

Abstract
Background
This is the first study of a Taiwanese population reporting transcatheter aortic valve implantation (TAVI) outcomes of the first 100 cases from a single center offering two different transcatheter heart valve technologies via six types of approaches. We herein report the 30-day and one-year outcomes in our first 100 TAVI patients at Taipei Veterans General Hospital.
Methods
From May 2010 to April 2016, 100 consecutive patients with severe aortic stenosis (AS) who were considered unsuitable or at high risk for surgical aortic valve replacement underwent TAVI. Patient outcomes were classified according to the Valve Academic Research Consortium-2 (VARC-2) definitions. The device performance was assessed using transthoracic echocardiography by independent investigators.
Results
The mean patient age was 81.1 years, where 54% were female, and the mean Logistic EuroSCORE was 21.5%. The Medtronic CoreValve was used in 84 patients and the Edwards Sapien or Sapien XT valve (ESV) in 16. The transfemoral approach was the most frequently used route (83%), followed by transapical (9%) access. Overall, there was no procedural death. The VARC-2 outcomes were as follows: device success, 95%; stroke, 1%; major vascular complication, 3%; a need for pacemaker implantation, 5.1%. At discharge, the incidence of postoperative mild, moderate or severe paravalvular leak was 30%, 3% and 0%, respectively. At one year, the all-cause mortality rate was 14.0%, and no valve-related dysfunction was observed. Through multivariable analysis, non-transfemoral access [hazard ratios (HR) 4.81; 95% confidence interval (CI) 1.66-14.09; p = 0.004] and advanced chronic kidney disease (stages 4-5), (HR 3.13; 95% CI 1.07-9.09; p = 0.036) were independently associated with an increased risk of one-year mortality.
Conclusions
We demonstrated that TAVI shows good early and mid-term outcomes in terms of survival, technical success, valve-related adverse events and haemodynamic performance in high-risk patients with severe AS.
Keywords: Aortic stenosis, Edwards Sapien XT, Medtronic CoreValve, TAVI
INTRODUCTION
Degenerative aortic stenosis (AS) is the most common valvular heart disease in adults, with a prevalence of approximately 4% in patients over 80 years of age. After the onset of symptoms (angina, syncope, or heart failure), the average survival time is 2 to 3 years, with a high risk of sudden death.1 Surgical replacement of the aortic valve (SAVR), which has been the only effective treatment in adults with severe symptomatic AS, provides symptomatic relief and long-term survival. However, in clinical practice, more than 30% of patients with severe symptomatic AS do not undergo SAVR due to advanced age, left ventricular dysfunction, or the presence of multiple coexisting conditions.2,3 Current evidence points to the clinical superiority of transcatheter aortic valve implantation (TAVI) vs. medical therapy in patients with critical AS deemed inoperable,4 and TAVI is now deemed equivalent to SAVR in severe AS patients at high surgical risk.5-7 To date, over 100,000 TAVI procedures have been performed worldwide, and over 600 of these procedures took place in Taiwan. A large meta-analysis of 8874 patients undergoing TAVI showed 7.5% of patients died within 30 days, and the cumulative mortality rate was 21.6% at the one-year interval.8 More than 100 patients have undergone TAVI procedure using self-expanding Medtronic CoreValve (MCV) (Medtronic, Minneapolis, MN) or balloon-expandable Edwards Sapien or Sapien XT devices (ESV) (Edwards Lifesciences, Irvine, CA) at Taipei Veterans General Hospital. We report the 30-day and one-year Valve Academic Research Consortium-2 (VARC-2)9 outcomes in our first 100 TAVI patients.
METHODS
Patients
From May 2010 to April 2016, 100 consecutive patients with severe AS (valve area ≤ 1.0 cm2 and mean aortic-valve gradient ≥ 40 mm Hg) underwent TAVI by one team at our institution. All patients had New York Heart Association (NYHA) symptoms exceeding class II. Patients were selected for TAVI when considered unsuitable or at high risk for surgical aortic valve replacement by heart team discussion. Operative risk was calculated using the logistic European System for Cardiac Operative Risk Evaluation (EuroSCORE) score. Patient selection for TAVI was based on the approved indication for TAVI in Taiwan using either of the following criteria: 1) patients considered to beat high surgical risk with logistic EuroSCORE ≥ 20%, 2) the age of the patients was above 80 year-old, 3) patients have any one of the following condition including previous cardiac surgery, porcelain aorta, thoracic burning sequelae contrain dicating open heart surgery, history of mediastinum radiotherapy, severe connective tissue disease resulting in a contrain dication to surgery, cirrhosis of the liver (child class A or B), or severe pulmonary insufficiency with forced expiratory volume in one second (FEV1) < 1 liter. Patients for whom TAVI was deemed to be the best treatment option were selected based on the clinical consensus of a multidisciplinary team consisting of cardiac surgeons, interventional cardiologists, anesthetists, and imaging specialists.
The main exclusion criteria were a native aortic valve annulus of less than 18 mm or more than 29 mm, acute myocardial infarction < 14 days, a left ventricular ejection fraction of < 20%, active infection, hemodynamic instability, or life expectancy < 12 months.
Devices
In Taiwan, our multidisciplinary team was the first to apply to the Department of Health, R.O.C. for approval of the TAVI program using the balloon-expandable Edwards Sapien valve (Edwards Lifesciences, Irvine, CA, USA). We started TAVI with the Edwards Sapien valve in 10 patients in 2010.10,11 From October 2010 to December 2012, no TAVI devices was available in Taiwan until self-expandable MCV (Medtronic, Minneapolis, MN, USA) was approved in December 2012. The bioprosthesis was then added to our practice and has been predominantly used at our institution since then. The Edwards Sapien XT device was also accessible after it was approved in December 2015.
Procedures
All TAVI procedures were performed in a specially equipped hybrid operating suite. At the beginning of our experience, TAVI procedures were performed under general anesthesia. In December 2013, local anesthesia with conscious sedation had been exclusively used for transfemoral TAVI at our institution. The standard approach for both valves was through the transfemoral route, if feasible. In patients who did not have adequate anatomy to allow safe transfemoral access, alternative access routes such as trans-subclavian,12 direct aortic13 trans-abdominal aortic,14 or transcarotid15 access for the MCV and transapical16 access for the ESV (Edwards Sapien or Sapien XT) were used. Adjunct pharmacologic therapy included heparin during the procedure and aspirin (100 mg/day) indefinitely and clopidogrel (75 mg/day) for 3-6 months following the procedure.
