

Abstract
Pyogenic granuloma is a common benign vascular tumour occurring in all ages. Both skin and mucous membranes can be affected. Of pathogenetic importance are trauma, BRAF mutations and probably herpes virus type 1, Orf virus and/or human papilloma virus type 2. The tumour consists of capillary proliferations, venules and fibromyxoid stroma. The development of a lesion occurs in three stages and bleeding is a common symptom. The tumour can mimic various other vascular lesions, solid tumours, and soft tissue infections. In recent years, targeted tumour therapies have become the most common cause of drug-induced pyogenic granulomas. The backbone of treatment is surgical procedures including laser therapy. New developments in medical drug therapy include topical and systemic beta-adrenergic receptor antagonists timolol and propranolol. Drug therapy is an alternative for young children, ocular and periungual pyogenic granuloma.
Keywords: Pyogenic granuloma, benign vascular tumours, BRAF mutations, virus, surgery, beta-adrenergic receptor antagonists
Introduction
Pyogenic granuloma (PG) – also known as lobular capillary hemangioma - is a benign vascular tumour that occurs on the skin and mucous membranes, occasional it can be found subcutaneously or intravascularly. PG can arise spontaneously, in sites of injury, or within capillary malformations [1].
PG has been associated with certain medications such as oral contraceptives, retinoids, gefitinib, cabecitabine, and afatinib [2-5]. Most tumours occur as solitary lesions, but multiple grouped or disseminated tumours have been described. Multiple disseminated tumours are an adverse cutaneous effect of melanoma treatment with selective BRAF inhibitors like vemurafenib or encorafenib [6]. Multiple periungual PGs occur with targeted oncological therapies using epidermal growth-factor receptor inhibitors or mitogen-activated protein kinase (MEK) inhibitors [7], and rituximab [8].
Histology and Pathogenesis
Histologically, PG is composed of capillaries and venules with plump endothelial cells separated into lobules by fibromyxoid stroma. The development can be classified into (i) cellular phase, (ii) capillary phase or vascular phase, and (iii) involutionary phase. Slow fibromatous regression is seen in untreated lesions after longer time [9]. The endothelial cells in PG express CD34, ICAM-1, VCAM-1 associated with an increased microvascular density [10].
Recently, BRAF c.1799T>A mutation had been identified in endothelial cells as a major driver mutation in the pathogenesis of PG [11]. This explains the occurrence of multiple PGs in patients treated with BRAF inhibitors.
The participation of viral particles in PG pathogenesis has been discussed. Alpha-herpes viridiae type 1 is considered as a possible indirect factor stimulating angiogenesis in PG. In some patients, dermatotropic parapoxvirus (Orf) could be identified by polymerase-chain reaction (PCR). Human papilloma virus DNA could be identified in 44% of these lesions with HPV type 2 as the most common [12-15].
Clinical Presentation
PG occurs in all age groups. There is no clear predominance of a gender. PG appear as small or large, smooth or lobulated, reddish exophytic vascular nodules that can grow rapidly (Fig. 1). Larger lesions become lobulated and sometimes develop into mushroom-like, pediculated tumours (Fig. 2). PGs have a tendency to bleed profusely. Bleeding is the leading symptom for a visit to the doctor’s office.
Figure 1.
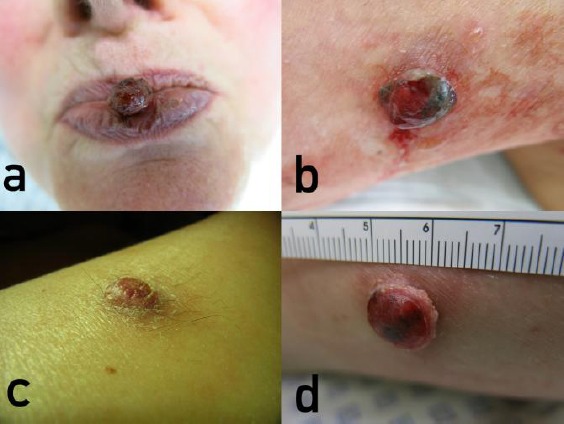
Pyogenic granuloma (PG) – common clinical presentations. (a) Nodular PG of the lower lip; (b) Collerette- like demarcation of a PG on the knee; (c) Flat, keratotic PG on the lower leg. (d) Marked collerette with a flat nodule on the lower arm
Figure 2.

