Zinner MJ, Schwartz SI, Ellis H, editors. Maingot's abdominal operations 10th ed. Prentice Hall International Inc; 1997. pp. 633–651. [Google Scholar]
- 2.Cromartis RA. Tuberculosis peritonitis. Surg Gynaec Obstet. 1977;144:875–876. [Google Scholar]
- 3.Underwood MJ, Thompson MM, Sayers RD. Presentation of abdominal tuberculosis to general surgeons. Br J Surg. 1979;10:1077–1079. doi: 10.1002/bjs.1800791030. [DOI] [PubMed] [Google Scholar]
- 4.AlKarawi MA, Mohammed AE, Yasawy MI. Protean manifestations of gastrointestinal tuberculosis: Report on 130 patients. J Clin Gastroenterol. 1995;20:225–324. doi: 10.1097/00004836-199504000-00013. [DOI] [PubMed] [Google Scholar]
- 5.MJ Joshi Tuberculosis. In: Surgical diseases in the tropics. Macmillan India Ltd 1992:3-51
- 6.Taylor BA. Tuberculosis peritonitis presenting in a hernial sac. JR Coll Surg Edin. 1986;31:313–315. [PubMed] [Google Scholar]
- 7.Faccin M, Youssef SR, Mozetic V. Inguinal hernia incarceration as a form of intestinal tuberculosis. Rev Paul Med. 1996;114:1097–1099. doi: 10.1590/s1516-31801996000100007. [DOI] [PubMed] [Google Scholar]