

Abstract
China’s middle-aged and older women suffer from poorer health than men. Using national baseline data from China Health and Retirement Longitudinal Study (CHARLS), a survey conducted from 2011 to 2012, this paper applies logistic models to investigate the association between female fertility history (parity, early childbearing, late childbearing) and middle-aged and late-life health. We find that parity is related to the mid-late life health of women. Women with four children or more are more likely to suffer from activities of daily living (ADL) impairment and poorer self-rated health than those with one to three children. Early childbearing is associated with ADL impairment. However, the correlation is mediated by socioeconomic status. Early childbearing is related to self-rated health in later life by an indirect-only mediation effect via educational attainment and personal income.
Keywords: fertility history, ADL impairment, self-rated health, parity, early childbearing, late childbearing
Introduction
Fertility plays an important role in the health of mid-aged and older women, but the conclusions are not consistent or even conflicting. Some studies suggest that women with high parity are more likely to experience poorer health and higher mortality risks in their later life (Kington et al., 1997; Grundy and Tomassini, 2005; Sudha et al., 2006), while others find no relationship between birth numbers and women’s later life health (Spence, 2008). Having children prematurely is detrimental to women’s later life health (Grundy and Holt, 2000; Grundy and Tomassini, 2005; Mirowsky, 2005; Spence, 2008; Grundy, 2009; Read et al., 2011), as is late childbearing (Alonzo, 2002; Albrektsen et al., 2005). However, late childbearing has been reported to have a significant positive association with healthy longevity among the oldest-old people (Zeng and Vaupel, 2004).
In China, the health of older women is a serious problem. Among the 95 million females aged 60 or above in 2010, only 39.6 percent reported having good health (PCO, 2012). To date, there are few studies of the association between fertility history and later health in China. Considering the different cultural and social backgrounds between Western countries and China, this paper uses the China Health and Retirement Longitudinal Study (CHARLS) data, collected from 2011 to 2012, to investigate correlations among ADL impairment, self-rated health in women’s mid-late life and their birth parity, ages at the first and last birth. The paper is divided into four sections. The first reviews the literature, followed by an introduction to the data and analytical method. The third section presents results, with the discussion and conclusions in the fourth section.
Literature Review
Childbearing history and later health in developed countries
The fertility history of women includes such indices as the number of pregnancies, parity, age at childbearing, abortion numbers, and birth spacing. Parity and childbearing age are two important variables in the relationship of fertility history to later life health.
Parity
Some studies have examined the association between parity and later life health and have generally found that high parity is associated with worse health. A study of American women aged over 50 found that women with six or more children had worse self-reported health than nulliparous women and women with only one or two children (Kington et al., 1997). Among African-American women, high parity (six or more children) was associated with worse self-rated health, but this association was mediated by social support (Sudha et al., 2006). With U.K. data, Grundy and colleagues (Grundy and Holt, 2000; Grundy and Tomassini, 2005) found a higher likelihood of reporting a physical limitation after age 50 among women who had at least five children. Read et al. (2011) used data from the British Household Panel Survey and found that high parity (four or more children) was associated with poorer health for both women and men. Using data from the Office for National Statistics Longitudinal Study, Grundy and Tomassini (2005) found that among people aged 51 to 60 and 61 to 70, nulliparous women and women with five or more children had significantly higher mortality risk than other women.
Some other studies, however, found no association or negative correlation between high parity and later health. With data from the National Longitudinal Survey of Mature Women (NLSMW) in the U.S., Spence (2008) found no statistically significant correlation between high parity and health. For people aged 71 to 80 with only one child, the mortality risk increased relative to those with more than one child (Grundy and Tomassini, 2005).
