

Abstract
Objectives
To examine the impact of enrolling in a health care plan through the Affordable Care Act (ACA) health care exchanges on self-reported access to care.
Study Design
Cohort study using self-reported data of patients newly enrolled in Kaiser Permanente California and Kaiser Permanente Colorado through the ACA health care exchanges for coverage beginning January 1, 2014.
Methods
Baseline and follow-up surveys conducted via mail and telephone, with response rates of 45% and 51% respectively.
Results
We found significant increases in the percentage of people who reported having a personal health care provider (59% vs. 73%, p<.01), and significant decreases in the percentage of people who reported delaying needed medical care due to costs (37% vs. 25%, p<.01) before and after ACA enrollment. There was a significant increase in the percentage of patients who reported receiving a flu shot during the prior year (41% vs. 52%, p<.01). Among the people who reported having less than 4 months of health care coverage in 2013, these improvements were even more pronounced; this group also showed significant increases in the percentage who felt they had a place to go when they needed medical care (43% vs. 56%, p<.01), and the percentage reporting they received advice to quit smoking or using tobacco (46% vs. 72%, p<.05).
Conclusions
These findings are an important addition to the evidence base that the ACA is improving the health care experience, and reducing barriers due to costs, in people obtaining insurance coverage through the health care exchanges.
Keywords: Affordable Care Act, access, costs of care
Introduction
A major goal of the Affordable Care Act (ACA) is to increase access to health care, particularly for people who are uninsured, under-insured, or without stable health care insurance.1 The ACA has reduced the size of the uninsured population, and in 2016 close to 13 million Americans enrolled in a health plan through the federal or state-operated health care exchanges.2 However, there has been significant debate as to whether the ACA has achieved its goals of improving access while decreasing costs.3 Most empirical studies since implementation of the ACA’s health care exchanges in 2014 have focused on the number of uninsured Americans within the US and by state,4–6 or examined care trends at the population level.6 The impact of insurance obtained through health care exchanges on access and costs of care and at the individual level is largely unknown. The purpose of our study was to measure changes in self-reported health care access and cost-related barriers to health care in patients obtaining insurance through the ACA’s health care exchanges.
Methods
We surveyed 2,145 adults age 18–64 who obtained insurance coverage through Kaiser Permanente (KP) by enrolling via the California or Colorado state health care exchanges starting January 1, 2014. The survey was restricted to individuals who had not had KP health care coverage in the five years prior to initial exchange enrollment. Survey questions asked about health care experiences in the prior year, and asked individuals about their perceptions of whether they had a usual source of care and a regular health care provider, or had delayed health care due to cost. Questions also assessed patient self-reported preventive behaviors and health behavior counseling. New KP members eligible for the survey were initially contacted by mail and asked to return a paper version of the survey; non-respondents were called and offered the survey by phone. Responders to the initial baseline survey were re-contacted in one year and asked the same set of questions, in order to assess if access, preventive behaviors, or cost barriers had changed since health care exchange enrollment. The response rate for the baseline survey was 45%, and the response rate for the follow-up survey was 51%. We compared differences in individual baseline survey responses regarding experiences in the year prior to ACA enrollment (2013) to follow-up survey responses regarding experiences in the year post-ACA enrollment (2014) at the individual level using chi-square tests for significance. Analyses were performed using SAS v.9.2. This study was approved by the KPNC and KPCO Institutional Review Boards.
Results
A total of 528 patients completed both baseline and follow-up surveys; these responders were 55% female and 71% non-Hispanic White, with 62% reporting a household income of < $50,000 per year (data not shown.) We found significant increases in the percentage of people who reported having a personal health care provider (59% vs. 73%, p<.01), and significant decreases in the percentage of people who reported delaying needed medical care due to costs (37% vs. 25%, p<.01) before and after ACA enrollment. There was a significant increase in the percentage of patients who reported receiving a flu shot as well (41% vs. 52%, p<.01) (see Figure 1). Among the people who reported having less than 4 months of health care coverage in 2013, these improvements were even more pronounced (Figure 2). In addition, health care exchange enrollment was associated with significant increases in the percentage who felt they had a place to go when they needed medical care (43% vs. 56%, p<.01), and the percentage reporting they received advice to quit smoking or using tobacco (46% vs. 72%, p<.05) (Figure 2).
