

Abstract
Return-to-play from injury is a complex process involving many factors including the balancing of tissue healing rates with the development of biomotor abilities. This process requires interprofessional cooperation to ensure success. An often-overlooked aspect of return-to-play is the development and maintenance of sports specific conditioning while monitoring training load to ensure that the athlete's training stimulus over the rehabilitation period is appropriate to facilitate a successful return to play. The purpose of this clinical commentary is to address the role of energy systems training as part of the return-to-play process. Additionally the aim is to provide practitioners with an overview of practical sports conditioning training methods and monitoring strategies to allow them to direct and quantify the return-to-play process.
Level of Evidence
5
Keywords: Acute/chronic workload, energy system development, return-to-play, sports rehabilitation, strength and conditioning, training load
INTRODUCTION
Injury is an unfortunate outcome for some of those involved in sports. An estimated seven million Americans receive medical attention for sports related injuries each year.1 Once an athlete sustains an injury it is important that they progress through a focused rehabilitation program to allow them to return to their previous level of competition. This process has been termed the return to sport continuum and is separated further into three distinct phases (Figure 1).2 The approach taken during this transition from injury to full participation is critical in preparing the athlete for competition at a high level while also reducing the risk of re-injury.3 Unfortunately, the return-to-play (RTP) approach is not always handled in a systematic way. This can lead to a delay in the athlete's RTP, leaving the athlete underprepared for the demands of sport with increased risk of re-injury or decreased performance upon return.4-6
Figure 1.

Return to Play Continuum.
The RTP process is a multi-disciplinary venture including sports physicians, physical therapists, athletic trainers, strength and conditioning coaches, and sport coaches. Collectively, these professionals as well as the athletes themselves all play a role in the decision making process.2,7 Communication amongst these groups is paramount in optimizing athletic care and ensuring the best possible outcomes.2,5 However, the criteria used to gauge progress are often vague and lack standardization.8 As a result communication during the RTP process can be compromised. In some instances a standard of practice is used that focuses on local tissue adaptations based on healing time frames.8,9 While a time based approach does improve communication, Herrington and colleagues make a strong argument that this is insufficient and a task-based approach that focuses on clearly defined performance goals is the best approach for RTP.9 Thus it is important that the language that is used in describing the RTP process is familiar to everyone involved, is measurable, and reflects best practices.
As an athlete recovers, the emphasis progresses from protecting the injured tissue, to guiding the healing process, and finally into restoring the capacity of strength and energy systems. However, this restoration of strength and capacity may not be fully realized during the athlete's rehabilitation.10 In the best-case scenario, an athlete will be “medically cleared” to play using RTP algorithms (e.g., muscle strength, joint range of motion, a series of performance tests, etc.), which have been shown to be of value in making this decision.11 However, even these approaches typically give very little information regarding how much training the athlete has performed or whether their fitness is sufficient to tolerate competition at a high level.12,13 Better documentation of the training process during RTP allows for the quantification of workload, providing direction to the program and enhancing communication. This need for an assessment of the workload performed in the RTP process and its potential link to re-injury was recently listed as a key focus area by the 2016 Consensus Statement on Return to Sport from the First World Congress in Sports Physical Therapy, Bern.2
To address some of these concerns several authors have proposed RTP frameworks, which can aide in discussions amongst the relevant practitioners.4-7 For example, the updated Strategic Assessment of Risk and Risk Tolerance (StARRT) framework breaks the decision making process down into three parts: 1) the assessment of health risk, 2) the assessment of activity risk, and 3) the assessment of risk tolerance.4,6 Approaches like this establish a system that monitors the entire process while assigning each professional a role in clearing the athlete for RTP. None of the approaches referred to above have explicitly described an assessment of the athletes acute or chronic workload. However the authors of this paper find that the StaRRT framework suits this process well and propose that the assessment of workload should be included in each of the three categories laid out in the StaRRT framework.2,4,6 This will allow for a smooth transition from injury to medical clearance for RTP and on to return to performance while ensuring that the athlete has performed an appropriate amount of chronic loading to tolerate these progressions.5,6,12,14
It is typical that strength and conditioning is performed by “healthy” athletes.5 However, injured athletes also benefit from a training program that prevents detraining and helps to re-develop any biomotor adaptations lost during the initial rehabilitation process. This thought process has led various authors to propose a comprehensive approach to strength and conditioning within the RTP paradigm.5,14,15 The role of strength training within rehabilitation has been discussed elsewhere;14,15 but very little has been described regarding re-conditioning, or energy systems development during the RTP process. All of the bodies’ energy systems play a supporting role at the onset of activity thus any form of training can be used to promote energy system development. However, specific acute training variables such as mode of exercise, duration, intensity, and rest interval dictate the type of adaptations elicited.
Training and rehabilitation are complex processes that require sufficient monitoring to ensure that performance objectives are being met. The goal of the training process is to ensure that the training is progressed at the optimal pace and that the athlete is not under or over exposed to training loads.12 As such, all individuals involved in RTP decision-making process should have an understanding of the athlete's current level of fitness and its relation to their clearance for RTP.
The purpose of this clinical commentary is to address the role of energy systems training as part of the RTP process. Thus, an overview of the three metabolic pathways followed by energy system training concepts will be provided. Finally, practically applicable methods are given for monitoring the training process providing practitioners with tools to quantify the training result and direct the RTP process for the athlete.