Transfemoral (TF) approach
TF procedures were performed by surgical cutdown of femoral arteries or double-ProGlide (Abbott Vascular) preclose technique.17 After retrograde pre-dilation of the native valve, the valve was crossed and implanted as previously described.18
Trans-subclavian approach
This procedure required surgical isolation of the left axillary artery. Once the artery was isolated, a purse string suture was placed to allow subsequent closure at the end of the procedure. The artery was punctured at the distal end of the purse string, and a 6-F sheath was placed into the artery. The standard 0.035-inch guidewire was then exchanged for a pre-shaped 0.035-inch Amplatz Super Stiff guidewire, and an 18-F sheath was positioned in the axillary artery. The valve was crossed with the same procedure as previously described for the TF approach.18 Then, the axillary access site was surgically repaired.12
Direct aortic approach
The procedure was performed through a 5-cm incision in the right second intercostal space. The right anterior mini-thoracotomy was made such that the medial angle of incision was positioned just before the projection of the right internal mammary artery 1.5-2 cm laterally to the sternal edge. A basal ascending aorta aortography, using a graduated pigtail, was performed to measure the distance between the aortic annulus and the selected entry site in the ascending aorta. To safely perform the MCV implantation, more than 6 cm was needed. At the entry site, two aortic purse-string sutures for direct aortic access were placed in a standard fashion as previously reported.13
Transcarotid approach
Under general anesthesia, the proximal common right carotid artery of the patient was exposed through a small incision 2-cm above the right clavicle. An 8-Fr sheath was initially inserted in the artery using a percutaneous technique. Progression of wires and sheaths was followed with caution under fluoroscopy. Thereafter, an 18-Fr sheath was placed down to the upper part of the ascending aorta for introduction of the delivery catheter. To reduce cerebral hypoperfusion, another 8-Fr sheath (5 cm in length) was inserted into the right carotid artery in the opposite direction from the 18-Fr sheath. The two sheaths were connected by a catheter extension tube (2 cm in inner diameter and 20 cm in length), shunting blood through the upper part of the ascending aorta to the distal common right carotid artery. Cerebral oximetry with near infrared spectrometer was continually monitored to assess cerebral perfusion throughout the procedure.
Trans-abdominal aortic approach
Laparotomy was performed through a midline incision, and the omentum and bowels were protected and packed away from the surgical field. The distal abdominal aorta was gently palpated to identify an area free of calcifications. The aorta was punctured with a standard needle, and a soft J-tip 0.035 wire was advanced through a 6-Fr sheath. A pigtail catheter was placed over the wire into the ascending aorta, and then the soft wire was exchanged for a super stiff Amplatzwire. After dilatation with 12- and 18-Fr dilators over the stiff wire, the 18-Fr sheath was inserted through the abdominal aorta into the descending aorta.14
Transapical approach
For the transapical procedure, a left anterolateral mini-thoracotomy and pericardiotomy were performed, and a double pledgeted purse-string suture or U stitches were placed at the left ventricular apex. After puncture of the apex, antegrade crossing, and pre-dilatation, the ESV was deployed underrapid ventricular pacing as previously reported.16
Study endpoints
All clinical endpoints of this study were defined according to the VARC-2 criteria.9 "Device success" was defined as the absence of procedural mortality and correct positioning of a single prosthetic heart valve into the proper anatomical location and intended performance of the prosthetic heart valve [no prosthesis-patient mismatch and mean aortic valve gradient < 20 mmHg or peak velocity < 3 m/s, and no moderate or severe prosthetic valve regurgitation (PVL)]. Following valve deployment, assessment of valve function was performed using transthoracic echocardiography by independent investigators before discharge, at the 3-month follow-up, and at the 6-month follow-up. The 30-day-combined safety endpoint is a combined endpoint defined by VARC-2 as a composite of all-cause mortality, major stroke, life-threatening or disabling bleeding, acute stage 2 or 3 kidney injury including renal replacement therapy, major vascular complications, and repeat procedure for valve-related dysfunction. VARC-2 proposed using the AKIN system for the reporting of acute kidney injury (AKI). AKI was defined as an absolute (< 48 hours) reduction in kidney function and defined as: stage 1 – increase in serum creatinine to 150-199% (1.5-1.99 x increase compared with baseline) or increase of > 0.3 mg/dL or urine output < 0.5 ml/kg/h for > 6 but < 12 h; stage 2 – increase in serum creatinine to 200--299% (2.0-2.9 x increase compared with baseline) or urine output < 0.5 ml/kg/h for > 12 but < 24 h; stage 3 – increase in serum creatinine to > 300% (> 3 x increase compared with baseline) or serum creatinine of > 4.0 mg/dL with an acute increase of at least 0.5 mg/dL or the new need for renal replacement therapy post TAVI.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD), and analyzed with the Student’s t test or the Wilcoxon rank sum test, depending on the variable distribution. Categorical variables were compared using the chi-square test with Yates’ correction for continuity or the Fisher’s exact test. For all comparisons, a p value of < 0.05 was considered statistically significant. Cumulative survival curves for all-cause mortality were generated using the Kaplan-Meier method. Cox regression was used to evaluate predictors of one-year all-cause mortality. The following variables were selected on the basis of clinical relevance and were included in the Cox model: sex; age ≥ 85 years; logistic EuroSCORE ≥ 20%; estimated glomerular filtration rate (eGFR) using the Modification of Diet in Renal Disease equation ≤ 30 mL/min; left ventricular ejection fraction ≤ 35%; presence of severe pulmonary hypertension (≥ 60 mmHg); type of device; access (TF vs. non-TF); major vascular complications; and moderate, or severe PVL after procedure. Univariable predictors with a p < 0.05 were included in a multivariable model. Stepwise multivariable analyses were performed. The significance level thresholds for entry and exit of independent variables were set at 0.10. Hazard ratios (HR), 95% confidence intervals (CI), and p values from the final multivariable Cox proportional hazards models are presented. All analyses were performed using SAS software (version 9.3, SAS Institute Inc., Cary, North Carolina, USA).
