

Description
A 16-year-old male patient with anorexia nervosa was admitted to our hospital because of unconsciousness. He was in hypoglycaemic shock, with a serum glucose level of 40 mg/dL, and recovered consciousness after a venous injection of glucose. The patient’s systolic blood pressure remained <70 mm Hg after he recovered consciousness. A 12-lead ECG showed Q waves and ST segment elevation in the precordial leads, and echocardiography showed hypokinesis of the midventricle and apex. Next, we performed coronary angiography, which revealed the absence of stenosis of the coronary arteries. Left ventriculography showed findings typical of takotsubo cardiomyopathy, apical ballooning with akinesis of the midventricle and apex and hyperkinetic basal segments (figure 1). 201Tl and iodofiltic acid (123)I-dual cardiac single-photon emission CT (SPECT) (figure 2A,B) at 1 week showed the absence of perfusion defect and fatty acid metabolism abnormality at the apex. Metaiodobenzylguanidine cardiac SPECT (figure 2C) at 2 weeks showed that sympathetic nerve innervation had occurred in the same area as the akinetic midventricle and apex. Echocardiography indicated complete recovery of cardiac wall motion 40 days after admission. In summary, the multiple SPECT images suggested that sympathetic nerve innervation is one of the leading pathophysiologies of takotsubo cardiomyopathy in the subacute phase.
Figure 1.
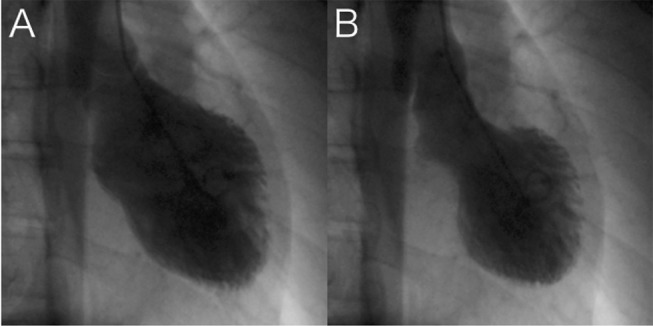
(A) Diastolic phase of left ventriculography. (B) Systolic phase of left ventriculography showing akinesis of the midventricle and apex.
Figure 2.
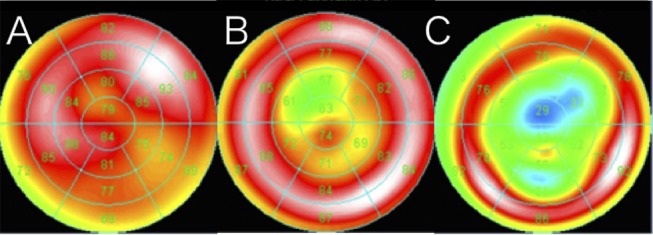
(A and B) 201Tl and iodofiltic acid (123)I-dual cardiac single-photon emission CT (SPECT) at 1 week showing the absence of perfusion defect and fatty acid metabolism abnormality at the apex. (C) Metaiodobenzylguanidine cardiac SPECT at 2 weeks showing sympathetic nerve innervation in the midventricle and apex.
Learning points.
Sympathetic nerve innervation is one of the leading pathophysiologies of takotsubo cardiomyopathy in the subacute phase.
Hypoglycaemic shock can lead to takotsubo cardiomyopathy.
Footnotes
Contributors: YI and YM were involved in diagnostic process, review of the literature and drafting of the manuscript.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.