

Abstract
The measurement of root canal length is a pre-requisite for successful pulpectomy. The conventional manual and radiographic methods are not very accurate. In the present study, odontometer was used [Group B) to assess its efficacy over the conventional methods (Group A) for recording root canal length. In group A, 36 teeth were treated with pulpectomy while in group B, 51 teeth were managed by the same treatment. It was observed that post operative complications in group B were significantly less (p < 0.05). The odontometer proved to be an excellent device for rapid and accurate measurement of root canal length.
KEY WORDS: Pulpectomy, Root canal length, Odontometer
Introduction
At present the modalities being used for the measurement of root canal length are radiographs and tactile sensation. With radiographs an accurate estimate is difficult, especially in curved canals. Feeling the apex with an instrument (tactile) requires skill, experience and cannot be considered absolutely accurate. Various electronic devices used to measure the exact length of the root canal have been introduced into the endodontic practice in the last few years [1, 2, 3, 4, 5]. The odontometer is one such device which identifies different tissues of the tooth and surrounding structures depending upon difference in their electrical impedance. It is also used for effective treatment of hypersensitive teeth and application of other oral medications by iontophoresis. This study compares the clinical utility of odontometric vis-a vis manual and radiological measurements of root canal length.
Material and Methods
In the present study 169 teeth from 126 patients which required conservative treatment were included. These patients reported to the department of Dental Surgery, Armed Forces Medical College, Pune for treatment. A total 87 teeth out of these were treated with pulpectomy, 36 in group ‘A’ and 51 in group ‘B’. The root canal length in group A was measured by conventional techniques whereas odontometer was used for this purpose in group B.
All patients were examined and treated in anatomical dental chair under sharp halogen light.
For recording root canal length in group A, following techniques were used : (i) A reamer was inserted to detect the apex by feel of operator's fingers or the patient's complaint of pain, (ii) A periapical intra-oral x-ray taken with a reamer inserted into the canal and then the length of the root canal was estimated by establishing a ratio between the length of the tooth over the length of the reamer inserted with the lengths found on the film. A rubber stopper was used to mark the length on the reamer.
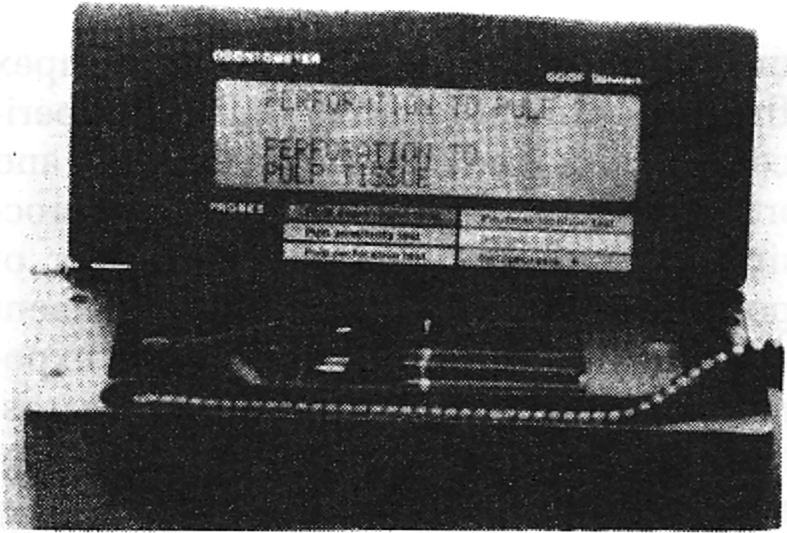
In group B odontometer was used for measuring length of the root canal. The display reading which are seen on the odontometer are “ready”, “apical foramen”, “pulp tissue”, dentine”, “apical pulp tissue”, “apical constriction”, and “stop/through foramen”. As soon as the odontometer is opened, the apparatus starts an internal test cycle. In a few seconds display signals “ready” (Fig. 1). Specific probe was selected and it was connected to the plug on the coiled lead. The black plug was connected to the neutral oral mucosa and placed in the saliva moist area, and this electrode was used for all applications. For recording the length of the root canal, it was dried until a paper point was moist only at the tip because the odontometer does not function accurately in moist canal. The area around the crown was dried for electrometric recording. The odontometer was started by placing the neutral mucosa electrode and by connecting the red coloured test clip. The test clip was attached to the root canal instrument. The root canal instrument was then inserted into the canal until required “apical region” was shown on display. The exact working length was thus measured.