RESULTS
Baseline characteristics
From May 2010 to April 2016, one hundred consecutive patients undergoing TAVI at our institution were included in this analysis. All patients had severe symptomatic AS (mean aortic valve area 0.67 ± 0.22 cm2 and mean trans-aortic gradient 48.1 ± 18.9 mmHg). Among these patients, eight (8%) had a bicuspid aortic valve, three (3%) had previously undergone mitralvalve replacement with a mechanical prosthesis, and one (1%) underwent valve-in-valve implantation for failed St. Jude EPIC porcine valve. Baseline clinical and echocardiographic characteristics of the study population are shown in Table 1. Forty-six percent of the population were male, and the mean age was 81.1 years. The mean logistic EuroSCORE was 21.5%.
Table 1. Baseline characteristics of the study population (n = 100).
| Age (yrs) | 81.1 ± 7.9 |
| Men | 46 (46%) |
| Body mass index (kg/m2) | 24.2 ± 3.7 |
| Body surface area (m2) | 1.61 ± 0.20 |
| Hypertension | 73 (73%) |
| Diabetes mellitus | 41 (41%) |
| Hyperlipidemia | 38 (38%) |
| NYHA class III or IV | 81 (81%) |
| CAD | 37 (37%) |
| Previous MI | 4 (4 %) |
| Previous PCI | 27 (27%) |
| Previous CABG | 6 (6%) |
| Peripheral artery disease | 18 (18%) |
| Cerebrovascular disease | 19 (19%) |
| Pulmonary disease | 32 (32%) |
| Previous BAV | 9 (9%) |
| Previous pacemaker | 2 (2%) |
| Atrial fibrillation | 22 (22%) |
| Logistic EuroSCORE (%) | 21.5 ± 16.3 |
| Serum creatinine (mg/dL) | 1.6 ± 2.0 |
| Estimated GFR (ml/min) | 43.3 ± 19.9 |
| Estimated GFR < 60 ml/min | 81 (81%) |
| Bicuspid valve | 9 (9%) |
| Previous mitral prosthesis | 3 (3%) |
| Pre-existing pacemaker | 2 (2%) |
| Dialysis | 6 (6%) |
| Echocardiographic findings | |
| Aortic valve area (cm2) | 0.67 ± 0.22 |
| Mean PG (mmHg) | 48.1 ± 18.5 |
| LVEF (%) | 54.5 ± 10.9 |
| LVEF < 35% | 10 (10%) |
| sPAP > 60 mmHg | 14 (14%) |
Data are expressed as mean ± SD or number (percentage).
BAV, balloon aortic valvuloplasty; CABG, coronary artery bypass grafting; CAD, coronary artery disease; GFR, glomerular filtration rate; Logistic EuroSCORE, Logistic European System for Cardiac Operative Risk Evaluation; LVEF, left ventricular ejection fraction; MI, myocardial infarction; NYHA, New York Heart Association; PCI, percutaneous coronary intervention; PG, pressure gradient; sPAP, systolic pulmonary arterial pressure.
Procedural outcomes
The main procedural variables are presented in Table 2. Of the 100 consecutive TAVI procedures performed, the transfemoral approach was the most frequently used route (83%), followed by the transapical approach (9%). The MCV device was implanted in a total of 84 patients. Of that number, 76 patients (90.5%) were treated via the transfemoral approach, 3 (3.6%) via the tran-subclavian approach, 2 (2.4%) via the direct aortic, 2 (2.4%) via the transcaortid, and 1 (1.2%) via the trans-abdominal aortic approach. The ESV device was implanted in 16 patients, 7 (43.8%) via the transfemoral approach and 9 (56.2%) via the transapical approach. The most commonly used implant was the 29-mm valve (48.8%) in the MCV recipients, and the 26-mm valve (50%) in the ESV group. TAVI was performed using local anesthesia with conscious sedation in 57 (57%) patients. The amount of contrast medium administered was 143 ± 69 ml.
Table 2. Procedural characteristics (n = 100).
| Variable | Overall (n = 100) | MCV (n = 84) | ESV (n = 16) | p |
| Bioprosthesis size | ||||
| MCV 26 mm | 35 (41.7%) | |||
| MCV 29 mm | 41 (48.8%) | |||
| MCV 31 mm | 8 (9.5%) | |||
| ESV 23 mm | 7 (43.8%) | |||
| ESV 26 mm | 8 (50%) | |||
| ESV 29 mm | 1 (6.2%) | |||
| Access | ||||
| Transfemoral | 83 (83%) | 76 (90.5%) | 7 (43.8%) | < 0.001 |
| Transapical | 9 (9%) | 9 (56.2%) | ||
| Trans-subclavian | 3 (3%) | 3 (3.6%) | ||
| Direct aortic | 2 (2%) | 2 (2.4%) | ||
| Transcarotid | 2 (2%) | 2 (2.4%) | ||
| Trans-abdominal aortic | 1 (1%) | 1 (1.2%) | ||
| Local anesthesia | 57 (57%) | 56 (66.7%) | 1 (6.3%) | < 0.001 |
Data are expressed as mean ± SD or number (percentage). ESV, Edwards; MCV, Medtronic CoreValve.
Procedural outcomes within the first 72 hours after TAVI are summarized in Table 3. No procedural death occurred. Proper device positioning was achieved in 98 patients, and two of the MCV recipients needed a second valve for the treatment of a low position of the first implanted valve. Three patients (2 among the MCV recipients and 1 in the ESV group) had post-procedural moderate paravalvular regurgitation assessed by echocardiography. Thus, "device success" (defined as absence of procedural mortality, correct positioning of one prosthetic heart valve into the proper anatomical location, and intended performance of the heart valve without moderate or severe regurgitation) was achieved in 95 patients.
Table 3. Postprocedural outcomes (< 72 h after the index procedure) of the study population (n = 100).
| Outcome | No. (%) of events |
| Device successa | 95 (95%) |
| Myocardial infarction | 3 (3%) |
| Coronary obstruction | 2 (2%) |
| Stroke or TIA | 1 (1%) |
| Acute kidney injure, stage 2 or 3 | 3 (3.2%) |
| Major vascular complications | 3 (3%) |
| Cardiac tamponade | 4 (4%) |
| Annulus rupture | 0 |
| Valve malpositioning | 2 (2%) |
| Need for a second valve | 2 (2%) |
| Posptocedural AR, moderate to severe | 3 (3%) |
Data are expressed as mean ± SD or number (percentage).