Age at childbearing
Some researchers have suggested that the health of middle-aged and older women was related to their early childbearing. Childbirth before 21 or 22 years old was detrimental to later health (Grundy and Holt, 2000; Mirowsky, 2005), led to poorer self-rated health (Kington et al., 1997; Alonzo, 2002; Mirowsky, 2005; Sudha et al., 2006; Henretta, 2007; Hank, 2010), and increased the risk of ADL limitations (Spence, 2008). In Norway, England and Wales, and the U.S., teenage childbirth was associated with higher mortality risks in late middle age (Grundy, 2009). Teenage childbearing may limit educational attainment (McElroy, 1996), and the subsequent disadvantage may include lower socioeconomic status, lower income and worse health (Grundy and Tomassini, 2005; Mirowsky, 2005; Henretta, 2007).
The health of middle-aged and older women was also related to late childbearing. Having a child after age 35 was detrimental to later life health (Alonzo, 2002; Albrektsen et al., 2005) and was associated with an increase in self-reported physical impairments (Mirowsky, 2002). However, Snowdon et al. (1989) proposed that becoming pregnant or bearing children after 40 may be an indicator of good health. Zeng and Vaupel (2004) also believed that older women who had been able to have children after 35 were in better health.
As can be seen above, there is a consensus on the correlation between early childbearing and later health, but inconsistencies in the relationship between late childbearing and later health.
The Chinese context
Throughout China’s history, the traditional Confucian culture has had a far-reaching impact on women’s fertility motivations and behaviors, and has generated orthodox fertility ideologies such as “more sons, more blessings”, and “early childbearing”. The mainstream value of “more sons, more blessings” was prevalent before 1980 when the one-child policy became strictly enforced, and it was quite universal for a Chinese woman to have many children and bear children prematurely (Qi, 2006). Having many children with short birth intervals and bearing children early seriously affected the physical health of women (Zhao, 2009).
Hard physical labor and improper nursing during pregnancy or even shortly after delivery resulted in poor health conditions for women (Zheng, 1997; Yao, 2000). The physical and psychological health of women were also impaired by traditional birth customs, outdated delivery mode (home parturition with the assistance of an untrained midwife), and poor medical and sanitary facilities (Huang, 1996).
Son preference may also be a factor affecting women’s health. In some areas of China with strong son preference, both the baby girl and puerperal mother would not be well cared for by their families (Yao, 2000), leaving them with high risks of illness and mortality (Zheng, 1997). Under the impact of entrenched patriarchy, patrilocality, and patrilineality, women were in an inferior social position and, as a result, tended to allocate resources or health investments to their husband and sons and neglected their own health (Duan, 2008).
Recently the fertility ideology has changed, and the fertility intention is one child or two children for the majority of couples (Jiang et al., 2016). While delivery conditions have improved greatly, older women remain subject to the above contexts during their childbearing age.
Childbearing and later health in China
In China, the literature on the relationship between fertility history and later health is relatively sparse, and the conclusions are inconsistent. Using data from the 2000 wave of the Chinese Longitudinal Healthy Longevity Survey (CLHLS), Liu (2004) found that there was no statistical correlation between the self-rated health of older people and the number of their surviving children. With the 2005 wave of the CLHLS, Chen and Lei (2009) found that although the parity and health of older people were not related, the more surviving children, the better health the parents might have in their later life. However, Geng (2013), using data from the Survey on Urban Family Life conducted in 1999, found that parents (aged 61 or above) who had more children had worse self-rated health. Based on the 2000 wave of the CLHLS, Zeng and Vaupel (2004) found that older people who had given birth after 35 or even 40 had better health, indicating a positive correlation between late childbearing and later health.
Based on this literature, we make the following hypothesis:
Hypothesis 1: High parity is associated with poorer mid-aged and later life health.
Hypothesis 2: Early childbearing is detrimental to mid-late life health. But the association is mediated by educational attainment and personal income. The mediation pathways are shown in Figure 1.
Hypothesis 3: Late childbearing is related to poorer mid-aged and later health.
Figure 1.