Fig. 1.

Display “READY” indicates connect the probe.
The irrigants used for pulpectomy were 5% sodium hypochlorite solution and hydrogen peroxide. Intra-canal medicaments for inter treatment dressings used were cortisone antibiotic combinations and the sealing agent used was provi paste. The root canals were filled with gutta percha points with endomethasone.
Pre and post operative radiological examination was carried out in all cases.
Results
Table 1 reflects the details of post operative complications as observed on the following day, after one week, 12 weeks and 24 weeks. It can be seen that 13 teeth (36.1%) out of 36 teeth in Group A developed post operative complications on the following day, whereas only one tooth in group B out of 51 teeth had pain (p < 0.05). After one week, eight teeth (22.22%) out of 36 teeth in group A persisted with complications after being prescribed antibiotics and analgesics, compared to only one tooth (p < 0.05) in group B. One tooth out of eight teeth in group A was retreated with apicoectomy while the remaining 7 teeth of this group were retreated by pulpectomy. Similarly, one tooth with complications in group B was retreated with pulpectomy. Two teeth in group A were extracted at emergency visits while only one tooth needed extraction in group B at 12 weeks follow-up visit. At 24 weeks post operative review, no teeth in any of the groups had any complications.
TABLE 1.
Assessment of post operative complications in teeth treated with pulpectomy
| Complications | Following day | One week | 12 weeks/24 weeks | |||
|---|---|---|---|---|---|---|
| Group A | Group B | Group A | Group B | Group A | Group B | |
| Pain | – | 1 | – | – | – | – |
| Discomfort | 1 | – | – | – | – | – |
| (2.78) | ||||||
| Pain, discomfort, tenderness | 8 (22.22) | – | 5 (13.89) | – | – | – |
| Discomfort, tenderness | 4 (11.11) | – | – | – | – | – |
| Pain, discomfort, tenderness, abscess | – | – | 3 | 1 | 2* | 1$ |
| (8.33) | (1.96) | (5.56) | (1.96) | |||
| Total teeth with complications | 13 | 1 | 8 | 1 | 2 | 1 |
| (36.11) | (1.96) | (22.22) | (1.96) | (5.56) | (1.98) | |
| No complaints | 23 | 50 | 28 | 50 | 34 | 50 |
| (63.89) | (98.04) | (77.78) | (98.04) | (94.44) | (98.04) | |
| Total | 36 | 51 | 36 | 51 | 36 | 51 |
| p < 0.05 | p < 0.05 | p > 0.05 | ||||
Extracted at emergency visit before 12 weeks review; $ Extracted al 12 weeks review: Figures within parenthesis indicate %.
Extracted al 12 weeks review: Figures within parenthesis indicate %.