AR, aortic regurgitation; TIA, transient ischemic attack.
a Defined as absence of procedural mortality, correct positioning of a single prosthetic heart valve into the proper anatomical location, and intended performance of the heart valve without moderate or severe regurgitation.
Three patients had a periprocedural myocardial infarction (MI), and coronary obstruction occurred in two of the MCV recipients. One patient with low-lying ostia of the left coronary artery (8.0 mm) was pre-emptively protected by a guidewire and a balloon through a guide catheter engaged in the left coronary artery. She became hypotensive after MCV deployment, and coronary angiography showed occlusion of the mid segment of left anterior descending artery (LAD), suggestive of embolization of aortic material. Following implantation of one drug-eluting stent in the LAD, the patient’s blood pressure became stable. The other patient with bicuspid aortic valve experienced unexplained hypotension hours after MCV implantation. Transthoracic echocardiography revealed right ventricular dysfunction, suggestive of right coronary artery (RCA) ischemia, which was confirmed by angiography that revealed no flow in the RCA secondary to ostial occlusion by the bicuspid leaflet. We attempted to recanalise the RCA but failed despite use of multiple wires. The patient required temporary hemodynamic support with extracorporeal membrane oxygenation for refractory cardiogenic shock, after which right-ventricular function recovered within a short period of time.
One patient with an MCV suffered from a stroke due to hypovolemic shock caused by left ventricle perforation (defined as major vascular complication by VARC-2) by the Amplatz Super stiff. Excluding six patients on regular hemodialysis, stage 2 or 3 AKI requiring temporary dialysis occurred in three patients (3.2%). Four patients (3 in the MCV recipients and 1 in the ESV group) had cardiac tamponade (categorized as life-threatening bleeding according to VARC-2 definition). One patient developed cardiac tamponade immediately after deployment of an Edwards Sapien valve, and prompt pericardiocentesis successfully stabilized the patient. This may have resulted from an aortic tear caused by asymmetrical distribution of aortic annulus calcification.19 Three MCV recipients had left ventricle perforation (defined as major vascular complication by VARC-2) caused by the Amplatz Super stiff wire, requiring surgical repair.
VARC-2 outcome at 30 days and one year
Thirty-day and one-year outcomes are summarized in Table 4. At the 30-day follow-up, all-cause mortality was 4%: of these patients, three died of sepsis (2 patients suffering from pneumonia and one with liver abscess) and one patient on hemodialysis died suddenly of unknown cause on day 27 after discharge. Stage 2 or 3 AKI developed in three patients after 72 hours, and the cumulative incidence of stage 2 or 3 AKI at 30-day was 6.4%. Excluding two patients with pre-existing pacemakers, the overall incidence of new pacemaker implantation was 5.1% and was comparable between patients treated with MCV or ESV (4.9% in the MCV group vs. 6.3% in the ESV group, p = 0.409). There was no valve-related dysfunction requiring repeat procedure within 30 days.
Table 4. VARC-2 outcomes at 30-day and one-year follow-up.
| Outcome | No. (%) of events |
| 30 dayscumulative clinical outcomes | |
| All-cause mortality | 4 (4%) |
| Cardiac mortality | 1 (1%) |
| All stroke | 1 (1%) |
| Life-threatening bleeding | 4 (4%) |
| Acute kidney injury, stage 2 or 3 | 6 (6.4%) |
| Coronary artery obstruction | 2 (2%) |
| Major vascular complication | 3 (3%) |
| New pacemaker implantation | 5 (5.1%) |
| Valve-related dysfunction requiring repeat procedure (BAV, TAVI, or SAVR) | 0 |
| One-year cumulative clinical outcomes | |
| All-cause mortality | 14 (14%) |
| Cardiac mortality | 1 (1%) |
| All stroke | 3 (3%) |
| Requiring hospitalizations for worsening heart failure | 3 (3%) |
| NYHA class III or IV | 3 (3%) |
| Valve-related dysfunctiona | 0 |
Data are expressed as number (percentage).
BAV, balloon aortic valvuloplasty; SAVR, surgical aortic valve replacement; TAVI, transcatheter aortic valve implantation; VARC, Valve Academic Research Consortium.
a Refers to mean aortic valve gradient > 20 mmHg, the effective orifice area (EOA) < 0.9-1.1 cm2, and/or the Doppler velocity index (DVI) < 0.35 m/s, and/or moderate or severe prosthetic valve regurgitation.
Ten more patients died between 30-days and one-year post-procedure, resulting in a one-year cumulative all-cause mortality rate of 14.0%, and none was cardiac-related. The 100 patients who underwent the procedure were followed up for a mean duration of 748 days. The shortest follow-up time was 6 days, and the longest one was 2455 days. Figure 1 shows the Kaplan-Meier curve of all-cause mortality. Two additional instances of disabling stroke occurred between the 30-day and 1-year mark, resulting in a total stroke rate of 3% at one year. Three patients needed re-hospitalization for heart failure. One additional patient required implantation of a new permanent pacemaker between 30 days and 1 year for an overall one-year rate of 6.1%. No valve-related dysfunction was observed within one year, which includes the presence of moderate or severe prosthesis regurgitation, valve thrombosis, or prosthetic valve endocarditis.
Figure 1.
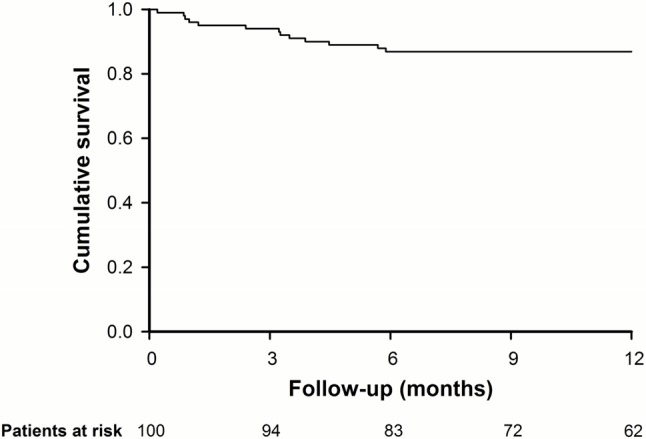
Kaplan-Meier survival curve for all-cause mortality to one year.