Pyogenic granuloma (PG) – less common clinical findings. (a) Larger mushroom-like, thrombosed PG – melanoma-like; (b) Mushroom-like PG on the finger bow with a wet surface and maceration of the surrounding skin – pyoderma-like; (c) Large pedunculated PG of the upper lip – hemangioma like; (d) Large, firm nodular PG of the palm – non-melanoma skin cancer-like
Hands, lower lips and gingiva are most frequently affected [1]. In one study, PG was the most common benign lesion of the lips responsible for 48% of all cases [16]. Another study from Brazil investigated gingival lesions in children and adolescents. PGs accounted for 42% of all gingival lesions [17]. Considering the nail organ, most lesions occur on the nail folds, but subungual tumours have also been observed [18].
During pregnancy, large intraoral PGs may develop [19]. Uncommon sites are vulva and penis, oesophagus, gut, and tracheobronchial tree [20-24]. Gastrointestinal PG can cause severe anaemia [25]. Extremely rare are intravascular tumours which bear the risk of thrombosis [26].
Portwine stains are at risk for secondary PG [27]. Their treatment with vascular lasers may induce PG as well [28].
Satellitosis is a very uncommon phenomenon in benign tumours. Nevertheless, satellitosis has been observed in paediatric PG [29, 30]. Deep-seated PG is a rare entity with 3.8% of all PGs diagnosed in childhood [31].
Differential diagnoses
PG can mimic other vascular tumours, including Kaposi form hemangioendothelioma, infantile hemangiomas, vascular malformations, and Kaposi sarcoma. In so-called “Kaposi-like PG” human herpes virus type 8 could be identified. These lesions are true Kaposi sarcomas, not PG [32]. Other malignancies that can mimic PC are malignant lymphomas, basal cell carcinoma, or malignant melanoma [33-35]. In immunocompromised patients, deep soft tissue infections like phaeohyphomycosis or bartonellosis should be considered [36, 37].
Treatment
The usual treatment for PG consists of excision, the treatment with the lowest rate of recurrence [1]. Depending on the area, size and patient wishes, curettage, electrocautery, radiosurgery, cryosurgery, sclerotherapy, or laser treatment are alternative options. Among lasers, diode lasers of wave-length between 808 to 980 nm [38-40] or solid-state neodymium - yttrium aluminium garnet (Nd:YAG) lasers [41, 42], erbium-YAG and CO2 lasers [43, 44] have all been used successfully. Erbium-YAG laser lacks coagulation, what may become a disadvantage in larger lesions. Successful photodynamic therapy (PDT) with 5-aminolevulinic acid has been reported for a single PG on a finger [45]. A possible advantage of PDT compared to laser removal has yet not proved.
In small children, topical or oral medical therapy with beta-adrenergic receptor antagonists timolol or propranolol seems to be effective [46]. Periungual PGs have been treated off-label with topical 1% propranolol cream [47]. For PG on ocular surfaces medical treatment with topical 0.5 % timolol eye drops twice daily for a minimum of 21 days, is an option [48]. The treatment, either oral or topical, warrants monitoring. Since systemic absorption can occur even after timolol eye drops, patients should be monitored for bradycardia, hypotension, hypoglycemia, and bronchoconstriction. In elderly patients, syncope and falls have been observed [49, 50].
Footnotes
Funding: This research did not receive any financial support.
Competing Interests: The authors have declared that no competing interests exist.
