

Abstract
Isolated gastric Crohn’s disease with initial presentation related to gastric outlet obstruction is an unusual clinicopathological entity. We undertake here a literature review of this rare initial presentation of isolated gastric Crohn’s disease and discuss the formidable diagnostic and therapeutic challenges encountered in such patients.
Keywords: Gastroenterology, Endoscopy
Background
Crohn’s disease (CD) is a chronic idiopathic inflammatory disease characterised by segmental and transmural involvement of gastrointestinal tract. Colon and small intestine are the most common sites that account for 40% and 30% cases of CD, respectively. However, isolated gastric involvement occurs only in 0.7% of all the cases with gastrointestinal CD.1–4 In the largest case series published to date, only 7 of 940 patients with CD who presented at a major Dutch university referral centre had isolated proximal CD.1–4
Isolated gastric CD typically presents with chronic non-specific gastritis-like symptoms such as nausea, vomiting, epigastric pain and weight loss.5–10 However, it is extremely rare for gastric CD to present atypically as early gastric outlet obstruction. In these cases, other possible aetiologies like non-steroidal anti-inflammatory drug use, Menetrier disease, gastrinoma, collagen vascular disease and various infections, including Helicobacter pylori, cytomegalovirus and Mycobacterium tuberculosis must be systematically ruled out.5 6
Endoscopic findings in patients with gastric CD include nodularity (93%), aphthous ulcers (64%), thickened antral folds (64%), linear ulcerations (55%) and antral narrowing (43%).6 The most widely used histological feature in the diagnosis is the presence of non-caseating granulomas.7–11 However, only 4%–11% of adult patients with CD have granulomas in biopsies, making the diagnosis of atypical isolated gastric CD more challenging.12 Furthermore, the anti-Saccharomyces cerevisiae antibody (ASCA) is a marker for CD with relatively good specificity, but poor sensitivity.5
In patients with histopathological features of granulomatous gastritis, it is essential to consider sarcoidosis, mucosa-associated lymphoid tissue lymphoma and tuberculosis in differential diagnosis of isolated gastric CD.13 Although malignancy is quite rare in this age group, clinicians should always take a detailed clinical and family history, particularly focusing on the risk factors of malignancy. Furthermore, malignant changes should also be ruled out while conducting the histopathological analysis for CD.
Case presentation
A 27-year-old woman presented with nausea, heartburn, bloating and postprandial vomiting for the last 3 months. Previously, she was treated with antibiotics and antacids as a suspected case of chronic gastritis, but she showed no significant improvement. She also reported occasional low-grade fevers, body aches, joint pain and back ache with an unintentional weight loss of 20 lb over the last 3 months. She denied any pre-existing gastrointestinal disease, skin rashes or enterocutaneous fistulas.
On presentation, she had a heart rate of 74 beats/min, blood pressure of 130/78 mm Hg and a respiratory rate of 20/min. She had no oral or genital ulcers and no signs of inflamed joints. Her systemic examination was unremarkable.
Investigations
Laboratory studies revealed white cell count 7.29×109/L, platelets 339×109/L and haemoglobin 9.5 g/dL with a mean corpuscular volume 88.9 fL. Her serum total protein level was 7.7 g/dL with albumin 4.5 g/dL. Erythrocyte sedimentation rate and C reactive protein were 22 mm/hour and 3.7 mg/L, respectively. Her liver and renal function tests were within the normal limits. She has normal serum calcium levels and the ACE levels were also within normal limits. A wide range of serological tests were performed, including an antineutrophilic cytoplasmic antibodies, anti-dsDNA, complement C3 and C4 levels, rheumatoid factor, anticyclic citrullinated peptide antibodies, ASCA, tissue transglutaminase IgG and IgA, serum IgA levels and T-cell-based blood tests for tuberculosis infection, all of which came out normal. Stool cultures were inconclusive for Clostridium difficile. Stool antigens and serological tests were negative for H. pylori. Chest radiography was unremarkable for bilateral hilar lymphadenopathy or parenchymal abnormalities.