Figure 1.
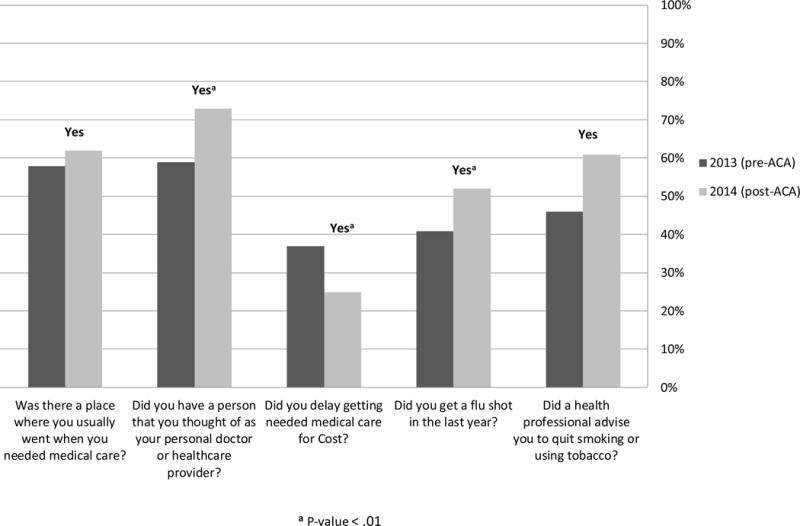
Changes in Access Pre- and Post-ACA Enrollment
Figure 2.
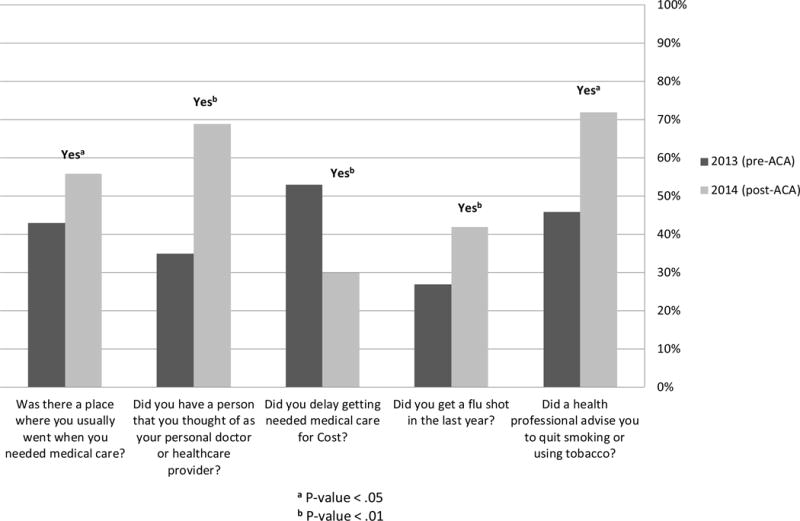
Changes in Access Pre- and Post-ACA Enrollment: Patients With Fewer Than 4 Months of Insurance in 2013
Discussion
We found that adults obtaining insurance through the health care exchanges reported increased access to care, increased use of preventive care, and fewer barriers to medical care due to cost, after ACA enrollment. These positive changes were even greater amongst patients with less than 4 months of health care coverage during the year prior to enrollment through a health care exchange. One prior study found improved trends in access and affordability after the ACA’s enactment by examining population-level trends;6 our analysis adds significant strength to the argument that the ACA has had a positive impact on care access, receipt of preventive services, and costs by examining changes in patient experiences at the individual level. While our study was conducted amongst ACA enrollees in systems whose cost-sharing structures might not represent all exchange plans, our finding that delays in receiving needed medical care were reduced after enrolling through the ACA exchanges is particularly important in light of the fact that many exchange insurance products offered are high-deductible health plans7 that involve significant cost-sharing for patients until the deductible is met.
