

Abstract
An 83-year-old man with severe symptomatic aortic valve stenosis underwent transcatheter aortic valve implantation (TAVI) using a 29 mm SAPIEN XT valve. He was haemodynamically stable, but developed haemolytic anaemia. Transthoracic echocardiography conducted 7 days after TAVI revealed an abnormal continuous flow from the right sinus of Valsalva adjacent to the implanted valve to the right ventricle. The amount of shunt flow was considered small and the patient was managed with diuretics successfully. He was discharged from the hospital 35 days after TAVI. He was doing well at 9 months after TAVI, despite persistence of the aorto-right ventricular fistula on repeat echocardiographic examinations.
Keywords: Resuscitation, General surgery, Medical education
Background
Although transcatheter aortic valve implantation (TAVI) is now widely used, several serious complications can still occur during the procedure. Annulus rupture is rare, but is one of the most serious complications in TAVI. Aorto-right ventricular perforation is even rarer and its prognosis is still unclear. Herein, we report a case of late-onset aorto-right ventricular perforation after TAVI, which was successfully managed with medical therapy.
Case presentation
An 83-year-old man with severe symptomatic aortic valve stenosis was referred to our hospital. He was considered to have New York Heart Association (NYHA) functional class III heart failure. The patient had a history of hepatic cancer, hypertension, lumber spinal stenosis and mild dementia.
Investigations
Echocardiography showed a severely calcified tricuspid aortic valve with reduced left ventricular systolic function (ejection fraction = 35%). The aortic valve area calculated using the continuity equation was 0.36 cm2 with a peak/mean transvalvular gradient of 104/63 mm Hg. Multislice CT (MSCT) showed heavy calcification of all aortic valve cusps, and the right cusp had a 6.5 mm longitudinal calcification (figure 1). Calcification of the sinotubular junction to the ascending aorta was mild. The MSCT measurements showed the annulus area=604 mm2, the sinus of Valsalva=35 mm × 36 mm × 36 mm and the sinotubular junction=34 mm × 32 mm. The Society of Thoracic Surgeons 30-day predicted risk of mortality score calculated for surgical aortic valve replacement was 8.8%. In view of this, the patient was deemed to be a high-risk patient for surgical aortic valve replacement, and a TAVI via transfemoral approach using a 29 mm SAPIEN XT valve (Edwards Lifesciences, CA, USA) was planned.
Figure 1.

Multislice CT images. (A) Heavy calcification in all three aortic valve cusps. (B) A 6.5 mm longitudinal calcification in the right cusp.
Treatment
The patient underwent transfemoral TAVI under general anaesthesia. After crossing the stenotic aortic valve using a 5-Fr AL-1 diagnostic catheter with a straight guidewire, a Safari dedicated guidewire (Boston Scientific, Massachusetts, USA) was placed in the left ventricle. A predilatation was conducted using a 25 mm balloon under rapid right ventricular pacing at 200 bpm. Then, a 29 mm SAPIEN XT valve was implanted with −2 cc balloon volume. The transesophageal echocardiography and aortography revealed moderate perivalvular aortic regurgitation; thus, the valve balloon was reinflated twice with nominal and +2 cc balloon volume. The paravalvular aortic regurgitation was reduced to mild and the procedure was completed (figure 2). The patient developed complete atrioventricular block after the valve implantation and underwent permanent pacemaker implantation 6 days after the TAVI. The patient was haemodynamically stable, but developed haemolytic anaemia. The transthoracic echocardiography (TTE) conducted 7 days after the TAVI showed mild paravalvular aortic regurgitation and an abnormal continuous flow from the right sinus of Valsalva adjacent to the implanted valve to the right ventricle (figure 3). However, neither the aorto-ventricular fistula nor any other abnormalities were observed in the aortic wall around the implanted valve on contrast-enhanced MSCT. Aortography revealed a very subtle abnormal flow from the ascending aorta to the right ventricle. The amount of shunt flow was considered small and the patient was managed with diuretics successfully.
Figure 2.