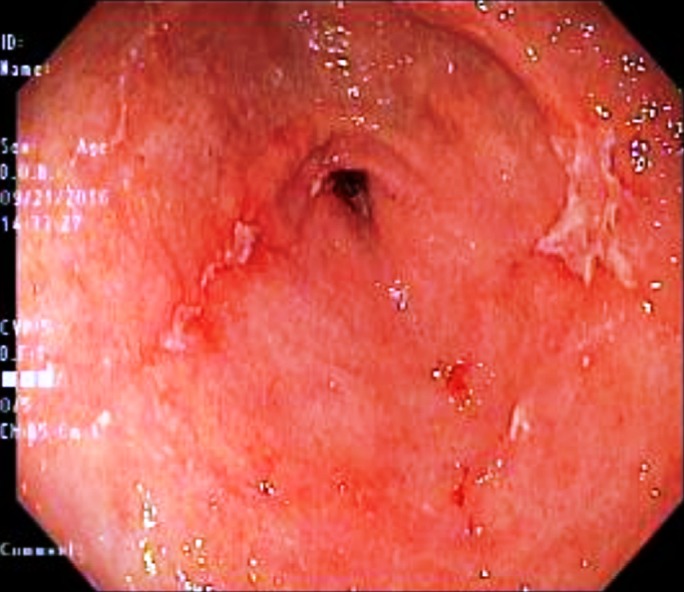
A contrast-enhanced CT showed distended stomach with ingested material (figure 1). Enteric contrast material was seen through small bowel loops to the level of the hepatic flexure of the colon (figure 2). Esophagogastroduodenoscopy (EGD) showed erythematous edematous mucosa in the stomach (figure 3). A significant narrowing of the pylorus was evident, which confirmed the partial gastric outlet obstruction in the present patient (figure 4). Multiple biopsies were taken from the suspicious gastric lesions. Duodenum appeared normal on EGD. Furthermore, colonoscopy was performed to rule out additional abnormalities in terminal ileum and colon, but it was normal. Biopsy specimens from duodenum, terminal ileum and colon were obtained.
Figure 1.

A contrast-enhanced CT showing distended stomach with ingested material.
Figure 2.

Enteric contrast material seen through small bowel loops to the level of the hepatic flexure of the colon.
Figure 3.

Esophagogastroduodenoscopy revealing erythematous edematous mucosa in stomach.
Figure 4.
Upper endoscopy showing pyloric stenosis confirming the partial gastric outlet obstruction.
Histopathological examination of the gastric biopsy specimens subsequently demonstrated patchy destruction and microabscesses of the deep gastric glands with relative sparing of the superficial mucosa along with changes in line with chronic active erosive gastritis (figure 5). Non-caseating granulomas composed of epithelioid cells and multinucleated giant cells were appreciated in random gastric biopsies. No intestinal metaplasia or evidence of H. pylori and cytomegalovirus infections were documented. Duodenal, terminal ileal and colonic biopsies were unremarkable for inflammation or ulceration. On the basis of clinical presentation, endoscopic findings, histopathological features and exclusion of possible aetiologies for granulomatous gastritis, the present patient was diagnosed with isolated gastric CD.
Figure 5.

Histopathological examination of the gastric biopsy specimens showing patchy destruction and microabscesses of the deep gastric glands with relative sparing of the superficial mucosa. Chronic active erosive gastritis was evident.
Treatment
Initially, a standard pyloric dilator with a balloon size of 10 mm was employed along with high dose of omeprazole, but it could not serve the purpose. Furthermore, a slim dilator (balloon size, 5.9 mm) was also unable to traverse through the pylorus in our patient. Therein, a superslim CRE balloon dilator (Boston Scientific, Natick, Massachusetts, USA) with the balloon size of 4.9 mm was used that successfully dilated the narrowed pylorus (figure 6). The patient was then started on oral prednisone therapy.
Figure 6.

An uneventful endoscopic balloon dilation of pyloric stenosis was performed.
Outcome and follow-up
The CD-related gastric outlet obstruction in the present case was initially treated with a single endoscopic dilatation along with corticosteroid therapy. The patient did not require any nasogastric (NG) feeding and she tolerated regular diet quite well. She showed a remarkable response on 1-month follow-up with the complete resolution of her symptoms. Oral prednisone was then tapered off and she was initiated on infliximab as the maintenance therapy. At the follow-up after 6 months, she continues to do well without any gastric outlet obstruction symptoms and she has started gaining weight appropriately.