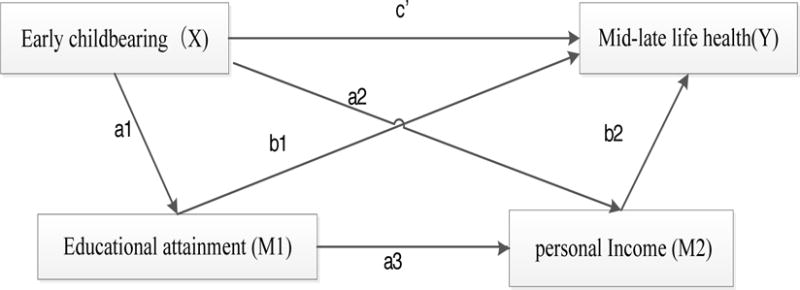
Multiple mediation pathway analysis
Data and Methods
Data
The data used in this paper are from the National Survey of the China Health and Retirement Longitudinal Study (CHARLS) conducted from 2011 to 2012. In this survey, a stratified (by per capita GDP of urban districts and rural counties) multi-stage (county/district, village/community, household), PPS (probability proportionate to size sampling) random sampling strategy was adopted. All the counties and districts in China are covered in this sampling except those in Tibet. The sample contains 450 villages/resident’s committees in 150 counties and districts throughout the country. As many as 17,708 people from 10,257 households with at least one person aged 45 or above responded to our questionnaire, with a response rate of 80.51%. The questionnaires consist of eight parts, among which the information about family members, health status, personal income, and household are included in our analysis. As this paper focuses on women aged 50 and above, we include 6,092 women after deleting outliers and cases with severe logical inconsistencies.
Variables
Dependent variables
In this paper, ADL functional status and self-rated health are used as dependent variables.
ADL functional status
ADL functional status: an index that indicates individual functional status of middle-aged and old women when they deal with activities of daily living (ADL) on their own. According to the international standard of Katz’s ADL index, ADL functional status contains six indices: these are the functional status of eating, dressing, transferring, bathing, using the toilet, and continence. In this paper, respondents who have no difficulties in all six activities are classified as “ADL active”, while the others are regarded as “ADL impaired” (Zeng and Vaupel, 2004). ADL-impaired respondents are assigned the number 1, and ADL active respondents are assigned 0.
Self-rated health
This is measured by the question: “how would you rate your health status?” Five answers are possible to this question: very good, good, fair, poor, and very poor. The question was asked twice, at both the beginning and the end of the survey. This paper takes the answer at the end as the respondents may be clearer about what “health condition” refers to. The self-rated health variable is treated as a binary variable, with very good and good set to 0, and fair, poor, and very poor set to 1.
Independent variables
Parity
Parity: the number of biological children of the respondents, including deceased children. For high parity, previous research suggests important distinctions at four+ (Grundy and Holt, 2000), five+ (Grundy and Tomassini, 2005; Spence, 2008), and six+ (Kington et al., 1997; Sudha et al., 2006). Given that 80% of the respondents in this paper were aged 50 to 69 and had 3.06 children on average, parity is set to 0 for women who have one to three children, and set to 1 when they have four children or more.
Early childbearing
Some scholars regard childbirth before the age of 20, 21, or 22 as early childbearing (Kington et al., 1997; Grundy and Holt, 2000; Alonzo, 2002; Mirowsky, 2005; Sudha et al., 2006; Henretta, 2007; Hank 2010). In this paper, we set the early childbearing age at 21. The variable is set to 1 if women gave birth before the age of 21, and otherwise it is set to 0.
Late childbearing
The age of 35 and older at estimated date of delivery has increasingly been acknowledged as advanced maternal age (Cleary-Goldman, et al.,2005; Delbaere et al., 2007). This paper defines late childbearing as a dichotomous variable, which is set to 0 if the last birth was before the age of 35, or 1 if the last birth was at 35 or above.
Control variables
In our analysis, we control for variables such as life habits in the past, characteristics in adolescence, social support and demographic characteristics.