References
- 1.Giblin AV, Clover AJ, Athanassopoulos A, Budny PG. Pyogenic granuloma - the quest for optimum treatment:an audit of treatment of 408 cases. J Plast Reconstr Aesthet Surg. 2007;60(9):1030–5. doi: 10.1016/j.bjps.2006.10.018. https://doi.org/10.1016/j.bjps.2006.10.018 PMid:17478135. [DOI] [PubMed] [Google Scholar]
- 2.Simmons BJ, Chen L, Hu S. Pyogenic granuloma association with isotretinoin treatment for acne. Australas J Dermatol. 2016;57(4):e144–5. doi: 10.1111/ajd.12418. https://doi.org/10.1111/ajd.12418 PMid:27885661. [DOI] [PubMed] [Google Scholar]
- 3.Massa A, Antunes A, Varela P. Pyogenic granuloma in a patient on gefitinib. Acta Med Port. 2016;29(6):416. doi: 10.20344/amp.6343. https://doi.org/10.20344/amp.6343 PMid:27⇌23. [DOI] [PubMed] [Google Scholar]
- 4.Fujiwara C, Motegi SI, Sekiguchi A, Amano H, Ishikawa O. Pyogenic granuloma possibly associated with capecitabine therapy. J Dermatol. 2016 doi: 10.1111/1346-8138.13691. https://doi.org/10.1111/1346-8138.13691. [DOI] [PubMed] [Google Scholar]
- 5.Inoue A, Sawada Y, Nishio D, Nakamura M. Pyogenic granuloma caused by afatinib:Case report and review of the literature. Australas J Dermatol. 2017;58(1):61–2. doi: 10.1111/ajd.12423. https://doi.org/10.1111/ajd.12423 PMid:26603180. [DOI] [PubMed] [Google Scholar]
- 6.Henning B, Stieger P, Kamarachev J, Dummer R, Goldinger SM. Pyogenic granuloma in patients treated with selective BRAF inhibitors:another manifestation of paradoxical pathway activation. Melanoma Res. 2016;26(3):304–7. doi: 10.1097/CMR.0000000000000248. https://doi.org/10.1097/CMR.0000000000000248 PMid:27116335. [DOI] [PubMed] [Google Scholar]
- 7.Robert C, Sibaud V, Mateus C, Verschoore M, Charles C, Lanoy E, Baran R. Nail toxicities induced by systemic anticancer treatments. Lancet Oncol. 2015;16(4):e181–9. doi: 10.1016/S1470-2045(14)71133-7. https://doi.org/10.1016/S1470-2045(14)71133-7. [DOI] [PubMed] [Google Scholar]
- 8.Wollina U. Multiple eruptive periungual pyogenic granulomas during anti-CD20 monoclonal antibody therapy for rheumatoid arthritis. J Dermatol Case Rep. 2010;4(3):44–6. doi: 10.3315/jdcr.2010.1050. https://doi.org/10.3315/jdcr.2010.1050 PMid:21886749 PMCid:PMC3157817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Marla V, Shrestha A, Goel K, Shrestha S. The histopathological spectrum of pyogenic granuloma:A case series. Case Rep Dent. 2016;2016:1323798. doi: 10.1155/2016/1323798. https://doi.org/10.1155/2016/1323798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Seyedmajidi M, Shafaee S, Hashemipour G, Bijani A, Ehsani H. Immunohistochemical evaluation of angiogenesis related markers in pyogenic granuloma of gingiva. Asian Pac J Cancer Prev. 2015;16(17):7513–6. doi: 10.7314/apjcp.2015.16.17.7513. https://doi.org/10.7314/APJCP.2015.16.17.7513 PMid:26625754. [DOI] [PubMed] [Google Scholar]
- 11.Groesser L, Peterhof E, Evert M, Landthaler M, Berneburg M, Hafner C. BRAF and RAS mutations in sporadic and secondary pyogenic granuloma. J Invest Dermatol. 2016;136(2):481–6. doi: 10.1038/JID.2015.376. https://doi.org/10.1038/JID.2015.376. [DOI] [PubMed] [Google Scholar]
- 12.El Hayderi L, Rübben A, Nikkels AF. [The alpha-herpesviridae in dermatology:Herpes simplex virus types I and II. German version]. Hautarzt. 2017;68(3):181–6. doi: 10.1007/s00105-016-3929-5. https://doi.org/10.1007/s00105-016-3929-5 PMid:28197699. [DOI] [PubMed] [Google Scholar]
- 13.Biyik Ozkaya D, Taskın B, Tas B, Asıran Serdar Z, Demirkesen C, Su O, Onsun N. Poxvirus-induced angiogenesis after a thermal burn. J Dermatol. 2014;41(9):830–3. doi: 10.1111/1346-8138.12589. https://doi.org/10.1111/1346-8138.12589 PMid:25110123. [DOI] [PubMed] [Google Scholar]