Valve performance at one year
At baseline, the mean aortic valve orifice area was 0.67 ± 0.22 cm2, and the mean aortic trans-valvular gradient was 48.1 ± 18.9 mmHg (Table 5). At the time of discharge, the mean effective orifice area had improved to 1.55 ± 0.36 cm2 (p < 0.001 vs. baseline), and the mean aortic transvalvular gradient decreased to 10.2 ± 4.0 mmHg (p < 0.001 vs. baseline). These results were sustained at one year, with a mean orifice area of 1.66 ± 0.49 cm2 and a mean aortic gradient of 10.1 ± 4.7 mmHg. Additional valve performance data by independent investigators are shown in Table 5. Moderate and severe aortic regurgitation (AR) was present before the procedure in 17% and 2% of the patients, respectively. At 30 days after TAVI, paravalvular AR was trivial or mild in 97% of echocardiograms; three patients (3%) had moderate regurgitation, and no patient had severe regurgitation. These results were maintained at the one-year echocardiographic follow-up (Figure 2).
Table 5. Transthoracic echocardiography data.
| Variable | Baseline | Discharge | 30 days | One year |
| Peak aortic gradient, mmHg* | 78.8 ± 29.2 | 18.9 ± 7.8 | 16.9 ± 8.4 | 18.2 ± 8.7 |
| Mean aortic gradient, mmHg* | 48.1 ± 18.9 | 10.2 ± 4.0 | 9.3 ± 4.6 | 10.1 ± 4.7 |
| Aortic valve area, cm2* | 0.67 ± 0.22 | 1.55 ± 0.36 | 1.72 ± 0.39 | 1.66 ± 0.49 |
| LVEF, % | 55 ± 11 | 55 ± 9 | 57 ± 7 | 57 ± 7 |
| Mitral regurgitation, mod/sev (%) | 16 | 13 | 7 | 8 |
Data are expressed as mean ± SD or number (percentage). * Significant change (p < 0.001) from baseline to 30 days and 6 months (paired Student t-test). LVEF, left ventricular ejection fraction; mod/sev, moderate/severe.
Figure 2.
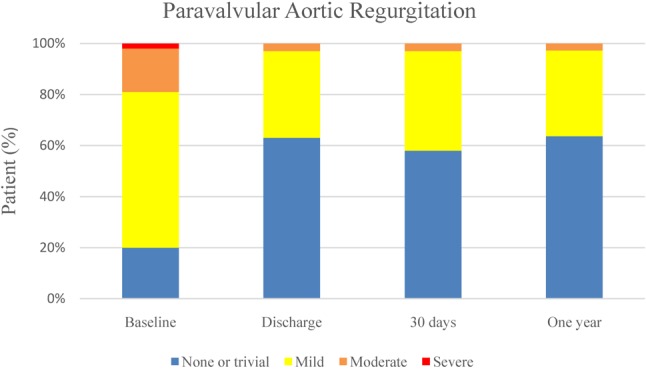
The percentage of patients with paravalvular aortic regurgitation at baseline, at discharge, 30 days, and 6 months after the procedure.
Multivariable analysis of all-cause mortality at one year
The Cox model identified access of TAVI as the significant univariate predictor of one-year all-cause mortality. Other predictors, such as logistic EuroSCORE and eGFR, showed some evidence of increased one-year all-cause mortality risk, although they were not statistically significant (Table 6). A multivariable analysis showed that the predictors of increased all-cause mortality at one year were non-TF TAVI (HR 4.81; 95% CI 1.66-14.09; p = 0.004), and advanced chronic kidney disease (CKD) (stages 4-5, defined as eGFR ≤ 30 mL/min) (HR 3.13; 95% CI 1.07-9.09; p = 0.036).
Table 6. Summary and comparison of outcomes with four of the most important national registries or trials.
| Taipei VGH (n = 100) | ADVANCE20 (n = 1015) | CoreValve US trial extreme surgical risk21 (n = 489) | TVT22 (n = 26414) | GARY23 (n = 15964) | |
| EuroSCORE (%) | 21.5 | 19.3 | 22.6 | - | 18.3 |
| MCV/ESV (%) | 84/16 | 100/0 | 100/0 | - | 37.7/52.6 |
| Posptocedural AR, moderate to severe (%) | 3.0 | 16.2 | 10.5 | 5.1 | 5.8 |
| Stroke (%) | 1.0 | 3.0 | 4.0 | 2.1 | 1.5 |
| Major vascular complication (%) | 3.0 | 10.9 | 8.2 | 4.9 | 4.1 |
| Permanent pacemaker (%) | 5.1 | 26.3 | 21.6 | 10.0 | 17.5 |
| 30-day mortality (%) | 4.0 | 4.5 | 8.4 | 4.9 (in-hospital) | 5.2 |
| 1-year mortality (%) | 14.0 | 18.4 | 24.3 | 23.7 | 24.3 |
AR, aortic regurgitation; ESV, Edwards Sapien or Sapien XT devices; GARY, German Aortic Valve Registry; MCV, Medtronic CoreValve; TVT, The Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry; VGH, Veterans General Hospital.
DISCUSSION
In Taiwan, this was the first study reporting the first 100 consecutive patients undergoing TAVI from a single center in the treatment of high-risk and inoperable patients with severe AS. The overall device success rate of 95% is encouraging, suggesting that with careful planning and appropriate technique, immediate procedural success can be achieved in most patients in whom the procedure is attempted.
TAVI is a widely accepted alternative to surgical aortic valve replacement (SAVR) among inoperable patients or selected high-risk patients with severe AS. The two devices in main stream use are the MCV and the ESV. The self-expanding MCV and the balloon-expandable ESV were approved in Taiwan in December 2012 and December 2015, respectively. The use of both devices is complementary, and makes TAVI feasible for patients with a wide array of anatomic dimensions.
