

Description
A 12-year-old, previously healthy, girl presented to our hospital with a 3-day history of epigastric pain and vomiting. She also reported having frequent epigastric pain for the past 2 years. Physical examination revealed a body mass index of 13.5 kg/m2 and abdominal distension. Abdominal contrast-enhanced CT revealed a bloated stomach and a sandwiched horizontal portion of the duodenum between the aorta and superior mesenteric artery (SMA). The angle between the aorta and SMA was 17°, and the aorta–SMA distance was 5.2 mm (figure 1A,B), which met the diagnostic imaging adult criteria for SMA syndrome (SMAS).1 An upper gastrointestinal series also revealed that the contrast agent smoothly reached the proximal duodenum, but stopped at the horizontal portion of the duodenum where stenosis was suspected based on CT (figure 1C). Decompression using a nasogastric tube improved her clinical symptoms, and she was discharged. SMAS is characterised by obstruction of the horizontal portion of the duodenum from the compression of the SMA and aorta. Most adult patients have predisposing factors for SMAS, including wasting disease, severe injuries, dietary disorders and postoperative states.2 In contrast, SMAS may occur in healthy children and is accompanied by growth spurts during puberty.3 The patient’s weight increase, which could not catch up to the height increase, was thought to be the cause in this case (figure 2). Therefore, SMAS should be included as a differential diagnosis in adolescent patients with chronic abdominal pain.
Figure 1.

(A) CT axial section shows a sandwiched horizontal portion of the duodenum between the superior mesenteric artery (SMA) and abdominal aorta (arrow), which was was proximal to the duodenal and gastric dilation. The distance between the aorta and SMA is 5.2 mm. (B) CT sagittal section shows a 17° angle between the aorta and the SMA. (C) An upper gastrointestinal series shows an abrupt cut-off (arrow) at the horizontal portion of the duodenum.
Figure 2.
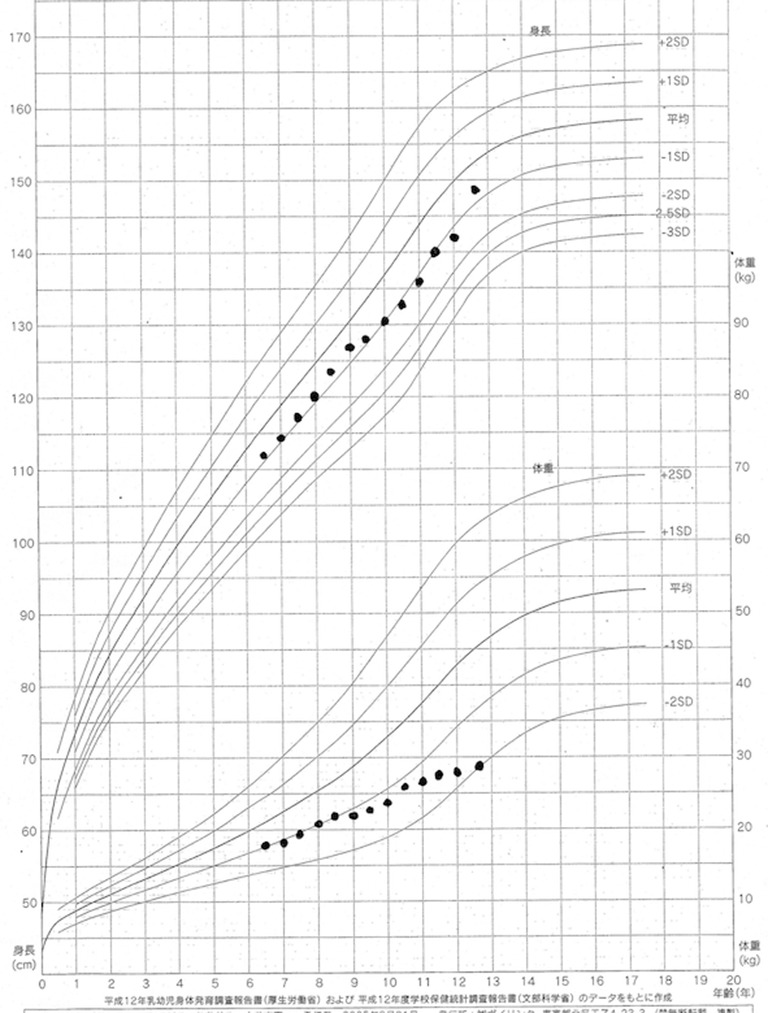
This growth chart demonstrates that the growth in weight was poor, compared with the growth in height.
Learning points.
Superior mesenteric artery syndrome may occur in healthy children and is accompanied by growth spurts during puberty.
Superior mesenteric artery syndrome should be included as a differential diagnosis in adolescent patients with chronic abdominal pain.
Footnotes
Contributors: KK diagnosed the patient and wrote this article. YK provided specific advice.
Competing interests: None declared.
Patient consent: Consent obtained from guardian.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Unal B, Aktaş A, Kemal G, et al. Superior mesenteric artery syndrome: CT and ultrasonography findings. Diagn Interv Radiol 2005;11:90–5. [PubMed] [Google Scholar]
- 2. Panda N, Das R, Gumta M, et al. Wilkie's syndrome: review of eight cases. Acta Gastroenterol Latinoam 2013;43:240–7. [PubMed] [Google Scholar]
- 3. Shin MS, Kim JY. Optimal duration of medical treatment in superior mesenteric artery syndrome in children. J Korean Med Sci 2013;28:1220–5.doi:10.3346/jkms.2013.28.8.1220 [DOI] [PMC free article] [PubMed] [Google Scholar]