Life habits of the past includes whether the respondent ever smoked (chewed tobacco, smoked a pipe, smoked self-rolled cigarettes, or smoked cigarettes/cigars) or drank (including beer, wine, or liquor).
Characteristics of adolescence include the residence type before age 16 (0=village, 1=city/town) and health condition before 15 (0=good, 1=fair or bad).
Social support is measured by whether the respondent is or is not living with one of her children.
Demographic characteristics include marital status (without a spouse, have a spouse), age group (50–59, 60–69, 70–79, 80 or above), whether the respondent is an agricultural worker, her household registration type (rural or urban), and living region (Eastern, Central and Western China)
Mediating variables
Mediating variables include educational attainment and personal income. Educational attainment includes 11 categories from illiterate to doctoral degree, and is treated as a continuous variable. Personal income is the sum of wage income, pensions and government subsidy.
The measurements and descriptive statistics of the variables are shown in Table 1.
Table 1.
Definition and descriptive statistics of variables
| Definition and measurement | %/M | SD | |
|---|---|---|---|
| Health outcomes | |||
| ADL impaireda | 0=ADL active | ||
| 1=ADL impaired | 21.96% | ||
| Self-rated health | 1=unhealthy | 80.14% | |
| Independent variables | |||
| Number of children | 1–12 | 3.06 | 1.56 |
| Paritya | 0=1 child to 3 children | ||
| 1=4 and more | 32.47% | ||
| Age at first birth | 15–49* | 24.39 | 4.24 |
| Age at last birth | 15–49* | 30.56 | 5.37 |
| Early childbearinga | 0= first birth at 21 or above | ||
| 1=first birth before 21 | 16.30% | ||
| Late childbearinga | 0=last birth before 35 | ||
| 1=last birth at 35 or above | 21.27% | ||
| Control variables | |||
| Life habits | |||
| Smokinga | 0=no 1=yes | 9.29% | |
| Drinkinga | 0=no 1=yes | 8.30% | |
| Characteristics in adolescence | |||
| Health during childhood up to and including 15a | 0=good | ||
| 1=fair or bad | 25.92% | ||
| Residence before 16 years old a | 0=village | ||
| 1=city/town | 10.37% | ||
| Social support | |||
| Living with childa | 0=no 1=yes | 51.38% | |
| Demographic variables | |||
| Marital status a | 0=without spouse | ||
| 1=have a spouse | 80.35% | ||
| Age | 50–100 | 61.98 | 8.505 |
| Age group (50–59)a | 0=50–59 | ||
| 1=60–69 | 33.67% | ||
| 2=70–79 | 14.74% | ||
| 3=80 or above | 4.49% | ||
| Worka | 0=others | ||
| 1=Engage in agricultural work | 48.19% | ||
| Household registration typea | 0=Rural | ||
| 1=Urban | 20.93 % | ||
| Region (Eastern region) | 34.72% | ||
| Central region | 33.08% | ||
| Western region | 32.21% | ||
| SES | |||
| Educational attainment | 1–1010 | 2.523.53 | 1.816.86 |
| Personal income (ln+1) | 0 – 12.28 | 2.88 | 4.10 |
Generally, childbearing age is limited to 15 to 49. In our data, there were some extreme outliers which were not acceptable and were deleted.
These are dummy variables
In this paper, as ADL functional status and the self-rated health are dichotomous variables, logistic regression models are employed.
Results
Descriptive results
As is shown in Table 1, among the 6,092 women aged 50 or above, the average parity is 3.06, the average age at first birth is 24.39, and the average age at last birth is 30.56. 21.96 percent of women suffer from ADL impairment, and 80.14% of women think their self-rated health is fair or bad. 32.47 percent of the women have four children or more. 16.30 percent of women had their first child before 21, 21.27 percent of women had their last child at 35 or above.
