

Abstract
Leiomyomas of the bladder constitute <0.5% of all bladder tumors, with about 250 cases reported. Most patients present with urinary frequency or obstructive urinary symptoms. There are rare cases with other presentations, such as dyspareunia. We report a 22-year-old female who presented with complaints of pelvic discomfort, dysuria, and dyspareunia. Imaging and cystoscopy showed a protruding bladder lesion, which was excised through a transurethral resection. The pathologic diagnosis was bladder leiomyoma. Although being a benign condition, they can cause several different symptoms and should be early diagnosed and treated.
Keywords: Dyspareunia, leiomyoma, urinary bladder neoplasms
INTRODUCTION
Benign tumors of the bladder are rare, and leiomyomas represent <0.5% of the cases, with about 250 reported cases worldwide.[1,2,3]
Although it may be asymptomatic in about 20% of the cases, the majority presents with obstructive voiding symptoms or irritative urinary symptoms. The literature describes rare cases with distinct clinical presentation, as dyspareunia.[4,5] For diagnosis, cystoscopy and ultrasound examinations are the most frequently performed. Treatment consists of surgical removal of the tumor, and the prognosis is excellent. The authors describe a case of a young woman with bladder leiomyoma detected in what seemed a case of vaginitis.
CASE REPORT
The patient, a 22-year-old female, with no significant previous medical history, presented to her family doctor with complaints of pelvic discomfort, dysuria, and dyspareunia, for the last 3 months. At the time of consultation, she also notes a whitish odorless vaginal discharge. She denied any episodes of fever, low back pain, menstrual disorders, vulvar symptoms, or changes in urine. The gynecological examination showed sparse, whitish airy leukorrhea, with no visible lesions on the cervix. The pelvic bimanual examination caused pain with the mobilization of the cervix and adnexal regions. She was empirically treated with metronidazole vaginal suppository id for 7 days and azithromycin 1 g single dose. A pelvic ultrasound (bladder and gynecologic), urinalysis, and urine culture were requested.
The gynecologic ultrasound showed only a small amount of fluid in the endocervical canal with a thickness of 1.2 mm, and ovaries of normal morphology and dimensions, with some bilateral cystic structures of probable functional nature. The bladder ultrasound described a little vaguely nodular thickening area in the anterior wall, of relatively regular contour measuring 9 mm × 4 mm. The urinalysis and urine culture were both unremarkable. Considering these results and the clinical improvement observed, it was decided to perform a new pelvic ultrasound in 2 months. Meanwhile, the patient went to the emergency department with complaints of dysuria, pollakiuria, and urinary urgency. These symptoms were interpreted as cystitis, and a single dose of fosfomycin was empirically prescribed.
The new bladder ultrasound, performed 2 months after the first one, showed a hypoechoic nodule on the anterior wall, measuring 16 mm × 11 mm × 6 mm, with regular contours, well-defined limits and homogeneous texture, compatible with benign lesion.
The patient was referred to the urology consultation. About 2 months after this referral and 1 month before the urology consultation, the patient went again to the emergency service with complaints of dysuria and pollakiuria, with a urine dipstick analysis compatible with cystitis and having been prescribed norfloxacin.
Following the urology consultation, the patient underwent cystoscopy, which revealed a lesion protruding into the bladder lumen. A transurethral resection of the bladder was scheduled and performed in 2 months, and it went with no complications. The anatomopathological analysis established the diagnosis of bladder leiomyoma [Figures 1 and 2]. The patient was evaluated after a month and considering she was asymptomatic; she was discharged from the urology consultation.
Figure 1.