ENERGY SYSTEM PHYSIOLOGY
Exercise places both metabolic and neuromuscular demands on the body16 and in order to meet these demands adenosine triphosphate (ATP) must be provided to working muscle through the interactions of the three metabolic pathways:16,17
The phosphagen system
The glycolytic system
The oxidative system
The intensity and duration of the exercise bout determines which of the energy systems has the greatest contribution to energy supply. Activities such as Olympic Weightlifing and the 100m sprint utilize ATP at a very high rate and therefore rely on the Adenosine triphosphate-Phosphocreatine (ATP-PCr) pathways to rephosphorylate ADP to ATP. This pathway relies on the single-step creatine kinase reaction to rephosphorylate ADP and thus has a high rate of energy supply. However, there is a finite supply of intramuscular ATP and PCr stores resulting in a very limited capacity of this system.
Intermediate duration activities such as 400m sprinting must rely on higher capacity energy systems to rephosphorylate ATP. This multistep pathway utilizes glucose/glycogen to provide ATP for continued muscular contraction and will so in the absence of oxygen. However, fatiguing by-products are produced, which limit the duration of this energy system. Longer duration activites such as marathon running rely on oxidative phosphorylation pathways (aerobic glycolysis/β-oxidation, Kreb's Cycle, electron transport chain) to sustain ATP production over the extended exercise duration. However, these pathways require the integrated delivery and utilization of oxygen and thus have substantially lower rates of ATP supply. Although not mutually exclusive, the proportional reliance on these three energy systems depends on both the duration and intensity of exercise (Table 1).
Table 1.
Energy System Demands
| Duration | Intensity | Primary Energy System |
|---|---|---|
| 0 – 6 seconds | Maximal | Phosphagen |
| 6 – 30 seconds | Near-Maximal | Phosphagen & Anaerobic Glycolysis |
| 30 – 120 seconds | High | Anaerobic Glycolysis |
| 2 – 3 minutes | Moderate | Anaerobic & Aerobic Glycolysis |
| > 3 minutes | Low | Oxidative |
Table 1 may serve to provide a general understanding of the metabolic demands of various sport activities. For example, the metabolic requirements of sports such as Olympic weightlifting, 100m sprinting, or Marathon running, are relatively easy to classify since the intensity and specific durations of these sports biases them towards the ends of the spectrum. The demands of many team sports, however, present a greater challenge when classifying them based on metabolic or energy systems demand. A majority of team sports are comprised of maximal or near maximal sprints followed by brief periods of recovery18 and therefore do not utilize the extremes of the energy system as in the previous examples. Descriptions of metabolic pathways, such as Table 1, make it appear as though these pathways are mutually exclusive with distinct ‘on-off’ switches as the duration increases and the intensity of work decreases. It should be noted that each of the systems works to supply energy in concert, however their relative contributions change depending on the task.19 As such, team sport athletes require fitness levels sufficient to support metabolic requirements specific to their sport and position that spans the three main metabolic pathways.
The “on and off”, intermittent nature of team sport has been termed repeated sprint ability (RSA).20,21 RSA reflects a key characteristic of team sport, whereby a large portion of competition is spent performing lower intensity activities with brief bouts of maximal to near maximal efforts interspersed throughout the time played.20 Thus, it is important that athletes participating in activities with high RSA demands possess the ability to repeat maximal or near maximal efforts with limited fatigue.17,20 As fatigue accumulates over the course of a competitive match the ability to repeatedly sprint at a maximal speed becomes compromised. Multiple mechanisms of fatigue have been explored within the construct of RSA.17,20,22,23 In addition, many acute training and competition variables have been studied as well. For example, decreased RSA due to fatigue may be attributed to duration, work-to-rest interval,24 type of recovery (active vs. passive),17,25 oxygen uptake kinetics26 and changes in muscle metabolites.27 While the physiological underpinnings of RSA continue to be explored it is important to note that a variety of training methods have been proposed to address these limitations and improve RSA.17,28 For example, high-intensity interval training (HIIT) methods have been shown to improve VO2max,29 VO2 kinetics,30 mitochondrial biogenesis,31,32 and sports performance.33,34
Energy system training terminology is not always consistent, which may result in confusion in the application of research principals to the actual training methods used.35 To alleviate this, Chamari and Padulo recommend doing away with physiological descriptions of training and instead propose three basic classifications for short duration – repeated effort exercise. This classification system can help practitioners develop training sessions without being confused or hindered by exercise physiology terminology. The classification system proposed by Chamari and Padulo are based on exercise duration and can be seen in Table 2.
Table 2.
Energy System Training Distribution
| Classification | Intensity | Duration | Programming Example |
|---|---|---|---|
| Explosive Efforts | Maximal | Up to 6 s | 3‐5 s work : 60‐120 s Rest |
| High Intensity Efforts | Maximal | 6 s to 1 min | 30 s work : 30 s Rest |
| Endurance Efforts | Maximal | > 1 min | 3 min work : 3 min Rest |
Note that longer duration exercise is not addressed within the classification structure of Chamari and Padulo; however, it should not be overlooked. While excessive amounts of long duration, endurance exercise may have deleterious effects on the explosive capabilities of power athletes36 a moderate amount of this type of conditioning has been found to increase performance in team sport competition as a major portion of team sport is spent performing low-intensity activities in-between high intensity efforts.37 During these periods, the aerobic energy system plays a central role in recovery between intense bouts of exercise and assists in repeating those high intensity efforts with less performance decrement.38-40 While the aerobic system may contribute 10% or less energy to a single sprint, with repeated sprints its contribution can rise to as much as 49%.38 For these reasons, a well-rounded training program should be designed to ensure that the full spectrum of the athlete's fitness is addressed within the RTP program.