Before turning to the regression analyses, we examine the connection between childbearing history and ADL impairment using a contingency table, as shown in Table 2. 30.49 percent of women who have four children or more are ADL impaired, whereas only 17.87% of women with one to three children are ADL impaired. 28.10 percent of women who had their first child before the age of 21 are ADL impaired, while this drops to 20.77% for those who had their first child at or after 21. 31.33 percent of women who had children at or after 35 are ADL impaired, while only 19.43% of women who had their last birth before 35 are ADL impaired.
Table 2.
Frequency distribution of ADL-impaired by parity, early childbearing and late childbearing
| ADL impaired
|
χ2 | |||
|---|---|---|---|---|
| No | Yes | Total | ||
| (1) Parity | ||||
| One to three children | 3379 | 735 | 4114 | |
| 82.13% | 17.87% | 100% | 124.11*** | |
| Four children or more | 1375 | 603 | 1978 | |
| 69.51% | 30.49% | 100% | ||
| (2) Early childbearing | ||||
| First birth at or after 21 | 4040 | 1059 | 5099 | |
| 79.23% | 20.77% | 100% | 26.04*** | |
| First birth before 21 | 714 | 279 | 993 | |
| 71.90% | 28.10% | 100% | ||
| (3) Late childbearing | ||||
| Last birth at or after 35 | 890 | 406 | 1296 | |
| 68.67% | 31.33% | 100% | 84.22*** | |
| Last birth before 35 | 3864 | 932 | 4796 | |
| 80.57% | 19.43% | 100% | ||
p < 0.001
Regression results
ADL functional status
Table 3 presents the logistic regression results for ADL functional status. In Model 1, after controlling for covariates, we see that those who have four children or more are more likely to be ADL impaired than those with one to three children. Early childbearing women are more likely to suffer from ADL impairment than those without early childbearing. However the correlation of late childbearing with ADL impairment is not statistically significant.
Table 3.
Logistic regression for fertility history on ADL functional status
| Variables | ADL impaired
|
|
|---|---|---|
| Model 1 | Model 2 | |
| Coefficient | Coefficient | |
| Parity | 0.16* (0.08) |
0.12+ (0.08) |
| Early childbearing | 0.15+ (0.09) |
0.10 (0.09) |
| Late childbearing | 0.05 (0.09) |
0.02 (0.09) |
| Life habits | ||
| Smoking | 0.20+ (0.10) |
0.17+ (0.10) |
| Drinking | 0.25** (0.09) |
0.28** (0.09) |
| Characteristics in adolescence | ||
| Health during childhood up to and including 15 | 0.29*** (0.07) |
0.28*** (0.07) |
| Residence before 16 years old | −0.07 (0.15) |
0.14 (0.15) |
| Social support | ||
| Living with child | −0.09 (0.07) |
−0.09 (0.07) |
| Demographic variables | ||
| Marital status | −0.01 (0.09) |
−0.00 (0.09) |
| Age group(50–59) | ||
| 60–69 | 0.49*** (0.08) |
0.52*** (0.08) |
| 70–79 | 0.81*** (0.11) |
0.79*** (0.11) |
| Above 80 | 1.51*** (0.16) |
1.45*** (0.16) |
| Work | −0.39*** (0.07) |
−0.44*** (0.07) |
| Household registration type | −0.80*** (0.11) |
−0.53*** (0.12) |
| Region (Eastern region) | ||
| Central region | 0.42*** (0.08) |
0.40*** (0.08) |
| Western region | 0.52*** (0.08) |
0.48*** (0.08) |
| SES | ||
| Educational attainment | −0.11*** (0.02) |
|
| Personal income(ln+1) | −0.04*** (0.01) |
|
| _cons | −1.85*** (0.13) |
−1.47*** (0.14) |
|
| ||
| N | 6092 | 6092 |
| BIC | 6108.12 | 6073.81 |
Standard errors in parentheses
p< 0.1,
p< 0.05,
p< 0.01,
p< 0.001
In Model 2, educational attainment and personal income are added. Parity is still significantly related to ADL impairment, but the significance level is weaker than with Model 1. Also, the correlation between ADL functional status and early childbearing disappears. ADL impairment is significantly correlated with individual educational attainment and personal income. Higher personal income and better educational background will lower the risks of ADL impairment, which indicates that the association between early childbearing and ADL impairment is mediated by educational attainment and personal income. We will test this mediation below.