- 14.Ran M, Lee M, Gong J, Lin Z, Li R. Oral acyclovir and intralesional interferon injections for treatment of giant pyogenic granuloma-like lesions in an immunocompromised patient with human Orf. JAMA Dermatol. 2015;151(9):1032–4. doi: 10.1001/jamadermatol.2015.0760. https://doi.org/10.1001/jamadermatol.2015.0760 PMid:25946461. [DOI] [PubMed] [Google Scholar]
- 15.Vázquez-Martínez OT, González-Betancourt A, Barboza-Cerda MC, González-González SE, Lugo-Trampe Á, Welsh O, Rojas-Martínez A, Martínez-Rodríguez HG, Ocampo-Candiani J, Ortiz-López R. Human papillomavirus type 2 associated with pyogenic granuloma in patients without clinical evidence of warts. Int J Dermatol. 2015;55(7):745–50. doi: 10.1111/ijd.12982. https://doi.org/10.1111/ijd.12982 PMid:26492599. [DOI] [PubMed] [Google Scholar]
- 16.Tobouti PL, Olegário I, de Sousa SC. Benign vascular lesions of the lips:Diagnostic approach. J Cutan Pathol. 2017;44(5):451–5. doi: 10.1111/cup.12911. https://doi.org/10.1111/cup.12911 PMid:28111788. [DOI] [PubMed] [Google Scholar]
- 17.daSilva FC, Piazzetta CM, Torres-Pereira CC, Schussel JL, Amenábar JM. Gingival proliferative lesions in children and adolescents in Brazil:A 15-year-period cross-sectional study. J Indian Soc Periodontol. 2016;20(1):63–6. doi: 10.4103/0972-124X.168493. https://doi.org/10.4103/0972-124X.168493 PMid:27041840 PMCid:PMC4795138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wollina U. Subungual telangiectatic granuloma. Dtsch Arztebl Int. 2017;114(8):136. doi: 10.3238/arztebl.2017.0136. PMid:28302264 PMCid:PMC5374259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Silva de Araujo Figueiredo C, Gonçalves Carvalho Rosalem C, Costa Cantanhede AL, Abreu Fonseca Thomaz ÉB, Fontoura Nogueira da Cruz MC. Systemic alterations and their oral manifestations in pregnant women. J Obstet Gynaecol Res. 2017;43(1):16–22. doi: 10.1111/jog.13150. https://doi.org/10.1111/jog.13150 PMid:28074549. [DOI] [PubMed] [Google Scholar]
- 20.Abreu-Dos-Santos F, Câmara S, Reis F, Freitas T, Gaspar H, Cordeiro M. Vulvar lobular capillary hemangioma:A rare location for a frequent entity. Case Rep Obstet Gynecol. 2016;2016:3435270. doi: 10.1155/2016/3435270. https://doi.org/10.1155/2016/3435270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Katmeh RF, Johnson L, Kempley E, Kotecha S, Hamarneh W, Chitale S. Pyogenic granuloma of the penis:An uncommon lesion with unusual presentation. Curr Urol. 2017;9(4):216–8. doi: 10.1159/000447144. https://doi.org/10.1159/000447144 PMid:28413384 PMCid:PMC5385862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zhao J, Feng Q, Shi S. Pyogenic granuloma of the esophagus. Clin Gastroenterol Hepatol. 2017 doi: 10.1016/j.cgh.2017.03.028. https://doi.org/10.1016/j.cgh.2017.03.028. [DOI] [PubMed] [Google Scholar]
- 23.Romero Mascarell C, García Pagán JC, Araujo IK, Llach J, González-Suárez B. Pyogenic granuloma in the jejunum successfully removed by single-balloon enteroscopy. Rev Esp Enferm Dig. 2017;109(2):152–4. doi: 10.17235/reed.2017.4153/2015. PMid:28196424. [DOI] [PubMed] [Google Scholar]