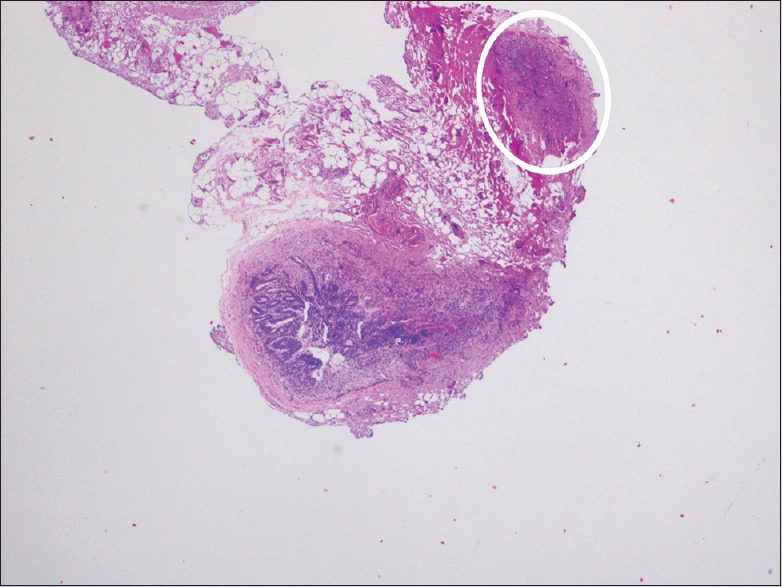
Leiomyoma with typical intersecting smooth muscle fascicles, circled in white (×20)
Figure 2.
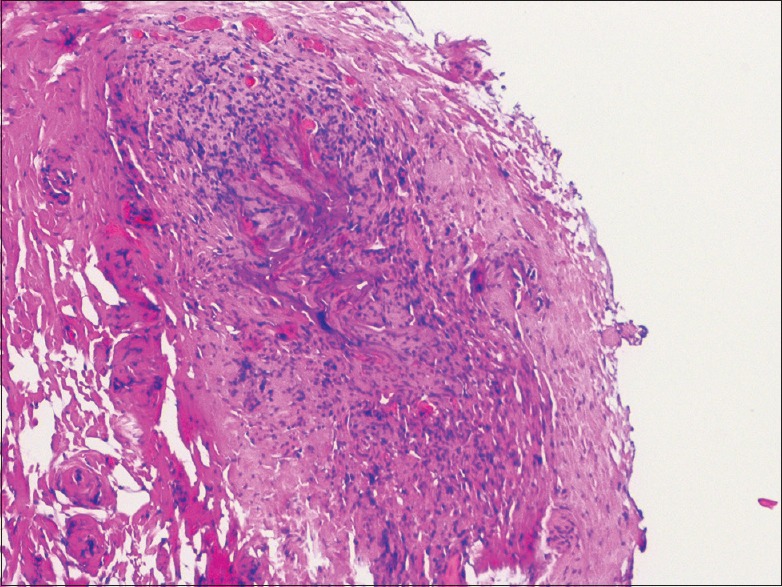
Detail of the tumor showing a proliferation of spindle-shaped cells and eosinophilic cytoplasm with no atypical mitotic figures (×100)
About 2 weeks after the hospital discharge, the patient went to her family doctor with complaints of dysuria and suprapubic and low back pain, which persisted since the date of discharge, with progressive worsening. She was apyretic and had a negative renal Murphy's punch sign (or Pasternacki's sign). A urine culture was ordered before empirical antibiotic therapy with fosfomycin, but the patient failed to do it. To this date, the patient remains asymptomatic.
DISCUSSION
Leiomyoma is a benign smooth muscle tumor that can occur in any organ.[5] In the urinary system, the location is more frequent in the bladder, being the most common benign mesenchymal tumor of this organ. Nonetheless, they only represent <0.5% of all bladder cancers.[2,3] In a review by Khater and Sakr in 2013, there were only 250 cases previously reported and since then six more cases were reported.[2,5,6,7,8,9] There is a female preponderance (70%), and this pathology affects those in their third to sixth decades, with a mean age of 44 years.[2,6,7] However, there are cases described in younger patients, as is the case with our patient.