TRAINING METHODS & PROGRAMMING
A determination of the individual needs of the athlete is important to ensuring that the testing done during the RTP process accurately assesses the demands that will be placed on them. This is done with a needs analysis of the sport and should be specific to the position the athlete plays as well as the level of competition they participate in (e.g., collegiate, amateur, professional). An in depth discussion of this processes is beyond the scope of this paper and the reader is referred to the following papers for an exploration of this topic in full.41,42 Numerous factors must be considered when deciding what to emphasize within training, such as the time since the initial injury, what has been done to date, and the time frame available before RTP. Communication between professionals involved in the RTP decision at this point will help to ensure that the RTP process is optimized.
The manipulation of acute training variables dictates the response the athlete has to the training program. Buchheit and Laursen23 recognize nine variables that can be manipulated within an energy system training session (Table 3). The manipulation of training variables can be used to change the focus of the session or to aid in selecting modalities (e.g., cycling, rowing) that may be appropriate during phases of the RTP process when activities like running are contra-indicated. These variables offer the practitioner a number of options for creating a training program. Table 4 provides guidelines for the manipulation of these variables based on the objectives of the training session (e.g., short duration or long duration) and training modalities that might be appropriate for the individual at that time. The clinician is advised to utilize this framework when designing programs.
Table 3.
Energy System Training Variables
| Segment of Training Session | Variable Manipulated |
|---|---|
| Work Interval | Intensity Duration Modality (e.g., Run, Bike, Rowing, etc.) |
| Recovery | Duration Intensity |
| Series: A group of sets performed in succession before a longer rest break is taken. | Number of Series Series Duration Time Between Series Between‐Series Recovery Intensity |
Table 4.
Energy System Training Parameters
| Work Interval | Recovery | Series | Adaptation | |||||
|---|---|---|---|---|---|---|---|---|
| Intensity | Duration | Intensity | Duration | Number of Series | Weekly Frequency | Timeframe | ||
| Short Duration – Repeated Efforts | ||||||||
| Explosive Effort | Maximal | <6 s | Passive | 30 to 120 s | 2 to 6 | 2 to 3 | 2 to 3 weeks | |
| High-Intensity Effort | Maximal | 15 to 30 s | RPE < 2 | 30 to 120 s | 4 to 10 | 2 to 3 | 2 to 3 weeks | |
| Endurance Effort | RPE 8 to 9 |
2-3 min | RPE < 2 | 2-3 min | 6 to 10 | 2 to 3 | 2 to 3 weeks | |
| Long Duration – Endurance | ||||||||
| Extensive | Zone 1 | 20-60 min | Continuous | 3 to 5 | 2 weeks to 3 months | |||
| Intensive | Zone 2 Zone 3 |
6-8 min 4-6 min |
Low Zone 1 |
2-4 min | 3 to 6 | 2 to 3 | 2 + weeks | |
When designing training programs, the practitioner is required to determine the appropriate training intensity for a given training session. Prescription of intensity has been based on of a number of physiological measures in the literature including maximal heart rate, VO2max, aerobic and anaerobic threshold, and critical power.43 Traditionally a percentage of these values are utilized to prescribe an internal (%VO2max, % threshold) or external (% critical power) intensity in either a continuous or interval-based prescription. With the popularity of interval-based prescriptions23 (see Training Methods & Programming) it is imperative that the practitioner not only considers the intensity of the exercise bout, but also the intensity of inter-interval recovery periods and inter-series recovery. Technology, such as GPS monitors, heart rate monitors, and power meters, may assist practitioners in directly quantifying training intensity, however, expense may limit their applicability in certain situations. The use of perceived intensity and duration make for an affordable solution that is easy to implement in any setting.
The rating of perceived exertion (RPE) is one of the most recognized measures for monitoring training intensity during a workout.44 Using this method clinicians may then prescribe exercise intensities within a binary or 3 zone model as shown in Table 5.44-47 The binary zone model differentiates low vs. high-intensity with respect to the first blood lactate threshold (2.5 mmol/L) or 72% HRmax, whereas the 3 zone model includes intensities below 2.5 mmol/L blood lactate or 55-82% HRmax as zone 1, 2.5 mmol/L to 4.0 mmol/L blood lactate or 82-87% HRmax as zone 2, and >4.0 mmol/L blood lactate and >87% HRmaz as zone 3.47 The RPE scale most often used is the modified CR10 scale seen in Table 7.45 These parameters offer a flexible model for developing both anaerobic and aerobic qualities in the injured athlete.
Table 5.
Sustained Effort Training Intensity Zones
| Binary Model | Intensity Zone | Heart Rate (Max) | RPE |
|---|---|---|---|
| Low Intensity | Zone 1 | 55 ‐ 82% | ≤ 5 |
| Zone 2 | 82 ‐ 87% | 5 ‐ 6 | |
| High Intensity | Zone 3 | 88 ‐ 99% | 7 ‐ 10 |
Table 7.
CR-10 Rating of Perceived Exertion
| Rating | Descriptor |
|---|---|
| 0 | Rest |
| 1 | Very Easy |
| 2 | Easy |
| 3 | Moderate |
| 4 | Somewhat Hard |
| 5 | Hard |
| 6 | |
| 7 | Very Hard |
| 8 | Very, Very Hard |
| 9 | Almost Maximal |
| 10 | Maximal |
The classification system established in Table 2 gives the practitioner a framework that can be used for designing and progressing the individual rehabilitation program. Key training sessions throughout the week would be designed to improve the predominant energy system demands required by the sport and position the athlete competes in. For example, the sport of American football is an intermittent sport comprised of repeated, high-intensity efforts of approximately 4 – 7s, followed by 15 – 80s of recovery, which would be considered “Explosive Effort” per Table 2.48-50 As such, the goal of the programming would be to maximize the various energy systems ability to tolerate these demands. Table 6 provides an example program demonstrating application of the various principals to a specific case. Training modalities should progress as the athlete moves through the RTP program. For example, the athlete may begin performing bike workouts, if running is initially contraindicated due to their injury, and then progress to linear running, change of direction running, and finally to open environment skill work, where the athlete must sprint at a high level whilst making decisions and changing directions. Similarly, exercise intensity would progress from lower intensity work to explosive efforts of straight ahead running, to change of direction work performed under similar work-to-rest ratios specific to the game. Finally, the athlete's program would be progressed from longer rest intervals to rest intervals that are more sport specific.