The standard approach for both types of valves developed for TAVI is through the transfemoral route because it is minimally invasive and feasible under conscious sedation using a totally percutaneous approach. Although significant technical improvements in sheath diameter and delivery catheter design have been achieved, the transfemoral approach is contrain dicated in patients with vessel diameter less than 6 mm, in cases of severe tortuosity or calcification of the femoral or iliac arteries, or in those undergoing previous iliofemoral surgery or stent implantation. Therefore, alternative routes for TAVI delivery have been developed, including transapical access for the ESV, trans-subclavian access for the MCV, and the transaortic access for both prostheses. Recently, the unconventional carotid artery access has been described for both prostheses. In our cohort, TF route was used in 83% of procedures and was less frequently adopted for implantation of the ESV than for the MCV (43.8% vs. 90.5%, p < 0.001). Since almost two-thirds of the ESVs were implanted in 2010 when only the earlier generation RetroFlex system was available, which requires the use of larger diameter 22-F to 24-F sheaths. Seventeen of our TAVI procedures were performed through five alternative approaches, such as transapical, direct aortic, trans-subclavian, transcarotid, and transabdominal access, when the TF route was not feasible. Using various access routes ensures that all of our patients can be treated.
Our study allowed for an objective evaluation of ‘real-world’ outcomes. Table 6 summarizes and compares our outcomes with four of the most important national registries or trials.20-23 Overall, our results are encouraging. Accumulating data have linked device failure,24 the occurrence of more-than-mild PVL after TAVI,25,26 stroke,27 and major vascular complications,26 with significantly increased long-term mortality after TAVI. In our cohort, only three patients experienced post-procedural moderate PVL, lower than those in other reports. This difference might be explained by the pre-procedural careful planning and meticulous implantation technique. In addition, balloon sizing, as suggested by Patsalis et al.,28 was routinely performed when there was uncertainty as to the annulus dimensions based on poor computed tomography quality, when the measurements fall in the "grey zone" between two valve sizes, and in the following unclear anatomical situations: bicuspid aortic valve, presence of mitral prosthesis, and short coronary ostia distances.
MCV implantation is frequently associated with atrioventricular block requiring pacemaker placement, possibly arising from greater expansion into the left ventricular outflow tract with compression of the septal conduction tissues. Accordingly, the need for permanent pacemaker placement after MCV implantation has been reported to be from 25.8%-33.0% of patients.29,30 In our study, the rate of permanent pacemaker requirement was only 5.1%, one of the lowest observed to date.29,30 That might result from our high implantation strategy for the MCV system at a target depth of ≤ 6 mm below the annulus. The importance of the correct implantation depth of the MCV was originally highlighted by Piazza et al.31 Recently, Petronio et al.32 demonstrated that a high implantation depth of ≤ 6 mm using the MCV system allowed for are duction in new pacemaker implantation (13.3% vs. 21.1%), and that a depth shallower than 4 mm was associated with a pacemaker rate of 6.1%. Our target implantation depth for CoreValve is between 2 and 4 mm. This high implantation strategy was achieved by coordination between two implanters: the second implanter maintained the CoreValve delivery system along the outer curvature of the aortic root by constantly applying tension on the Super stiff guidewires, while, the first implanter released the valve very slowly during the first third of the deployment in order to be able to precisely adjust the starting depth and to reposition the delivery catheter before full annular engagement of the CoreValve.
The incidences of major vascular complication was 3% in our series, and all of them were caused by left ventricle perforated by the Amplatz Super stiff guidewires. With the introduction of pre-shaped dedicated TAVI guidewires, such as SAFARI (Boston Scientific, Marlborough, MA, USA) and Confida Brecker Guidewire (Medtronic, Minneapolis, MN, USA), we would expect the complication of ventricular perforation by a stiff wire could be eradicated. Coronary obstruction occurred in two of the MCV recipients: one with low-lying ostia of the left coronary artery and the other with bicuspid aortic valve. Although a large multicenter registry33 reported that coronary obstruction following TAVI led to a 30-day mortality rate of 40.9%, both of our patients had survived at the 6-month follow-up.
The multivariate prediction model in the present study showed that non-TF access was a significant predictor of cardiovascular-related mortality at the one-year follow-up. Similarly, the PARTNER trial and SOURCE XT registry34 reported that the non-TF approach had one of the highest HRs for one-year mortality. Worse outcomes with a non-TF approach were also demonstrated in FRANCE-235 and the UK (United Kingdom) TAVI Registry.36 The PARTNER trial demonstrated that, in matched patients with similar degrees of peripheral arterial disease and extensive cardiovascular risk factors, transapical-TAVR is associated with greater periprocedural morbidity, mortality and prolonged recovery than TF-TAVR.37 We also demonstrated that patients with advanced CKD (stages 4-5), but not moderate CKD (stage 3), was a predictor of one-year mortality, consistent with other studies.38-41 A meta-analysis evaluating the impact of renal dysfunction in 32,131 TAVR patients showed that advanced stages of CKD were associated with significantly higher incidences of bleeding, AKI, and mid-term mortality.42 This meta-analysis also noted that postprocedural stroke occurred more frequently in patients with stage 4 CKD than with stage 1 and 2.42 However, other data have demonstrated that patients with advanced CKD may still benefit from the TAVI procedure because of improvement in functional status (New York Heart Association class) and absence of valve hemodynamic anomalies.38 Further studies are needed to address this issue by improved risk stratification facilitating proper decision-making for such challenging patients.
CONCLUSIONS
In conclusion, our data demonstrated that TAVI shows good early and one-year outcomes in terms of survival, technical success, valve-related adverse events and haemodynamic performance in selected extreme high-risk elderly patients with severe aortic stenosis. With careful planning, meticulous implantation technique, and various alternative approaches, it can be applied in a wide range of patients.
Acknowledgments
We would like to thank Yuan-Chen Hsieh for assistance with the data collection.