These tumors can be endovesical, intramural, or extravesical. The endovesical tumors are the most common and usually present with dysuria, urinary urgency, hematuria, and sometimes with low back pain. Some tumors are pedunculated and can manifest through urinary retention.[3,4]
Regarding the diagnosis, bladder ultrasound is the imagiologic examination that detects more often these tumors. In most cases, it shows a small mass with a solid aspect, homogeneous, and hypoechoic encapsulated by a hyperechogenic thin blade.[2] Cystoscopy shows the presence of a sessile tumor not arborescent and protruding into the bladder lumen computed tomography, and magnetic resonance imaging (MRI) can be performed to obtain further information on the size and location.[6] MRI is the preferred method for the composition and relation to plans of the bladder wall. Despite the imaging characteristic features, the definitive diagnosis is histopathology.[3]
The treatment of the leiomyoma is surgical, and the approach depends on the location and size of the tumor. In most cases, the transurethral route is the preferred although in some tumors, as in larger, involving the entire bladder wall, in a not propitious position or difficult to recognize, a segmental resection or laparoscopic partial cystectomy might be necessary.[2,10] Surgical complications are described almost exclusively in the larger urethral tumors. The prognosis is invariably favorable, with relief of complaints in symptomatic patients. The recurrence is rare.[3,7]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors would like to thank Hugo Antunes from the Department of Urology and Renal Transplantation and Rui Almeida and Carol Marinho from the Department of Anatomic Pathology of the Coimbra Hospital and University Centre, for their contributions to this case report.
REFERENCES
- 1.Carvalho TG, Botelho F, Resende A, Portugal R, Guimarães M, Silva J, et al. Leiomyomas of the bladder and urethra - two clinical cases. Acta Urol. 2010;27:51–4. [Google Scholar]
- 2.Khater N, Sakr G. Bladder leiomyoma: Presentation, evaluation and treatment. Arab J Urol. 2013;11:54–61. doi: 10.1016/j.aju.2012.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pardal H, Ferronha F, Gameiro C, Vilas-Boas V, Galego P, Melo P, et al. Intramural vesical leiomyoma in a patient with a pelvic fibrous tumour - case report. Acta Urol. 2011;2:28–31. [Google Scholar]
- 4.Kim IY, Sadeghi F, Slawin KM. Dyspareunia: An unusual presentation of leiomyoma of the bladder. Rev Urol. 2001;3:152–4. [PMC free article] [PubMed] [Google Scholar]
- 5.Xin J, Lai HP, Lin SK, Zhang QQ, Shao CX, Jin L, et al. Bladder leiomyoma presenting as dyspareunia: Case report and literature review. Medicine (Baltimore) 2016;95:e3971. doi: 10.1097/MD.0000000000003971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Silva-Gutiérrez A, Martínez-Méndez ME, González-Romo MA, Nava-Jácome O, Castillo-Zurita O, Morales-Díaz J, et al. Bladder leiomyoma. Rev Mex Urol. 2013;73:43–5. [Google Scholar]
- 7.Ortiz M, Henao DE, Cardona Maya W, Ceballos MM. Leiomyoma of the urinary bladder: A case report. Int Braz J Urol. 2013;39:432–4. doi: 10.1590/S1677-5538.IBJU.2013.03.18. [DOI] [PubMed] [Google Scholar]
- 8.Wu S. Imaging findings of atypical leiomyoma of the urinary bladder simulating bladder cancer: A case report and literature review. Med Ultrason. 2013;15:161–3. doi: 10.11152/mu.2013.2066.152.sw1. [DOI] [PubMed] [Google Scholar]
- 9.Jain SK, Tanwar R, Mitra A. Bladder leiomyoma presenting with LUTS and coexisting bladder and uterine leiomyomata: A review of two cases. Rev Urol. 2014;16:50–4. [PMC free article] [PubMed] [Google Scholar]
- 10.Jeschke K, Wakonig J, Winzely M, Henning K. Laparoscopic partial cystectomy for leiomyoma of the bladder wall. J Urol. 2002;168:2115–6. doi: 10.1016/S0022-5347(05)64309-1. [DOI] [PubMed] [Google Scholar]