Table 6.
Sample Basketball Sports Specific Training Progression after Injury to Lower Extremity (LE)
| Phase | Phase 1 Long Duration ‐ Endurance | Phase 2 Long/Short Duration | Phase 3 Short Duration – Repeated Effort |
|---|---|---|---|
| Training Parameters | 30 min Extensive work | Intensive efforts progressing to Endurance effort | Endurance effort alternated with High Intensity and Explosive Effort |
| 3‐5 Intensive Bouts | May still include extensive work for LE | ||
| Modality Used | Initially this will be regulated to activities that do not stress the injury. | At this point the exercise selection may begin to include LE based activities as deemed appropriate by medical staff. | The LE should be fully integrated assuming clearance with the goal being to match RTP demands. |
| Progression | Progression is based on medical clearance and adaptations as determined by relevant tests. | ||
MONITORING THE PROCESS
Monitoring the training process provides practitioners with the ability to quantify the volume and intensity of training an athlete has performed. In doing so, the practitioner can methodically manipulate training variables and increase or decrease the amount of training stress on a given day to allow for consistent improvement without exposing the athlete to loads that they are not prepared to tolerate. Several methods have been proposed to assist practitioners in understanding the dose-response relationship of training.51-54 In order to provide practitioners with low cost methods, this commentary will focus mainly on the use of Session Rating of Perceived Exertion (sRPE). More objective methods of training monitoring exist (e.g., HR, Global Position System (GPS) tracking, etc.); however these methods can be costly and require specific expertise to handle the data is required.
QUANTIFYING TRAINING SESSIONS
The dose-response relationship describes the interaction between what the athlete did in training and how they responded to it.51 A distinction between external (what the athlete did) and internal (how they responded) training load factors allows for contextualization of the applied training loads.
External training load represents the work performed by the athlete in a given training session.53 It can be quantified in several ways, such as the distance covered, amount of high speed running performed, weight lifted, or total training volume. The rehabilitation specialist or strength coach plans the expected external training load for a given day; as they select the training modality, exercise intensity, volume of work, and the work to rest ratio. Various methods of external load quantification have been explored in the literature.53 The use of integrated microtechnology (GPS, accelerometers, and gyroscopes) has become one of the most popular methods of external load quantification in team sport53,55-57 as these systems allow for the quantification of running, collisions, accelerations, decelerations, and change of direction measures during practice or sports training.56,58,59 Unfortunately, the expense of these systems may make their use impractical for practitioners in private practice or those working with teams or smaller universities with limited budgets. In these cases charting the details of the athletes training session is a simple alternative to track external training load as seen in Figure 2.
Figure 2.
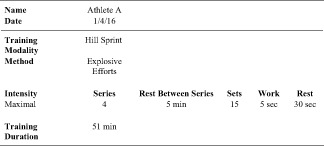
Example Training Document.
The athlete's response to the planned training session is termed internal training load.51,53 A well documented method of internal load quantification is heart rate response.51,53,54,60 The relationship between heart rate response and exercise intensity during a training session has been explored using various training impulse (TRIMP) models, which assign a weighting factor to an arbitrary number of HR zones.51,53,54,60 The HR zones are then summated to create a training load score for a given training session. While this approach is easy to apply the financial burden of purchasing equipment is still present60 and the kinetic response of HR adjustment makes them impractical for interval based training. Thus the use of internal load quantification via the session Rating of Perceived Exertion (sRPE) method is likely the most clinically applicable method available.45,51,53,54,60
Originally developed by Foster and colleagues,45,51 the RPE method allows the quantification of training load without the use of heart rate technology. Foster and colleagues found a consistent relationship between TRIMP scores and the individual's RPE during aerobic exercise45 and others have found similar relationships with RPE and %HRpeak and blood lactate.61 The athlete is asked to rate the intensity of the training session utilizing the descriptors of the CR10 Scale (Table 7).45,62 An arbitrary training load based on session RPE can be calculated by multiplying the corresponding number for the descriptor on the CR10 Scale by the duration of training, in minutes.62,63 These values can be stored in any spreadsheet software file for the individual athlete and changes in training load can be charted over time (Figure 3).
Figure 3.

Change in Training Load Over Time, for hypothetical “Athlete A”. Note: Values are calculated using RPE x Time.
It has been recommended that the athlete be asked to provide their session RPE approximately 20-30min following the training session.63,64 The timing of the response is thought to improve the athlete's ability to reflect on the session as a whole versus their perception of the last activity performed in the training session, which could be skewed by their overall fatigue at that time.45,64 This limitation may present a problem for practitioners, as keeping the athlete in the facility for 20-30min following their training session is often not practical. More recently, the importance of measurement timing has been called into question. Uchida and colleagues65 collected sRPE on boxers at both 10 and 30 min post training following three standardized training sessions (easy, moderate, and hard). They found that RPE had little variation between the 10 and 30min measurements across all three training sessions. Kraft and colleagues66 observed a similar response when quantifying sRPE for resistance training sessions taken at 15 vs. 30min. These findings indicate that practitioners may be able to practically apply the sRPE method in settings where it is not practical to wait 20-30min following training.