A major aim of the ACA was to help American health care achieve the “Triple Aim” of simultaneously optimize health care access and quality while reducing costs.3,8 These findings are an important addition to the evidence base that the ACA may be improving the health care experience, reducing barriers due to costs, and contributing to a greater sense of engagement with the health care system9 in people obtaining insurance coverage through the health care exchanges.
Take-Away Points.
Among patients newly enrolling in Kaiser Permanente California and Colorado through the ACA health care exchanges, we found:
Significant increases in the percentage of people who reported having a personal health care provider
Significant decreases in the percentage of people who reported delaying needed medical care due to costs
Significant increases in the percentage who felt they had a place to go when they needed medical care, and in receiving advice to quit smoking
These findings are an important addition to the evidence base that the ACA may be improving access to care in people obtaining insurance coverage through the health care exchanges.
Acknowledgments
Funding Source This study was funded by the Kaiser Permanente Center for Effectiveness and Safety Research, Contract no. KR021125. Dr. Schmittdiel also receives support from the Health Delivery Systems Center for Diabetes Translational Research (CDTR) [NIDDK grant 1P30-DK092924].
References
- 1.Blumenthal D, Abrams M, Nuzum R. The Affordable Care Act at 5 Years. N Engl J Med. 2015 Jun 18;372(25):2451–2458. doi: 10.1056/NEJMhpr1503614. [DOI] [PubMed] [Google Scholar]
- 2.Jost T. The 2016 Open Enrollment Tally: 12.7 Million Selected Plans, 1 Million More Than. 2015 http://healthaffairs.org/blog/2016/02/04/the-2016-open-enrollment-tally-12-7-million-selected-plans-1-million-more-than-2015/. Accessed February 11, 2016.
- 3.Berwick DM, Feeley D, Loehrer S. Change from the inside out: health care leaders taking the helm. Jama. 2015 May 5;313(17):1707–1708. doi: 10.1001/jama.2015.2830. [DOI] [PubMed] [Google Scholar]
- 4.Carman KG, Eibner C, Paddock SM. Trends In Health Insurance Enrollment, 2013–15. Health Aff (Millwood) Jun. 2015;34(6):1044–1048. doi: 10.1377/hlthaff.2015.0266. [DOI] [PubMed] [Google Scholar]
- 5.Sommers BD, Buchmueller T, Decker SL, Carey C, Kronick R. The Affordable Care Act has led to significant gains in health insurance and access to care for young adults. Health Aff (Millwood) Jan. 2013;32(1):165–174. doi: 10.1377/hlthaff.2012.0552. [DOI] [PubMed] [Google Scholar]
- 6.Sommers BD, Gunja MZ, Finegold K, Musco T. Changes in Self-reported Insurance Coverage, Access to Care, and Health Under the Affordable Care Act. Jama. 2015 Jul 28;314(4):366–374. doi: 10.1001/jama.2015.8421. [DOI] [PubMed] [Google Scholar]
- 7.Wharam JF, Ross-Degnan D, Rosenthal MB. The ACA and high-deductible insurance–strategies for sharpening a blunt instrument. N Engl J Med. 2013 Oct 17;369(16):1481–1484. doi: 10.1056/NEJMp1309490. [DOI] [PubMed] [Google Scholar]
- 8.Berwick DM, Nolan TW, Whittington J. The triple aim: care, health, and cost. Health Aff (Millwood) May-Jun. 2008;27(3):759–769. doi: 10.1377/hlthaff.27.3.759. [DOI] [PubMed] [Google Scholar]
- 9.Fisher ES, McClellan MB, Bertko J, et al. Fostering accountable health care: moving forward in medicare. Health Aff (Millwood) 2009 Mar-Apr;28(2):w219–231. doi: 10.1377/hlthaff.28.2.w219. [DOI] [PMC free article] [PubMed] [Google Scholar]