- 24.Qiu X, Dong Z, Zhang J, Yu J. Lobular capillary hemangioma of the tracheobronchial tree:A case report and literature review. Medicine (Baltimore) 2016;95(48):e5499. doi: 10.1097/MD.0000000000005499. https://doi.org/10.1097/MD.0000000000005499 PMid:27902613 PMCid:PMC5134768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Misawa S, Sakamoto H, Kurogochi A, Kirii Y, Nakamura S, Misawa T, Yoneda S, Hirano M, Owa O, Takagi H, Ota H. Rare cause of severe anemia due to pyogenic granuloma in the jejunum. BMC Gastroenterol. 2015;15:126. doi: 10.1186/s12876-015-0355-6. https://doi.org/10.1186/s12876-015-0355-6 PMid:26444414 PMCid:PMC4596517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Matsuzaki K, Imamura Y, Ozawa M, Nakajima T, Ikeda A, Konishi T, Jikuya T. Intravenous lobular capillary hemangioma in the subclavian vein. Ann Thorac Surg. 2016;102(5):e427–9. doi: 10.1016/j.athoracsur.2016.04.013. https://doi.org/10.1016/j.athoracsur.2016.04.013 PMid:27772599. [DOI] [PubMed] [Google Scholar]
- 27.Brightman LA, Geronemus RG, Reddy KK. Laser treatment of port-wine stains. Clin Cosmet Investig Dermatol. 2015;8:27–33. doi: 10.2147/CCID.S53118. PMid:25624768 PMCid:PMC4296879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wollina U, Zielinski M, Knopf B, Hipler C. [Eruptive capillary hemangioma following argon laser therapy of naevus flammeus] Hautarzt. 1989;40(4):212–4. PMid:2732049. [PubMed] [Google Scholar]
- 29.Rana R, Ramachandra SS, Prasad UC, Aggarwal P, Dayakara JK. Recurrent pyogenic granuloma with a satellite lesion. Cutis. 2015;96(2):E27–30. PMid:26367761. [PubMed] [Google Scholar]
- 30.Gupta V, Mridha AR, Sharma VK. Pediatric Dermatology Photoquiz:Multiple erythematous papules on the back. Recurrent pyogenic granulomas with satellitosis. Pediatr Dermatol. 2016;33(1):97–8. doi: 10.1111/pde.12700. https://doi.org/10.1111/pde.12700 PMid:26758098. [DOI] [PubMed] [Google Scholar]
- 31.Putra J, Rymeski B, Merrow AC, Dasgupta R, Gupta A. Four cases of pediatric deep-seated/subcutaneous pyogenic granuloma:Review of literature and differential diagnosis. J Cutan Pathol. 2017 doi: 10.1111/cup.12923. https://doi.org/10.1111/cup.12923 PMid:28233342. [DOI] [PubMed] [Google Scholar]
- 32.Ryan P, Aarons S, Murray D, Markham T, O’Sullivan S, Lyons F, Lee G, Fitzgibbon J. Human herpesvirus 8 (HHV-8) detected in two patients with Kaposi’s sarcoma-like pyogenic granuloma. J Clin Pathol. 2002;55(8):619–22. doi: 10.1136/jcp.55.8.619. https://doi.org/10.1136/jcp.55.8.619 PMid:12147659 PMCid:PMC1769721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bains A, Vedant D, Shanker V, Tegta GR. Primary cutaneous anaplastic large cell lymphoma masquerading as large pyogenic granuloma. Indian Dermatol Online J. 2016;7(6):526–8. doi: 10.4103/2229-5178.193896. https://doi.org/10.4103/2229-5178.193896 PMid:27990392 PMCid:PMC5134171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kumar P, Das A, Mondal A, Savant SS. Pyogenic granuloma-like basal cell carcinoma on the abdomen:A deceptive presentation. Indian Dermatol Online J. 2016;7(5):446–448. doi: 10.4103/2229-5178.190502. https://doi.org/10.4103/2229-5178.190502 PMid:27730056 PMCid:PMC5038121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Jafarian F, Powell J, Kokta V, Champagne M, Hatami A, McCuaig C, Marcoux D, Savard P. Malignant melanoma in childhood and adolescence:report of 13 cases. J Am Acad Dermatol. 2005;53(5):816–22. doi: 10.1016/j.jaad.2005.07.013. https://doi.org/10.1016/j.jaad.2005.07.013 PMid:16243130. [DOI] [PubMed] [Google Scholar]
- 36.Khader A, Ambooken B, Binitha MP, Francis S, Kuttiyil AK, Sureshan DN. Disseminated cutaneous due to Cladophialophora bantiana. Indian J Dermatol Venereol Leprol. 2015;81(5):491–4. doi: 10.4103/0378-6323.162333. https://doi.org/10.4103/0378-6323.162333 PMid:26261143. [DOI] [PubMed] [Google Scholar]
- 37.Bolton JG, Galeckas KJ, Satter EK. Inoculation bartonellosis in an adult:a case report. Cutis. 2010;85(1):37–42. PMid:20184210. [PubMed] [Google Scholar]