Using Model 2, women who have been engaged in agricultural work in the past year are less likely to be ADL impaired than nonagricultural workers. Unhealthy life habits are significantly correlated with ADL impairment; those who ever drank face a higher risk of ADL impairment. Women who were in poor health before age 15 are more likely to be ADL impaired.
We test for multiple mediation using a multiple-step multiple-mediator model (Preacher and Hayes 2008; Hayes et al. 2011). We used 5,000 bootstrap samples to obtain the bias-corrected 95 % confidence intervals for the total indirect effect (i.e., total mediated effect) and the specific indirect effects. The results indicate that there are two mediational paths as presented in Figure 2.
Figure 2.
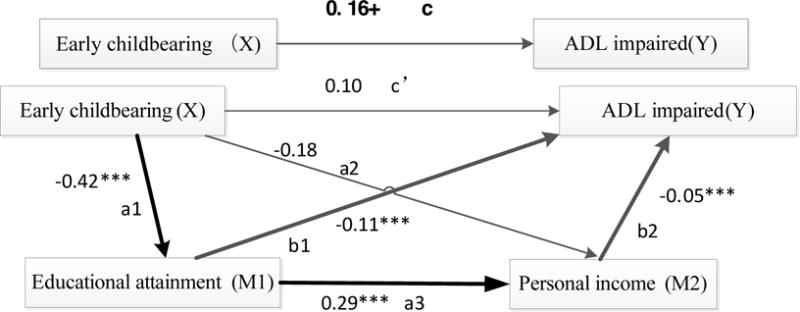
Multistep multiple-mediation analysis for ADL functional status +p< 0.1, *p< 0.05, **p< 0.01, ***p< 0.001
Self-rated health
Table 4 presents the regression results for self-rated health (SRH). In Model 1, after controlling for covariates, we see that women with four children or more are worse in self-rated health than those who have one to three children. In Model 2, we include educational attainment and personal incomes. The association between parity and self-rated health is still statistically significant, whereas early childbearing and late childbearing are no longer significant. Self-rated health is significantly correlated with educational attainment and personal income. Women with higher personal income and better educational background will be in better self-rated health.
Table 4.
Logistic regression for fertility history on self-rated health
| Variables | Fair and poor self-rated health
|
|
|---|---|---|
| Model 1 | Model 2 | |
| Coefficient | Coefficient | |
| Parity | 0.19* (0.09) |
0.16+ (0.09) |
| Early childbearing | 0.09 (0.10) |
0.06 (0.10) |
| Late childbearing | 0.04 (0.10) |
0.02 (0.10) |
| Life habits | ||
| Smoking | −0.02 (0.11) |
−0.04 (0.11) |
| Drinking | −0.38*** (0.09) |
−0.36*** (0.09) |
| Characteristics in adolescence | ||
| Health during childhood up to and including 15 | 1.02*** (0.09) |
1.02*** (0.09) |
| Residence before 16 years old | −0.18 (0.12) |
−0.08 (0.13) |
| Social support | ||
| Living with child | −0.06 (0.07) |
−0.06 (0.07) |
| Demographic variables | ||
| Marital status | 0.01 (0.09) |
0.01 (0.10) |
| Age group (50–59) | ||
| 60–69 | 0.14+ (0.08) |
0.16* (0.08) |
| 70–79 | −0.05 (0.12) |
−0.05 (0.12) |
| Above 80 | 0.16 (0.20) |
0.13 (0.20) |
| Work | −0.17* (0.08) |
−0.22** (0.08) |
| Household registration type | −0.26* (0.11) |
−0.10 (0.11) |
| Region (Eastern region) | ||
| Central region | 0.38*** (0.08) |
0.35*** (0.08) |
| West region | 0.58*** (0.08) |
0.54*** (0.08) |
| SES | ||
| Educational attainment | −0.04* (0.02) |
|
| Personal income(ln+1) | −0.03*** (0.01) |
|
| _cons | 1.02*** (0.13) |
1.23*** (0.14) |
|
| ||
| N | 6092 | 6092 |
| BIC | 5956.75 | 5956.44 |
Standard errors in parentheses
p< 0.1,
p< 0.05,
p< 0.01,
p< 0.001
We also see with Model 2 that middle-aged and older women who have been engaged in agricultural work in the past year have better self-rated health. There is a positive correlation between self-rated health and health condition before age 15.