Initially developed for aerobic exercise, session RPE has also been found to be valuable for quantifying other training activities. For example, session RPE has been used as a marker for training load during intermittent team sport activities and resistance training, providing practitioners with an affordable and easy to administer method of quantifying the internal training response.60,66-73
Finally, in addition to quantifying the session as a whole, RPE can be used to quantify bouts of work during energy system training.28 If the practitioner lacks a HR monitor, a prescribed RPE could be presented to the athlete for their work intervals. For example, performing high intensity efforts at an RPE of 8-9 for 30 s of work followed by 30 s of recovery at an RPE of 2.
MODELING THE TRAINING PROGRAM
Daily training loads can be evaluated over time to quantify how much training the athlete has performed during their RTP process and to ensure that they have trained enough in order to withstand the loads of practice and competition. As a method of understanding periodization in sport, RPE has often been reported in the literature in absolute terms, reflecting cumulative loads over one to two week blocks of training, or percent changes from one week to the next.67,68,73-75 While this method of reporting provides a useful look at how an athlete's program is progressing it tells little about the cumulative effect that training has had on the body. Utilizing RPE, a recent method proposed by Hulin and colleagues seeks to take into account both acute and chronic load during the training process as a way of quantifying changes in fitness and fatigue.76 This method, termed the acute:chronic ratio, allows practitioners to determine how the athlete is tolerating the training processes over time, while slowly progressing back to pre-injury fitness levels.12
The acute load represents the most recent weekly training load for the athlete while the chronic load is the four-week average of work the athlete has performed.76 The acute load is divided by the chronic load to produce a single number, which describes the athlete's current status.77 A ratio greater than 1 would indicate that the acute load for that week exceeded what the athlete had previously been exposed to.76 Using this method, it was observed that rugby athletes who exceed an acute:chronic workload of 2.11 were at a 3.4 times greater risk of injury.77 The metric is easy to compute and a visualization of the training response during the RTP program can serve as a discussion point amongst medical, rehabilitation, strength and conditioning coaches, and coaches.
Table 8 shows an example of using the acute:chronic training load to plan training. Periods of intense training are helpful in building an athlete's fitness, however, excessive periods of intense loading expose the athlete to increased risk of injury or, for the rehabilitating athlete, re-injury.45,63,78,79 The acute:chronic training load is useful for identifying periods of excessive loading, as can be seen by the conditional formatting in Figure 4. The acute:chronic ratio is flagged “red” any time the acute:chronic training load exceeds 2 and “yellow” any time the acute:chronic load exceeds 1. For example, in the first case there is an acute:chronic load of 2.10. The acute load in that given session was 6856, which is 2.10x greater than the average of the previous four sessions (3269.3). This data can be represented graphically as well. The bottom of Figure 4 shows a chart representing the athlete's acute load (red), chronic load (green), and acute:chronic ratio (grey shading). Additionally, the threshold lines indicating an acute:chronic load of 1 and 2 are also represented. In the example the practitioner noticed the high training loads for three consecutive weeks (weeks 5-7) before planning a few weeks of lower training (weeks 8-10) to allow for recovery and a dissipation of accrued fatigue.
Figure 4.
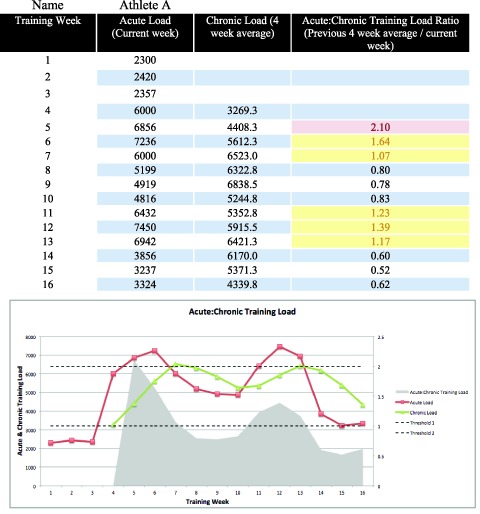
Acute: Chronic Training Load for hypothetical “Athlete A”. Note: Values are calculated using RPE x Minutes
CONCLUSION
RTP from an injury is a challenging process for everyone involved. The numerous factors inherent to decision making within the RTP process have been addressed in the recently updated StARRT framework.4,6 The framework is defined by a comparison of the individuals risk tolerance to the risk involved in their RTP. This clinical commentary has attempted to demonstrate how this can be used when assessing and programming energy system development in the injured athlete. An assessment based on the demands of the sport and the acute:chronic training load can be utilized to monitor the gap between these two domains. The implementation of energy system development principals allows the clinician to address the athlete's readiness and tolerance to the increasing demands they will face. By approaching the return to sport question in this manner the RTP team is able to ensure that relevant risks specific to capacity and workload are discussed and addressed during the rehabilitations and RTP process. This allows the athlete to RTP with a capacity that is able to handle the levels of stress that their spor requires.