- 38.Al-Mohaya MA, Al-Malik AM. Excision of oral pyogenic granuloma in a diabetic patient with 940nm diode laser. Saudi Med J. 2016;37(12):1395–1400. doi: 10.15537/smj.2016.12.15941. https://doi.org/10.15537/smj.2016.12.15941 PMid:27874157 PMCid:PMC5303780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Hasanoglu Erbasar GN, Senguven B, Gultekin SE, Cetiner S. Management of a recurrent pyogenic granuloma of the hard palate with diode laser:A case report. J Lasers Med Sci. 2016;7(1):56–61. doi: 10.15171/jlms.2016.12. https://doi.org/10.15171/jlms.2016.12 PMid:27330700 PMCid:PMC4908978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Wollina U. Three hundred patients treated with ultrapulsed 980 nm diode laser for skin disorders. Indian J Dermatol. 2016;61(5):540–4. doi: 10.4103/0019-5154.190111. https://doi.org/10.4103/0019-5154.190111 PMid:27688445 PMCid:PMC5029241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Au S, Fancher W, Scribner J. Treatment of pediatric pyogenic granuloma in a functionally and cosmetically sensitive area with the 1064nm Nd:Yag laser. Dermatol Online J. 2016;22(4) PMid:27617472. [PubMed] [Google Scholar]
- 42.Goldman A, Rossata F, Wollina U. Versatility of the Nd-YAG laser in the treatment of facial vascular alterations. Kosmet Med. 2008;29:134–7. [Google Scholar]
- 43.Fekrazad R, Nokhbatolfoghahaei H, Khoei F, Kalhori KA. Pyogenic granuloma:surgical treatment with Er:YAG laser. J Lasers Med Sci. 2014;5(4):199–205. PMid:25653822 PMCid:PMC4281984. [PMC free article] [PubMed] [Google Scholar]
- 44.Truschnegg A, Acham S, Kqiku L, Beham A, Jakse N. CO2 laser excision of a pyogenic granuloma associated with dental implants:A case report and review of the literature. Photomed Laser Surg. 2016;34(9):425–31. doi: 10.1089/pho.2016.4089. PMid:27420917. [DOI] [PubMed] [Google Scholar]
- 45.Liu J, Zhou BR, Yi F, Wu HJ, Zhang JA, Luo D. Pyogenic granuloma in a patient with psoriasis successfully treated by 5-aminolevulinic acid photodynamic therapy:A case report. Exp Ther Med. 2016;11(1):345–347. doi: 10.3892/etm.2015.2899. PMid:26889266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Wine Lee L, Goff KL, Lam JM, Low DW, Yan AC, Castelo-Soccio L. Treatment of pediatric pyogenic granulomas using β-adrenergic receptor antagonists. Pediatr Dermatol. 2014;31(2):203–7. doi: 10.1111/pde.12217. https://doi.org/10.1111/pde.12217 PMid:24138457. [DOI] [PubMed] [Google Scholar]
- 47.Piraccini BM, Alessandrini A, Dika E, Starace M, Patrizi A, Neri I. Topical propranolol 1% cream for pyogenic granulomas of the nail:open-label study in 10 patients. J Eur Acad Dermatol Venereol. 2016;30(5):901–2. doi: 10.1111/jdv.13071. https://doi.org/10.1111/jdv.13071 PMid:25708373. [DOI] [PubMed] [Google Scholar]
- 48.Oke I, Alkharashi M, Petersen RA, Ashenberg A, Shah AS. Treatment of ocular pyogenic granuloma with topical timolol. JAMA Ophthalmol. 2017;135(4):383–5. doi: 10.1001/jamaophthalmol.2017.0110. https://doi.org/10.1001/jamaophthalmol.2017.0110 PMid:28301661. [DOI] [PubMed] [Google Scholar]
- 49.de Graaf M, Breur JM, Raphaël MF, Vos M, Breugem CC, Pasmans SG. Adverse effects of propranolol when used in the treatment of hemangiomas:a case series of 28 infants. J Am Acad Dermatol. 2011;65(2):320–7. doi: 10.1016/j.jaad.2010.06.048. https://doi.org/10.1016/j.jaad.2010.06.048 PMid:21601311. [DOI] [PubMed] [Google Scholar]
- 50.Müller ME, van der Velde N, Krulder JW, van der Cammen TJ. Syncope and falls due to timolol eye drops. BMJ. 2006;332(7547):960–1. doi: 10.1136/bmj.332.7547.960. https://doi.org/10.1136/bmj.332.7547.960 PMid:16627515 PMCid:PMC1444852. [DOI] [PMC free article] [PubMed] [Google Scholar]