REFERENCES
- 1.Bonow RO, Carabello BA, Chatterjee K, et al. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients with Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. 2008;15:e523–e661. doi: 10.1161/CIRCULATIONAHA.108.190748. [DOI] [PubMed] [Google Scholar]
- 2.Iung B, Cachier A, Baron G, et al. Decision-making in elderly patients with severe aortic stenosis: why are so many denied surgery? Eur Heart J. 2005;26:2714–2720. doi: 10.1093/eurheartj/ehi471. [DOI] [PubMed] [Google Scholar]
- 3.Bach DS, Siao D, Girard SE, et al. Evaluation of patients with severe symptomatic aortic stenosis who do not undergo aortic valve replacement. Circ Cardiovasc Qual Outcomes. 2009;2:533–539. doi: 10.1161/CIRCOUTCOMES.109.848259. [DOI] [PubMed] [Google Scholar]
- 4.Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–1607. doi: 10.1056/NEJMoa1008232. [DOI] [PubMed] [Google Scholar]
- 5.Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic valve replacement in high-risk patients. N Engl J Med. 2011;364:2187–2198. doi: 10.1056/NEJMoa1103510. [DOI] [PubMed] [Google Scholar]
- 6.Adams DH, Popma JJ, Reardon MJ, et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;370:1790–1798. doi: 10.1056/NEJMoa1400590. [DOI] [PubMed] [Google Scholar]
- 7.Thyregod HG, Steinbruchel DA, Ihlemann N, et al. Transcatheter versus surgical aortic valve replacement in patients with severe aortic valve stenosis: 1-year results from the all-comers NOTION randomized clinical trial. J Am Coll Cardiol. 2015;65:2184–2194. doi: 10.1016/j.jacc.2015.03.014. [DOI] [PubMed] [Google Scholar]
- 8.Giordana F, D'Ascenzo F, Nijhoff F, et al. Meta-analysis of predictors of all-cause mortality after transcatheter aortic valve implantation. Am J Cardiol. 2014;114:1447–1455. doi: 10.1016/j.amjcard.2014.07.081. [DOI] [PubMed] [Google Scholar]
- 9.Kappetein AP, Head SJ, Généreux P, et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document. J Am Coll Cardiol. 2012;60:1438–1454. doi: 10.1016/j.jacc.2012.09.001. [DOI] [PubMed] [Google Scholar]
- 10.Chen YH, Hsu TL, Wu MH, et al. The acute and 3-month outcomes of transcatheter aortic valve implantation in Taiwan. Acta Cardiol Sin. 2011;27:213–220. [Google Scholar]
- 11.Yuan YT, Chen YH, Chen PL, et al. One-year results of transcatheter aortic valve implantation as an alternative treatment for severe aortic stenosis in high-risk patients. J Chin Med Assoc. 2013;76:698–702. doi: 10.1016/j.jcma.2013.08.007. [DOI] [PubMed] [Google Scholar]
- 12.Fraccaro C, Napodano M, Tarantini G, et al. Expanding the eligibility for transcatheter aortic valve implantation the trans-subclavian retrograde approach using the III generation CoreValve revalving system. JACC Cardiovasc Interv. 2009;2:828–833. doi: 10.1016/j.jcin.2009.06.016. [DOI] [PubMed] [Google Scholar]
- 13.Bruschi G, De Marco F, Botta L, et al. Direct aortic access for transcatheter self-expanding aortic bioprosthetic valves implantation. Ann Thorac Surg. 2012;94:497–503. doi: 10.1016/j.athoracsur.2012.04.021. [DOI] [PubMed] [Google Scholar]
- 14.Leu HB, Chang HH, Lin SM, Chen YH. Double trouble for transcatheter aortic valve implantation: a patient with no vascular access and high-risk features for bilateral coronary obstruction. Eur Heart J. Advance Access published October 17, 2016. doi: 10.1093/eurheartj/ehw083. [DOI] [PubMed] [Google Scholar]
- 15.Modine T, Sudre A, Delhaye C, et al. Transcutaneous aortic valve implantation using the left carotid access: feasibility and early clinical outcomes. Ann Thorac Surg. 2012;93:1489–1494. doi: 10.1016/j.athoracsur.2012.01.030. [DOI] [PubMed] [Google Scholar]
- 16.Lichtenstein SV, Cheung A, Ye J, et al. Transapical transcatheter aortic valve implantation in humans: initial clinical experience. Circulation. 2006;114:591–596. doi: 10.1161/CIRCULATIONAHA.106.632927. [DOI] [PubMed] [Google Scholar]
- 17.Toggweiler S, Gurvitch R, Leipsic J, et al. Percutaneous aortic valve replacement: vascular outcomes with a fully percutaneous procedure. J Am Coll Cardiol. 2012;59:113–118. doi: 10.1016/j.jacc.2011.08.069. [DOI] [PubMed] [Google Scholar]
- 18.Webb JG, Pasupati S, Humphries K, et al. Percutaneous transarterial aortic valve replacement in selected high-risk patients with aortic stenosis. Circulation. 2007;116:755–763. doi: 10.1161/CIRCULATIONAHA.107.698258. [DOI] [PubMed] [Google Scholar]
- 19.Leu HB, Chang HH, Wu MH, Chen YH. Four-year follow-up of acquired aorto-right ventricular fistula after transcatheter aortic valve implantation. Eur Heart J. 2016;37:2679. doi: 10.1093/eurheartj/ehv716. [DOI] [PubMed] [Google Scholar]
- 20.Linke A, Wenaweser P, Gerckens U, et al. Treatment of aortic stenosis with a self-expanding transcatheter valve: the International Multi-centre ADVANCE Study. Eur Heart J. 2014;35:2672–2684. doi: 10.1093/eurheartj/ehu162. [DOI] [PubMed] [Google Scholar]
- 21.Popma JJ, Adams DH, Reardon MJ, et al. Transcatheter aortic valve replacement using a self-expanding bioprosthesis in patients with severe aortic stenosis at extreme risk for surgery. J Am Coll Cardiol. 2014;63:1972–1981. doi: 10.1016/j.jacc.2014.02.556. [DOI] [PubMed] [Google Scholar]
- 22.Holmes DR, Jr., Nishimura RA, Grover FL, et al. Annual outcomes with transcatheter valve therapy: from the STS/ACC TVT Registry. J Am Coll Cardiol. 2015;66:2813–2823. doi: 10.1016/j.jacc.2015.10.021. [DOI] [PubMed] [Google Scholar]
- 23.Walther T, Hamm CW, Schuler G, et al. Perioperative results and complications in 15,964 transcatheter aortic valve replacements: prospective data from the GARY Registry. J Am Coll Cardiol. 2015;65:2173–2180. doi: 10.1016/j.jacc.2015.03.034. [DOI] [PubMed] [Google Scholar]