REFERENCES
- 1.Conn JM Annest JL Gilchrist J. Sports and recreation related injury episodes in the US population, 1997-99. Inj Prev. 2003;9(2):117–123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ardern CL Glasgow P Schneiders A, et al. 2016 Consensus statement on return to sport from the First World Congress in Sports Physical Therapy, Bern. Br J Sports Med. 2016;50(14):853–864. [DOI] [PubMed] [Google Scholar]
- 3.Ekstrand J Hagglund M Walden M. Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med. 2011;45(7):553–558. [DOI] [PubMed] [Google Scholar]
- 4.Creighton DW Shrier I Shultz R, et al. Return-to-play in sport: A decision-based model. Clin J Sport Med. 2010;20(5):379–385. [DOI] [PubMed] [Google Scholar]
- 5.Kraemer W Denegar C Flanagan S. Recovery from injury in sport: considerations in the transition from medical care to performance care. Sports Health 2009;1(5):392–395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Shrier I. Strategic assessment of risk and risk tolerance (StARRT) framework for return-to-play decision-making. Br J Sports Med. 2015;49(20):1311–1315. [DOI] [PubMed] [Google Scholar]
- 7.Clover J Wall J. Return-to-play criteria Following sports injury. Clin Sports Med. 2010;29(1):169–175. [DOI] [PubMed] [Google Scholar]
- 8.Barber-Westin SD Noyes FR. Factors used to determine return to unrestricted sports activities after anterior cruciate ligament reconstruction. Arthroscopy. 2011;27(12):1697–1705. [DOI] [PubMed] [Google Scholar]
- 9.Herrington L Myer G Horsley I. Task based rehabilitation protocol for elite athletes following Anterior Cruciate ligament reconstruction: a clinical commentary. Phys Ther Sport. 2013;14(4):188–198. [DOI] [PubMed] [Google Scholar]
- 10.Ithurburn MP Paterno MV Ford KR, et al. Young athletes with quadriceps femoris strength asymmetry at return to sport after anterior cruciate ligament reconstruction demonstrate asymmetric single-leg drop-landing mechanics. Am J Sports Med. 2015;43(11):2727–2737. [DOI] [PubMed] [Google Scholar]
- 11.Kyritsis P Bahr R Landreau P Miladi R Witvrouw E. Likelihood of ACL graft rupture: not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. Br J Sports Med. 2016;50(15):946–951. [DOI] [PubMed] [Google Scholar]
- 12.Blanch P Gabbett TJ. Has the athlete trained enough to return to play safelyϿ. The acute:chronic workload ratio permits clinicians to quantify a player's risk of subsequent injury. Br J Sports Med. 2016;50(8):471–475. [DOI] [PubMed] [Google Scholar]
- 13.Matheson GO Shultz R Bido J, et al. Return-to-play decisions: Are they the team physician's responsibility? Clin J Sport Med. 2011;21(1):25–30. [DOI] [PubMed] [Google Scholar]
- 14.Reiman MP Lorenz DS. Integration of strength and conditioning principles into a rehabilitation program. Int J Sports Phys Ther. 2011;6(3):241–253. [PMC free article] [PubMed] [Google Scholar]
- 15.Lorenz D Morrison S. Current concepts in periodization of strength and conditioning for the sports physical therapist. Int J Sports Phys Ther. 2015;10:734–747. [PMC free article] [PubMed] [Google Scholar]
- 16.Baechle TR Earle RW. Essentials of Strength Training and Conditioning. Human Kinetics; 2008. [Google Scholar]
- 17.Bishop D Girard O Mendez-Villanueva A. Repeated-sprint ability - part II: recommendations for training. Sports Med. 2011;41:741–756. [DOI] [PubMed] [Google Scholar]
- 18.Gibala MJ McGee SL. Metabolic adaptations to short-term high-intensity interval training: a little pain for a lot of gain? Exerc Sport Sci Rev. 2008;36(2):58–63. [DOI] [PubMed] [Google Scholar]
- 19.Gastin PB. Energy system interaction and relative contribution during maximal exercise. Sports Med. 2001;31(10):725–741. [DOI] [PubMed] [Google Scholar]
- 20.Girard O Mendez-Villanueva A Bishop D. Repeated-sprint ability - part I: factors contributing to fatigue. Sports Med. 2011;41:673–694. [DOI] [PubMed] [Google Scholar]
- 21.Wadley G Le Rossignol P. The relationship between repeated sprint ability and the aerobic and anaerobic energy systems. J Sci Med Sport. 1998;1(2):100–110. [DOI] [PubMed] [Google Scholar]
- 22.Bishop DJ. Fatigue during intermittent-sprint exercise. Clin Exp Pharmacol Physiol 2012;39:836–841. [DOI] [PubMed] [Google Scholar]
- 23.Buchheit M Laursen PB. High-intensity interval training, Solutions to the programming puzzle. Sports Med. 2013;43(10):927–954. [DOI] [PubMed] [Google Scholar]
- 24.Little T Williams AG. Effects of sprint duration and exercise: rest ratio on repeated sprint performance and physiological responses in professional soccer players. J Strength Cond Res. 2007;21:646–648. [DOI] [PubMed] [Google Scholar]
- 25.Spencer M Bishop D Dawson B, et al. Metabolism and performance in repeated cycle sprints: active versus passive recovery. Med Sci Sports Exerc. 2006;38:1492–1499. [DOI] [PubMed] [Google Scholar]
- 26.Dupont G Millet GP Guinhouya C, et al. Relationship between oxygen uptake kinetics and performance in repeated running sprints. Eur J Appl Physiol. 2005;95(1):27–34. [DOI] [PubMed] [Google Scholar]