Fluoroscopy images during transcatheter aortic valve implantation. (A) A 29 mm SAPIEN XT valve is implanted with +2 cc balloon volume. (B) Final aortography showing mild paravalvular regurgitation.
Figure 3.
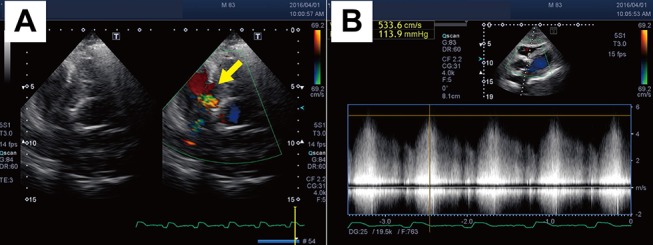
Transthoracic echocardiography images. (A) An abnormal colour jet (arrow) from the right sinus of Valsalva to the right ventricle. (B) The flow is continuous in systole and diastole.
Outcome and follow-up
The patient’s functional status improved to NYHA functional class I. However, he required prolonged hospitalisation due to disuse muscle atrophy of lower limbs. He was discharged from the hospital 35 days after the TAVI. He was doing well at 9 months after TAVI, despite persistence of the small aorto-right ventricular fistula (pulmonary blood flow/systemic blood flow ratio (Qp/Qs) =1) on repeat TTE examinations. The haemolytic anaemia is also mild and under control.
Discussion
Acquired aseptic intracardiac shunt is a rare complication after TAVI.1 Aorto-right ventricular fistula after TAVI is even rare. We found only six cases (table 1),2–7 in a literature search, thus, ours is the seventh reported case of aorto-right ventricular fistula following TAVI as a procedural complication. Severe calcification of the aortic valve and aggressive postdilation are the risk of this rare complication. Interestingly, all cases of aorto-right ventricular fistula were late-onset, which suggests that the mechanism of this complication is an erosion between the implanted valve edge and the aortic wall, resulting in late-onset perforation of the aortic wall. Six of the seven cases were treated with balloon expandable Edwards SAPIEN valves. This may indicate that erosion by the mechanical prosthetic valve struts is more severe with the balloon-expandable valve than the self-expandable valve. The prognoses varied. Two patients died after development of the aorto-right ventricular fistula; one died due to uncontrollable heart failure2 and the other died suddenly 3 months after the TAVI.4 Percutaneous closure using atrial septal occluders7 or coils3 was conducted when the shunt was significant. Although all aggressive treatments resulted in success, more evidence is required to establish a treatment strategy for this rare complication after TAVI.
Table 1.
Reports of aorto-right ventricular fistula after transcatheter aortic valve implantation
| References | Age/sex | Valve/size | Onset after TAVI | Qp/Qs | Management | Outcome |
| Shakoor et al 2 | 89/male | SAPIEN/29 mm | 30 days | 1.39 | Observation | Dead |
| Pilgrim et al 3 | 91/female | SAPIEN/26 mm | 1 month | 1.4 | Coil embolisation | Survived |
| Leroux et al 4 | 47/male | SAPIEN XT/26 mm | 3 weeks | NA | Observation | Dead (sudden death) |
| Leu et al 5 | 78/female | SAPIEN/26 mm | 2 weeks | 1.13 | Observation | Survived |
| García et al 6 | 85/male | CoreValve/29 mm | 72 hours | 1.53 | Observation | Survived |
| Nakamura et al 7 | 54/male | SAPIEN XT/29 mm | 5 days | 1.7 | ASO | Survived |
ASO, atrial septal occluder; NA, not applicable; Qp/Qs, pulmonary blood flow/systemic blood flow ratio; TAVI, transcatheter aortic valve implantation.
Learning points.
Aorto-right ventricular fistula is a rare complication after TAVI.
All reported cases were late-onset, which suggests that the mechanism of this complication is an erosion between the implanted valve edge and the aortic wall.
This complication is more frequently observed in patients with the balloon expandable valve than the self-expandable valve.
Percutaneous closure should be considered when the shunt is significant.
Footnotes
Contributors: NS: planning, conduct, reporting, conception and design, and acquisition of data.
KH: conduct, reporting and acquisition of data.
KY: conduct, reporting and acquisition of data.
TK: conduct, reporting and acquisition of data.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Rojas P, Amat-Santos IJ, Cortés C, et al. Acquired aseptic intracardiac shunts following transcatheter aortic valve replacement: a systematic review. JACC Cardiovasc Interv 2016;9:2527–38. 10.1016/j.jcin.2016.09.034 [DOI] [PubMed] [Google Scholar]
- 2. Shakoor MT, Islam AM, Ayub S. Acquired aorto-right ventricular fistula following transcatheter aortic valve replacement. Case Rep Cardiol 2015;2015:1–3. 10.1155/2015/608539 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Pilgrim T, Meier B, Wenaweser P. Aorto-right ventricular fistula after transfemoral aortic valve implantation. J Invasive Cardiol 2010;22:E30–1. [PubMed] [Google Scholar]
- 4. Leroux L, Dijos M, Peltan J, et al. Lethal aorto-right ventricular defect after transcatheter aortic valve implantation in a patient with Radiation-Induced porcelain aorta: notes of caution. Can J Cardiol 2016;32:135.e9–135.e11. 10.1016/j.cjca.2015.05.021 [DOI] [PubMed] [Google Scholar]
- 5. Leu HB, Chang HH, Wu MH, et al. Four-year follow-up of acquired aorto-right ventricular fistula after transcatheter aortic valve implantation. Eur Heart J 2016;37:2679 10.1093/eurheartj/ehv716 [DOI] [PubMed] [Google Scholar]
- 6. Muñoz-García AJ, Rodríguez-Bailón I, Briales JH, et al. Aorto-right ventricular fistula after percutaneous aortic valve implantation of a CoreValve prosthesis. Tex Heart Inst J 2011;38:728–9. [PMC free article] [PubMed] [Google Scholar]
- 7. Nakamura K, Passeri JJ, Inglessis-Azuaje I. Percutaneous closure of acute aorto-right ventricular fistula following transcatheter bicuspid aortic valve replacement. Catheterization and Cardiovascular Interventions 2016;98 Epub ahead of print 10.1002/ccd.26705 [DOI] [PubMed] [Google Scholar]