Discussion
Management of isolated gastric CD may be divided into acute and chronic. Laparoscopic or endoscopic surgical interventions have been considered as acute management. In terms of chronic management, various therapeutic agents have been employed for upper gastrointestinal CD. Few case reports demonstrated promising results with inhaled and systemic corticosteroids.14 Furthermore, thiopurines and methotrexate have been described for remission in CD; however, there are no reports specific to isolated gastric CD.15 The efficacy of anti-tumour necrosis factor therapy and calcineurin inhibitors for severe upper intestinal CD has been described in single case reports.13–16
We conducted a literature search of PubMed database regarding the presenting symptoms of isolated gastric CD. It showed only four case reports initially presenting with gastric outlet obstruction.6–9 Majority of these patients were middle-aged females. The most common initial manifestations included nausea, vomiting and epigastric discomfort. Endoscopy revealed inflammatory changes of the gastric mucosa and narrowing of the pylorus as the most common findings.
The exact pathogenesis of the CD-associated pyloric stenosis is yet to be determined. Previously, prolonged inflammation and fibrosis has been designated to be the culprit behind gastrointestinal strictures in patients with CD.17 Therefore, we assume that the pyloric stenosis has the same pathophysiological basis that lead to gastric outlet obstruction. The cases with isolated gastric CD with initial presentation dominated by gastric outlet obstruction were not only misdiagnosed, but underwent exhausting surgical interventions.6–10
In the previously reported cases, Scheck et al 6 opted for Billroth II distal gastrectomy with retrocolic gastrojejunostomy in their case. The gastrectomy specimen confirmed the diagnosis of gastric CD and the patient was subsequently initiated on azathioprine therapy. Burbige carried out vagotomy and Finney pyloroplasty for his apparent peptic disease and pyloric channel ulcer. However, his symptoms persisted. He was then initiated on a combination therapy with sulfasalazine and prednisone for the suspected CD with a dramatic response and was finally diagnosed.7 In the third case by Awad et al8, a short course of corticosteroids and total parenteral nutrition was employed that successfully treated the isolated gastric CD. Similarly, another report highlighted prednisolone as initial therapy with 6-mercaptopurine as the maintenance therapy demonstrating a remarkable response.9
Unfortunately, the present patient was also unnecessarily treated as a case of chronic gastritis owing to the diagnostic confusion secondary to this atypical and rare presentation of isolated gastric CD. However, the detailed clinical evaluation, consistent endoscopic features, multiple histopathological examinations and exclusion of other possible aetiologies helped us arriving at the definitive diagnosis of isolated gastric CD. The present patient is unique because of the degree of the narrowness of the pylorus.
We initially used a standard balloon dilator. Normally, a catheter of this size would just go into pylorus without any difficulty, but in the present case, we had to dilate the pylorus by employing a superslim CRE balloon dilator (Boston Scientific) with a balloon size of 4.9 mm. The patient showed a dramatic response to single endoscopic balloon dilatation followed by medical therapy with corticosteroids resulting in resolution of his symptoms. Since then, she has been on infliximab maintenance therapy without recurrence of her symptoms. Previously, balloon dilatation procedure for the management of gastric outlet obstruction had been associated with high recurrence rates. However, our patient showed a remarkable response on 6-month follow-up with no signs of disease recurrence.
While the present patient was cured with balloon dilatation and medical therapy, she did not undergo an unnecessary surgical intervention. Therefore, surgical therapy in isolated gastric CD can be indicated for ulcers not responding to medical therapy, massive bleeding, in gastric outlet obstructions for which balloon dilatation is unsuccessful or in cases where gastric fistulas have developed. However, further clinical studies are warranted to broaden the scope of our knowledge on isolated gastric CD and to frame guidelines to standardise the care of these patients.
Learning points.
Isolated gastric Crohn’s disease (CD) initially presenting with gastric outlet obstruction symptoms is an extremely unusual event in clinical practice.
Endoscopic biopsy along with laboratory investigations is an effective tool to hit the correct diagnosis of isolated gastric CD by exclusion of various causes of granulomatous gastritis.
A high index of clinical suspicion and prompt diagnosis should detect isolated CD before it results in pyloric stenosis and gastric outlet obstruction. This may prevent untoward morbidity and mortality related to disease and treatment in such patients.
