

Description
A 35-year-old man was referred to the Sarcoma service with a 2-year history of worsening back pain, left-sided radicular pain and a mass on CT scan. In the 6 months following the onset of the back pain, he developed progressive numbness and paraesthesia in the L2 dermatome. This was worse on standing. On clinical examination, power was unaffected but somewhat limited by pain. No ‘red flag’ symptoms were present (table 1). The CT scan demonstrated a large retroperitoneal mass on the left with invasion into the L2 vertebra (figure 1 and 2) and bilateral pulmonary metastases. USS-guided biopsy revealed high grade alveolar soft part sarcoma. He was started on palliative radiotherapy (30 Gy and 10 fractions) and given six cycles of doxorubicin and ifosfamide. Imaging at 8 months postdiagnosis has indicated stable disease.
Table 1.
‘Red flag’ symptoms of back pain4
| Sphincter and gait disturbance | Saddle anaesthesia | Severe or progressive motor loss |
| Widespread neurological deficit | Age <20 or >55 years | Previous malignancy |
| Systemic illness | Human inmmunodeficiency virus | Weight loss |
| Intravenous drug use | Steroid use | Structural deformity |
| Non-mechanical pain (no relief with bed rest) | Fever | Thoracic pain |
Figure 1.

Tumour causing erosive destruction of the left lateral aspect of the L2 vertebrae.
Alveolar soft part sarcoma is a very rare condition, believed to account for <1% of all soft tissue tumours.1 Diagnosis is made by a combination of histology and immunohistochemistry; looking for strong nuclear expression of transcription factor 3.1 Patients are typically young and present with metastases.
Complete wide surgical excision by a sarcoma surgeon is advised in cases where the disease remains localised. Recurrence following complete excision is rare, but metastases may still occur years later.2 In patients with localised disease survival rates of 60% at 5 years and 38% at 10 years have been documented.2 Chemoradiotherapy for metastatic disease has been documented in the literature, with limited success.3
Figure 2.
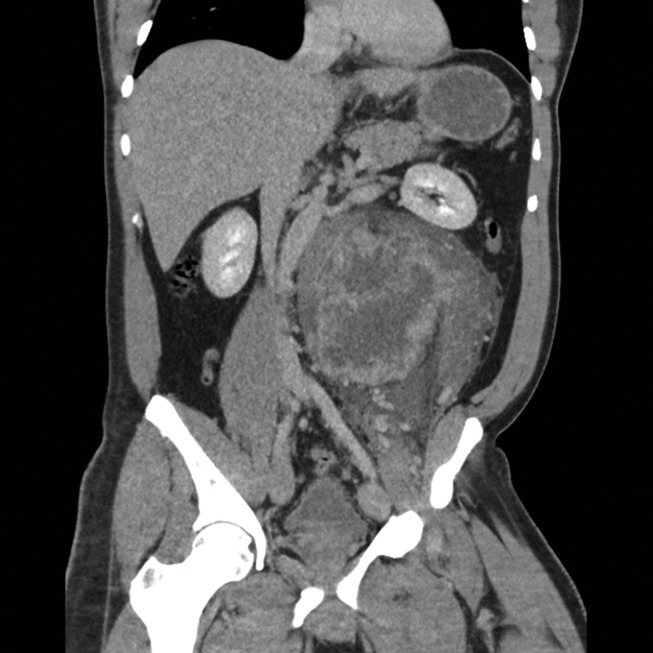
16.4×12.4×19.4 cm mass with central necrosis, closely related to the left psoas muscle.
Learning points.
This unfortunate case serves to remind us that despite the absence of ‘red flag’ symptoms, clinical suspicion should be raised in the presence of progressively worsening symptoms over a short duration.
Footnotes
Contributors: ATT and SJF drafted the article, which was edited for submission by AD. The patient was admitted under and reviewed by DG who suggested submission.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Folpe AL, Deyrup AT. Alveolar soft-part sarcoma: a review and update. J Clin Pathol 2006;59:1127–32.doi:10.1136/jcp.2005.031120 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Lieberman PH, Brennan MF, Kimmel M, et al. . Alveolar soft-part sarcoma. A clinico-pathologic study of half a century. Cancer 1989. ;63:1–13.doi:10.1002/1097-0142(19890101)63:1<1::AID-CNCR2820630102>3.0.CO;2-E [DOI] [PubMed] [Google Scholar]
- 3. Reichardt P, Lindner T, Pink D, et al. . Chemotherapy in alveolar soft part sarcomas. what do we know? Eur J Cancer 2003;39:1511–6. [DOI] [PubMed] [Google Scholar]
- 4. The Royal College of Radiologists. Acute back pain with potentially serious (red flag) features iRefer: making the best use of clinical radiology. London: The Royal College of Radiologists, 2012. http://irefer.org.uk/images/pdfs/msk_m05_abstract.pdf. [Google Scholar]