

Description
A woman in her 60s with a history of cutaneous melanoma status post wide local excision and negative sentinel lymph node biopsy more than one decade before presented with 3 weeks of worsening memory, word finding difficulty and changes in handwriting. Her family reported peculiar behaviour such as writing letters on top of (instead of next to) one another and using a hairbrush upside down. The patient also complained of new right leg pain, paraesthesias and a mild frontal headache. Dermatological exam was notable for a 2×2 cm smooth, round nodule on the right parietal scalp, which had been present for a few months and was notable for complete loss of the overlying hair (figure 1). MRI of the brain showed greater than 10 diffusely enhancing lesions suspicious for metastatic disease, with a dominant left parietal haemorrhagic lesion measuring approximately 2.8×2.9×2.2 cm (figure 2). Associated vasogenic oedema resulted in an 8 mm midline shift. Punch biopsy of the scalp nodule revealed malignant melanoma in the dermis staining positive for Melan-A and S100. A BRAF codon V600K missense mutation was detected. Left parietal craniotomy was performed for mass resection, and the patient subsequently received chemotherapy, Gamma Knife radiation, and targeted therapy with the BRAF inhibitor dabrafenib and the MEK inhibitor trametinib. Unfortunately, the patient did not respond to treatment and passed away from complications of metastatic melanoma.
Figure 1.
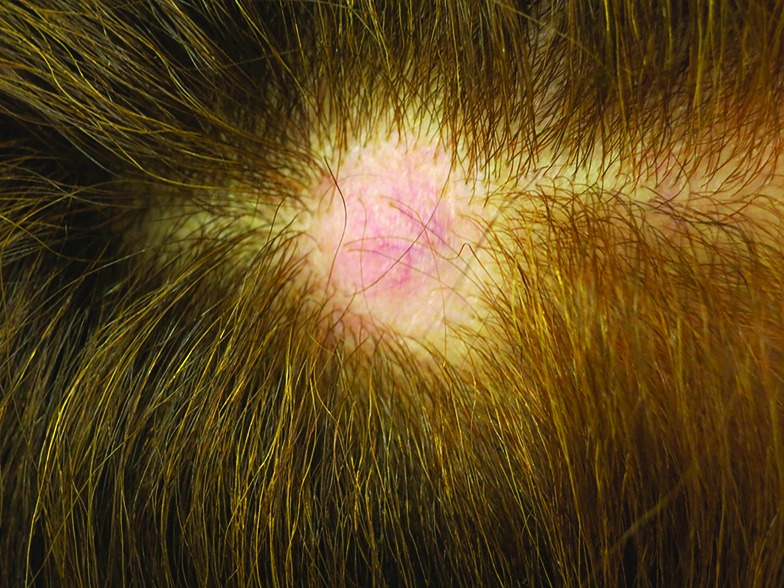
A smooth, alopecic nodule on the right parietal scalp diagnosed as alopecia neoplastica.
Figure 2.
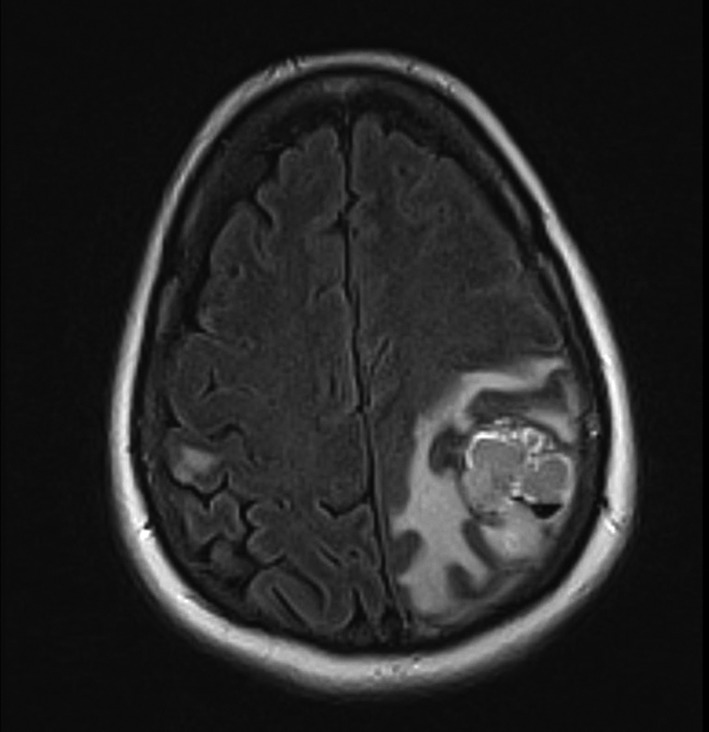
MRI of the brain showing numerous foci of metastatic melanoma, including a large haemorrhagic left parietal lobe lesion (axial view, T2 FLAIR).
Learning points.
Malignant melanoma is a skin cancer with a high potential for metastasis; metastatic disease can present more than 10 years after initial diagnosis, despite apparently successful resection.
Alopecia neoplastica is a rare form of cutaneous metastasis in which underlying cancer spreads to the scalp, replacing normal adnexal structures and hair follicles1 2; it must be differentiated from common and benign conditions such as alopecia areata.
A careful dermatological exam is essential in any patient with a history of malignancy; recognition of cutaneous metastatic disease can enable more timely diagnosis and treatment.
Footnotes
Contributors: Both authors had full access to the data contained in this manuscript. PC was the primary author of the manuscript, and RGM made substantive additions and changes to it.
Competing interests: None declared.
Patient consent: Obtained from next of kin.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Erstine EM, Elwood HR, Westbrook KC, et al. . Desmoplastic melanoma presenting as primary alopecia neoplastica: a report of two cases. J Cutan Pathol 2016;43:872–9.doi:10.1111/cup.12758 [DOI] [PubMed] [Google Scholar]
- 2.Mallon E, Dawber RP. Alopecia neoplastica without Alopecia: a unique presentation of breast carcinoma scalp metastasis. J Am Acad Dermatol 1994;31(2 Pt 2):319–21.doi:10.1016/S0190-9622(94)70163-6 [DOI] [PubMed] [Google Scholar]