- 27.Bishop D Lawrence S Spencer M. Predictors of repeated-sprint ability in elite female hockey players. J Sci Med Sport. 2003;6(2):199–209. [DOI] [PubMed] [Google Scholar]
- 28.Buchheit M Laursen PB. High-intensity interval training, Solutions to the programming puzzle. Sports Med. 2013;43(5):313–338. [DOI] [PubMed] [Google Scholar]
- 29.Helgerud J Høydal K Wang E, et al. Aerobic high-intensity intervals improve VO2max more than moderate training. Med Sci Sports Exerc. 2007;39:665–671. [DOI] [PubMed] [Google Scholar]
- 30.McKay BR Patterson DH Kowalchuk JM. Effect of short-term high-intensity interval training vs. continuous training on O2 uptake kinetics, muscle deoxygenation, and exercise performance. J Appl Physiol . 2009;107(1):128–138. [DOI] [PubMed] [Google Scholar]
- 31.Laursen PB. Training for intense exercise performance: high-intensity or high-volume training? Scand J Med Sci Sports. 2010;20:1–10. [DOI] [PubMed] [Google Scholar]
- 32.Little JP Safdar A Bishop D, et al. An acute bout of high-intensity interval training increases the nuclear abundance of PGC-1α and activates mitochondrial biogenesis in human skeletal muscle. Am J Physiol. 2011;300(6):R1303–R1310. [DOI] [PubMed] [Google Scholar]
- 33.Helgerud J Engen LC Wisløff U, et al. Aerobic endurance training improves soccer performance. Med Sci Sports Exerc. 2001;33: 1925–1931. [DOI] [PubMed] [Google Scholar]
- 34.Dupont G Akakpo K Berthoin S. The effect of in-season high-intensity interval training in soccer players. J Strength Cond Res. 2004;18(3):584. [DOI] [PubMed] [Google Scholar]
- 35.Chamari K Padulo J. ‘Aerobic’ and “Anaerobic” terms used in exercise physiology: a critical terminology reflection. Sports Med - Open 2015;1:9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Elliott MC Wagner PP Chiu L. Power athletes and distance training. Sports Med. 2007;37(1):47–57. [DOI] [PubMed] [Google Scholar]
- 37.Stone NM Kilding DAE. Aerobic conditioning for team sport athletes. Sports Med. 2009;39(8):615–642. [DOI] [PubMed] [Google Scholar]
- 38.Bogdanis GC Nevill ME Boobis LH, et al. Contribution of phosphocreatine and aerobic metabolism to energy supply during repeated sprint exercise. J Appl Physiol . 1996;80(3):876–884. [DOI] [PubMed] [Google Scholar]
- 39.Gaitanos GC Williams C Boobis LH, et al. Human muscle metabolism during intermittent maximal exercise. J Appl Physiol. 1993;75(2):712–719. [DOI] [PubMed] [Google Scholar]
- 40.Haseler LJ Hogan MC Richardson RS. Skeletal muscle phosphocreatine recovery in exercise-trained humans is dependent on O2availability. J Appl Physiol. 1999;86(6):2013–2018. [DOI] [PubMed] [Google Scholar]
- 41.Bangsbo PJ Iaia FM Krustrup P. The Yo-Yo intermittent recovery test. Sports Med. 2008;38(1):37–51. [DOI] [PubMed] [Google Scholar]
- 42.Dawson B. Repeated-sprint ability: where are we? Int J Sports Physiol Perform. 2012;7: 285–289. [DOI] [PubMed] [Google Scholar]
- 43.Mann T Lamberts RP Lambert MI. Methods of prescribing relative exercise intensity: Physiological and practical considerations. Sports Med. 2013;43(7):613–625. [DOI] [PubMed] [Google Scholar]
- 44.Eston R. Use of ratings of perceived exertion in sports. Int J Sports Physiol Perform 2012;7:175–182. [DOI] [PubMed] [Google Scholar]
- 45.Foster C Florhaug JA Franklin J, et al. A New approach to monitoring exercise training. J Strength Cond Res. 2001;15(1):109. [PubMed] [Google Scholar]
- 46.Seiler KS Kjerland GO. Quantifying training intensity distribution in elite endurance athletes: is there evidence for an “optimal” distribution? Scand J Med Sci Sports. 2006;16(1):49–56. [DOI] [PubMed] [Google Scholar]
- 47.Sylta Ø Tønnessen E Seiler S. From heart-rate data to training quantification: A comparison of 3 methods of training-intensity analysis. Int J Sports Physiol Perform. 2014;9(1):100–107. [DOI] [PubMed] [Google Scholar]
- 48.Hoffman JR. The applied physiology of American football. Int J Sports Physiol Perform. 2008;3(3):387–392. [DOI] [PubMed] [Google Scholar]
- 49.Iosia MF Bishop PA. Analysis of exercise-to-rest ratios during division IA televised football competition. J Strength Cond Res. 2008;22(2):332–340. [DOI] [PubMed] [Google Scholar]
- 50.Rhea MR Hunter RL Hunter TJ. Competition modeling of American football: observational data and implications for high school, collegiate, and professional player conditioning. J Strength Cond Res. 2006;20(1):58–61. [DOI] [PubMed] [Google Scholar]
- 51.Borresen J Lambert MI. The quantification of training load, the training response and the effect on performance. Sports Med. 2009;39(9):779–795. [DOI] [PubMed] [Google Scholar]
- 52.Buchheit M Racinais S Bilsborough JC, et al. Monitoring fitness, fatigue and running performance during a pre-season training camp in elite football players. J Sci Med Sport. 2013;16(6):550–555. [DOI] [PubMed] [Google Scholar]
- 53.Halson SL. Monitoring training load to understand fatigue in athletes. Sports Med. 2014;44(2):139–147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Lambert MI Borresen J. Measuring training load in sports. Int J Sports Physiol Perform. 2010;5(3):406–411. [DOI] [PubMed] [Google Scholar]