- 24.Clerfond G, Pereira B, Innorta A, et al. Comparison of outcomes after one-versus-two transcatheter aortic valve implantation during a same procedure (from the FRANCE2 Registry). Am J Cardiol. 2015;115:1273–1280. doi: 10.1016/j.amjcard.2015.01.560. [DOI] [PubMed] [Google Scholar]
- 25.Tamburino C, Capodanno D, Ramondo A, et al. Incidence and predictors of early and late mortality after transcatheter aortic valve implantation in 663 patients with severe aortic stenosis. Circulation. 2011;123:299–308. doi: 10.1161/CIRCULATIONAHA.110.946533. [DOI] [PubMed] [Google Scholar]
- 26.Kodali SK, Williams MR, Smith CR, et al. Two-year outcomes after transcatheter or surgical aortic-valve replacement. N Engl J Med. 2012;366:1686–1695. doi: 10.1056/NEJMoa1200384. [DOI] [PubMed] [Google Scholar]
- 27.Eggebrecht H, Schmermund A, Voigtländer T, et al. Risk of stroke after transcatheter aortic valve implantation (TAVI): a meta-analysis of 10,037 published patients. Eurointervention. 2012;8:129–138. doi: 10.4244/EIJV8I1A20. [DOI] [PubMed] [Google Scholar]
- 28.Patsalis PC, Al-Rashid F, Neumann T, et al. Preparatory balloon aortic valvuloplasty during transcatheter aortic valve implantation for improved valve sizing. JACC Cardiovasc Interv. 2013;6:965–971. doi: 10.1016/j.jcin.2013.05.006. [DOI] [PubMed] [Google Scholar]
- 29.Erkapic De Rosa S, Kelava A, Lehmann R, et al. Risk for permanent pacemaker after transcatheter aortic valve implantation: a comprehensive analysis of the literature. J Cardiovasc Electrophysiol. 2012;23:391–397. doi: 10.1111/j.1540-8167.2011.02211.x. [DOI] [PubMed] [Google Scholar]
- 30.Khawaja MZ, Rajani R, Cook A, et al. Permanent pacemaker insertion after CoreValve transcatheter aortic valve implantation: incidence and contributing factors (the UK CoreValve Collaborative). Circulation. 2011;123:951–960. doi: 10.1161/CIRCULATIONAHA.109.927152. [DOI] [PubMed] [Google Scholar]
- 31.Piazza N, Onuma Y, Jesserun E, et al. Early and persistent intraventricular conduction abnormalities and requirements for pacemaking after percutaneous replacement of the aortic valve. JACC Cardiovasc Interv. 2008;1:310–316. doi: 10.1016/j.jcin.2008.04.007. [DOI] [PubMed] [Google Scholar]
- 32.Petronio AS, Sinning JM, Van Mieghem N, et al. Optimal implantation depth and adherence to guidelines on permanent pacing to improve the results of transcatheter aortic valve replacement with the Medtronic CoreValve System: The CoreValve Prospective, International, Post-Market ADVANCE-II Study. JACC Cardiovasc Interv. 2015;8:837–846. doi: 10.1016/j.jcin.2015.02.005. [DOI] [PubMed] [Google Scholar]
- 33.Ribeiro HB, Webb JG, Makkar RR, et al. Predictive factors, management, and clinical outcomes of coronary obstruction following transcatheter aortic valve implantation: insights from a large multicenter registry. J Am Coll Cardiol. 2013;62:1552–1562. doi: 10.1016/j.jacc.2013.07.040. [DOI] [PubMed] [Google Scholar]
- 34.Schymik G, Lefèvre T, Bartorelli AL, et al. European experience with the second-generation Edwards SAPIEN XT transcatheter heart valve in patients with severe aortic stenosis: 1-year outcomes from the SOURCE XT Registry. JACC Cardiovasc Interv. 2015;8:657–669. doi: 10.1016/j.jcin.2014.10.026. [DOI] [PubMed] [Google Scholar]
- 35.Gilard M, Eltchaninoff H, Iung B, et al. Registry of transcatheter aortic-valve implantation in high-risk patients. N Engl J Med. 2012;366:1705–1715. doi: 10.1056/NEJMoa1114705. [DOI] [PubMed] [Google Scholar]
- 36.Fröhlich GM, Baxter PD, Malkin CJ, et al. Comparative survival after transapical, direct aortic, and subclavian transcatheter aortic valve implantation (data from the UK TAVI registry). Am J Cardiol. 2015;116:1555–1559. doi: 10.1016/j.amjcard.2015.08.035. [DOI] [PubMed] [Google Scholar]
- 37.Blackstone EH, Suri RM, Rajeswaran J, et al. Propensity-matched comparisons of clinical outcomes after transapical or transfemoral transcatheter aortic valve replacement: a Placement of Aortic Transcatheter Valves (PARTNER)-I trial substudy. Circulation. 2015;131:1989–2000. doi: 10.1161/CIRCULATIONAHA.114.012525. [DOI] [PubMed] [Google Scholar]
- 38.Allende R, Webb JG, Munoz-Garcia AJ, et al. Advanced chronic kidney disease in patients undergoing transcatheter aortic valve implantation: insights on clinical outcomes and prognostic markers from a large cohort of patients. Eur Heart J. 2014;35:2685–2696. doi: 10.1093/eurheartj/ehu175. [DOI] [PubMed] [Google Scholar]
- 39.Yamamoto M, Hayashida K, Mouillet G, et al. Prognostic value of chronic kidney disease after transcatheter aortic valve implantation. J Am Coll Cardiol. 2013;62:869–877. doi: 10.1016/j.jacc.2013.04.057. [DOI] [PubMed] [Google Scholar]
- 40.D'Ascenzo F, Moretti C, Salizzoni S, et al. 30 days and midterm outcomes of patients undergoing percutaneous replacement of aortic valve according to their renal function: a multicenter study. Int J Cardiol. 2013;167:1514–1518. doi: 10.1016/j.ijcard.2012.04.161. [DOI] [PubMed] [Google Scholar]
- 41.Thourani VH, Forcillo J, Beohar N, et al. Impact of preoperative chronic kidney disease in 2,531 high-risk and inoperable patients undergoing transcatheter aortic valve replacement in the PARTNER Trial. Ann Thorac Surg. 2016;102:1172–1180. doi: 10.1016/j.athoracsur.2016.07.001. [DOI] [PubMed] [Google Scholar]
- 42.Gargiulo G, Capodanno D, Sannino A, et al. Moderate and severe preoperative chronic kidney disease worsen clinical outcomes after transcatheter aortic valve implantation: meta-analysis of 4992 patients. Circ Cardiovasc Interv. 2015;8:e002220. doi: 10.1161/CIRCINTERVENTIONS.114.002220. [DOI] [PubMed] [Google Scholar]