Footnotes
Contributors: FI and WU wrote the discussion and did literature review. QH and KS wrote the presentation and summary.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Nugent FW, Roy MA. Duodenal Crohn’s disease: an analysis of 89 cases. Am J Gastroenterol 1989;84:249–54. [PubMed] [Google Scholar]
- 2. Wagtmans MJ, Verspaget HW, Lamers CB, et al. Clinical aspects of Crohn’s disease of the upper gastrointestinal tract: a comparison with distal Crohn’s disease. Am J Gastroenterol 1997;92:1467–71. [PubMed] [Google Scholar]
- 3. Grübel P, Choi Y, Schneider D, et al. Severe isolated Crohn’s-like disease of the gastroduodenal tract. Dig Dis Sci 2003;48:1360–5. 10.1023/A:1024123613071 [DOI] [PubMed] [Google Scholar]
- 4. Ingle SB, Pujari GP, Patle YG, et al. An unusual case of Crohn’s disease with isolated gastric involvement. J Crohns Colitis 2011;5:69–70. 10.1016/j.crohns.2010.10.001 [DOI] [PubMed] [Google Scholar]
- 5. Ingle SB, Adgaonkar BD, Jamadar NP, et al. Crohn’s disease with gastroduodenal involvement: Diagnostic approach. World J Clin Cases 2015;3:479 10.12998/wjcc.v3.i6.479 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Scheck SM, Ram R, Loveday B, et al. Crohn’s disease presenting as gastric outlet obstruction. J Surg Case Rep 2014;2014:rju128 10.1093/jscr/rju128 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Burbige EJ. Crohn’s disease of the stomach. West J Med 1977;126:397. [PMC free article] [PubMed] [Google Scholar]
- 8. Awad J, Farah R, Reshef R, et al. Pyloric stenosis as a presenting symptom of Crohn’s disease. J Gastrointestin Liver Dis 2006;15:175. [PubMed] [Google Scholar]
- 9. Ho CH, Sinatra FR, Pietzak MM. A 9-year-old girl with poor weight gain and postprandial vomiting. Gastroenterology 2015;148:904–5. 10.1053/j.gastro.2014.12.042 [DOI] [PubMed] [Google Scholar]
- 10. Wagtmans MJ, van Hogezand RA, Griffioen G, et al. Crohn’s disease of the upper gastrointestinal tract. Neth J Med 1997;50:S2–S7. 10.1016/S0300-2977(96)00063-0 [DOI] [PubMed] [Google Scholar]
- 11. Alcántara M, Rodriguez R, Potenciano JL, et al. Endoscopic and bioptic findings in the upper gastrointestinal tract in patients with Crohn’s disease. Endoscopy 1993;25:282–6. 10.1055/s-2007-1010315 [DOI] [PubMed] [Google Scholar]
- 12. Horjus Talabur Horje CS, Meijer J, Rovers L, et al. Prevalence of Upper Gastrointestinal lesions at primary diagnosis in adults with inflammatory bowel disease. Inflamm Bowel Dis 2016;22:1896–901. 10.1097/MIB.0000000000000786 [DOI] [PubMed] [Google Scholar]
- 13. Shapiro JL, Goldblum JR, Petras RE. A clinicopathologic study of 42 patients with granulomatous gastritis. is there really an "idiopathic" granulomatous gastritis? Am J Surg Pathol 1996;20:462–70. [DOI] [PubMed] [Google Scholar]
- 14. Ibrahim SH, Smyrk TC, Faubion WA. Treatment of isolated gastric Crohn’s disease with inhaled corticosteroids. Case Rep Gastroenterol 2008;2:363–8. 10.1159/000158543 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Leitner GC, Vogelsang H. Pharmacological- and non-pharmacological therapeutic approaches in inflammatory bowel disease in adults. World J Gastrointest Pharmacol Ther 2016;7:5–20. 10.4292/wjgpt.v7.i1.5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Firth M, Prather CM. Unusual gastric Crohn?s disease treated with infliximab - a case report. Am J Gastroenterol 2002;97:S190 10.1016/S0002-9270(02)05063-3 [DOI] [Google Scholar]
- 17. Chang CW, Wong JM, Tung CC, et al. Intestinal stricture in Crohn’s disease. Intest Res 2015;13:19–26. 10.5217/ir.2015.13.1.19 [DOI] [PMC free article] [PubMed] [Google Scholar]