- 55.Aughey RJ. Applications of GPS technologies to field sports. Int J Sports Physiol Perform. 2011:6: 295–310. [DOI] [PubMed] [Google Scholar]
- 56.Boyd LJ Ball K Aughey RJ. Quantifying external load in Australian football matches and training using accelerometers. Int J Sports Physiol Perform 2013;8: 44–51. [DOI] [PubMed] [Google Scholar]
- 57.Dellaserra CL Gao Y Ransdell L. Use of integrated technology in team sports: A review of opportunities, challenges, and future directions for athletes. J Strength Cond Res. 2014;28(2):556–573. [DOI] [PubMed] [Google Scholar]
- 58.Gabbett TJ. Relationship between accelerometer load, collisions, and repeated high-intensity effort activity in rugby league players. J Strength Cond Res. 2015;29(12):3424–3431. [DOI] [PubMed] [Google Scholar]
- 59.Wundersitz DW Gastin PB Robertson SJ, et al. Validity of a trunk-mounted accelerometer to measure physical collisions in contact sports. Int J Sports Physiol Perform. 2015;10: 681–686. [DOI] [PubMed] [Google Scholar]
- 60.Impellizzeri FM Rampinini E Coutts AJ, et al. Use of RPE-based training load in soccer. Med Sci Sports Exerc. 2004;36: 1042–1047. [DOI] [PubMed] [Google Scholar]
- 61.Coutts AJ Rampinini E Marcora SM, et al. Heart rate and blood lactate correlates of perceived exertion during small-sided soccer games. J Sci Med Sport. 2009;12(1):79–84. [DOI] [PubMed] [Google Scholar]
- 62.Borg G Hassmén P Lagerström M. Perceived exertion related to heart rate and blood lactate during arm and leg exercise. Eur J Appl Physiol Occup Physiol. 1987;56(6):679–685. [DOI] [PubMed] [Google Scholar]
- 63.Foster C. Monitoring training in athletes with reference to overtraining syndrome. Med Sci Sports Exerc. 1998;30(7):1164–1168. [DOI] [PubMed] [Google Scholar]
- 64.Hornsby JH Green JM O’Neal EK, et al. Influence of terminal RPE on session RPE. J Strength Cond Res. 2013;27(10):2800–2805. [DOI] [PubMed] [Google Scholar]
- 65.Uchida MC Teixeira LFM Godoi VJ, et al. Does the timing of measurement alter session-RPE in boxers? J Sports Sci Med. 2014;13(1):59–65. [PMC free article] [PubMed] [Google Scholar]
- 66.Kraft JA Green JM Thompson KR. Session ratings of perceived exertion responses during resistance training bouts equated for total work but differing in work rate. J Strength Cond Res. 2014;28(2):540–545. [DOI] [PubMed] [Google Scholar]
- 67.Cross MJ Williams S Trewartha G, et al. The influence of in-season training loads on injury risk in professional rugby union. Int J Sports Physiol Perform. 2016;11(3):350-355. [DOI] [PubMed] [Google Scholar]
- 68.Genner KM Weston M. A comparison of workload quantification methods in relation to physiological responses to resistance exercise. J Strength Cond Res. 2014;28(9):2621–2627. [DOI] [PubMed] [Google Scholar]
- 69.Jeong T-S Reilly T Morton J, et al. Quantification of the physiological loading of one week of “pre-season” and one week of ‘in-season’ training in professional soccer players. J Sports Sci . 2011;29(11):1161–1166. [DOI] [PubMed] [Google Scholar]
- 70.Kraft JA Green JM Gast TM. Work distribution influences session ratings of perceived exertion response during resistance exercise matched for total volume. J Strength Cond Res. 2014;28(7):2042–2046. [DOI] [PubMed] [Google Scholar]
- 71.Lovell TWJ Sirotic AC Impellizzeri FM, et al. Factors affecting perception of effort (session rating of perceived exertion) during rugby league training. Int J Sports Physiol Perform. 2013;8(1):62–69. [DOI] [PubMed] [Google Scholar]
- 72.Moreira A Bilsborough JC Sullivan CJ, et al. Training periodization of professional Australian football players during an entire Australian Football League season. Int J Sports Physiol Perform. 2015;10(5):566–571. [DOI] [PubMed] [Google Scholar]
- 73.Ritchie D Hopkins WG Buchheit M, et al. Quantification of training and competition load across a season in an elite australian football club. Int J Sports Physiol Perform. 2015;11(4):474–479. [DOI] [PubMed] [Google Scholar]
- 74.Rogalski B Dawson B Heasman J, et al. Training and game loads and injury risk in elite Australian footballers. J Sci Med Sport. 2013;16(6):499–503. [DOI] [PubMed] [Google Scholar]
- 75.Veugelers KR Young WB Fahrner B, et al. Different methods of training load quantification and their relationship to injury and illness in elite Australian football. J Sci Med Sport. 2016;19(1):24–28. [DOI] [PubMed] [Google Scholar]
- 76.Hulin BT Gabbett TJ Blanch P, et al. Spikes in acute workload are associated with increased injury risk in elite cricket fast bowlers. Br J Sports Med. 2013;48(8):bjsports–2013–092524–712. [DOI] [PubMed] [Google Scholar]
- 77.Hulin BT Gabbett TJ Lawson DW, et al. The acute:chronic workload ratio predicts injury: high chronic workload may decrease injury risk in elite rugby league players. Br J Sports Med. 2016;50(4):231–236. [DOI] [PubMed] [Google Scholar]
- 78.Kiely J. New horizons for the methodology and physiology of training periodization. Sports Med. 2010;40(9):803–805. [DOI] [PubMed] [Google Scholar]
- 79.Issurin VB. New horizons for the methodology and physiology of training periodization. Sports Med. 2010;40(3):189–206. [DOI] [PubMed] [Google Scholar]