Discussion
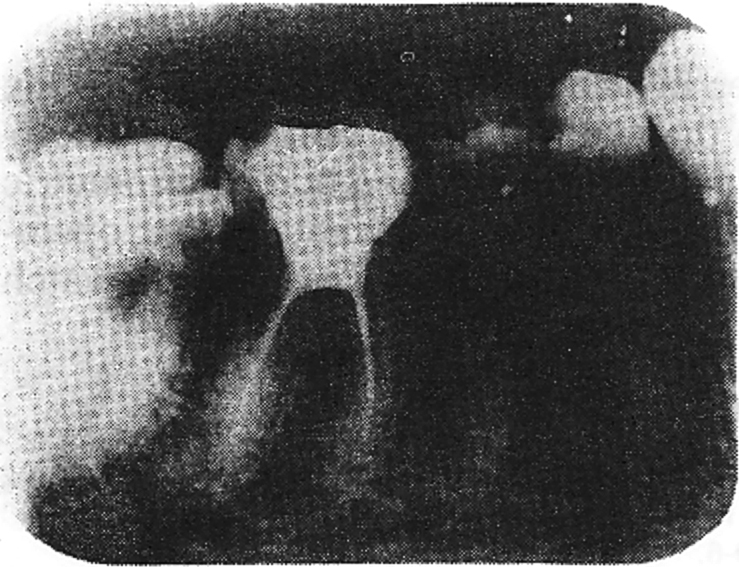
There is significant difference (p < 0.05) between group A and B as regards occurrence of complications at the post operative review on the following day and also at one week's review indicating higher failure rate of root canal treatment in group A. The length of root canal could not be properly obturated in group A as is evident from post operative periapical x-ray films (Fig. 2). These improper fillings were observed more in posterior teeth than anterior. In group B in which odontometer was used, root canals could be completely obturated (Fig. 3). The odontometer was also of great help to show perforation of pulp tissue on screen (Fig. 4). At post operative review on following day, patients with complications in treated teeth were prescribed antibiotics and analgesics. There after if complications persisted and abscess formed, pulpectomy was redone in posterior teeth whereas apicoectomy was done in anterior teeth. The teeth which did not respond to retreatment were extracted. As evident from the results of the present study (Table 1), no fresh complications were observed after 12 weeks review. There is therefore no requirement of a prolonged review of 24 weeks.
Fig. 2.
Lack of apical approximation resulls in incomplete obturation.
Fig. 3.

Complete obturation of root canals.
Fig. 4.
Odontometer indicating perforation into pulp tissue.
Development of more complications in group A than B as discussed above, points to the fact that odontometer is quite efficient for planning and executing pulpectomy. For the pulpectomy, to be successful, it is imperative that a proper root canal length is recorded, prior to its obturation, This is the key factor for success of root canal therapy. The tactile sensation gives rise to excessive variance in measurement due to inherent error in “feeling your way down” a canal [1]. Feeling the apex with an instrument requires skill and experience and cannot be considered accurate and moreover is time consuming in terms of processing the radiographs and the number of exposures required for accurate measurement of the length of roots canals. Repeated exposure to radiation presents additional hazards. Moreover the exact location of the apical foramen still cannot be determined with certainty by radiographs as the foramen most often emerges at the side of root at varying distances from the radiographic apex, but this variation can range from 0 to 5 mm [2]. The odontometer helps in accurately determining the root canal length through perception of an auditory tone thus eliminating the drawbacks of the earlier methods used for measuring the length of the involved root canal. Most of the workers [3, 4, 5, 6] feel electrometric devices specially the audio type are more reliable and quicker in determining the correct working length than conventional radiographs. However, Inouse [1] mentioned that electrometric devices too have a disadvantage that operator's attention is distracted as he has to watch the meter constantly.
REFERENCES
- 1.Inouse N. An audiometric method for determining the length of root canals. J Can Dent Assoc. 1973;39:630–636. [PubMed] [Google Scholar]
- 2.Dehlin Electrometric measuring of apical foramen. Quintessence International. 1979;1:13–22. [PubMed] [Google Scholar]
- 3.O'Neill LJ. A clinical evaluation of electronic root canal measurement. Oral Surg. 1974;38:469–473. doi: 10.1016/0030-4220(74)90376-4. [DOI] [PubMed] [Google Scholar]
- 4.Sunada L. A now method for measuring the length of the root canal. J Dent Res. 1982;41:375–387. [Google Scholar]
- 5.Ushiyma M. New principle method for measuring the root canal length. J Endo. 1983;9:97–104. doi: 10.1016/S0099-2399(83)80105-8. [DOI] [PubMed] [Google Scholar]
- 6.Bramante CM, Barbet A. A critical evaluation of some methods for determining tooth length. Oral Surg. 1974;37:463–473. doi: 10.1016/0030-4220(74)90122-4. [DOI] [PubMed] [Google Scholar]