Figure 3 shows the multiple mediation analysis of early childbearing on self-rated health. The results indicate that the association between early childbearing and SRH is mediated by educational attainment and personal income, as indicated in Figure 3.
Figure 3.
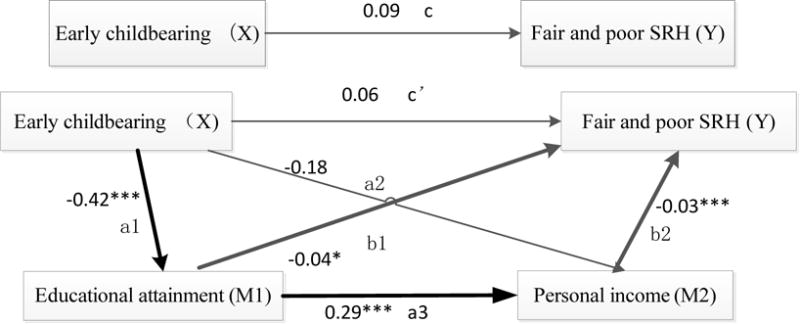
Multistep multiple-mediation analysis for SRH. +p< 0.1, *p< 0.05, **p< 0.01, ***p< 0.001
Discussion and Conclusions
China is confronted with a severe aging problem. Due to their biological characteristics and social role, women have poorer health than men (Zhao et al., 2014), a problem that demands attention. Using the national baseline data of CHARLS, we analyzed the correlation between women’s fertility history and mid- and late-life health. Our findings are as follows.
We validate hypothesis 1 that parity is related to the health of Chinese middle-aged and older women. Women with four children or more are likely to experience ADL impairment and poorer self-rated health, consistent with previous findings in Western countries (Kington et al., 1997; Grundy and Holt, 2000; Grundy and Tomassini, 2005; Sudha et al., 2006; Read et al., 2011). Insufficient nutrition will have strongly negative effects on women’s physical condition (Santow, 1995). Due to the backward economy of China from the 1960s to the 1980s, during which most women in this study were of childbearing age, women could not obtain enough of the nutrition needed for healthy pregnancy and delivery. Moreover, the outdated fertility customs and culture did great harm to their health (Zhuang, 2006), leading to poor health in mid-late life. In that specific context, women with more children are more likely to be in poorer health in late life. The accumulated physiological stress can affect women’s health in the long term.
However, some researchers believe that there is no correlation between parity and the later health of Chinese women (Liu, 2004; Chen and Lei, 2009). This inconsistency may be due to the different data analyzed. Liu (2004) and Chen and Lei (2009) used the data from CLHLS, which mainly contains samples of the oldest-old. It may also be caused by differences in the way health status is measured.
Our results partly support hypothesis 2. We find that early childbearing is associated with ADL impairment, and this association is mediated by educational attainment and personal income. We find no direct association between early childbearing and self-rated health, but we discern an indirect-only mediation effect of early childbearing via educational attainment and personal income on later life self-rated health. Our finding of an association between ADL impairment and early childbearing is consistent with previous studies (Grundy and Holt, 2000; Grundy and Tomassini, 2005; Mirowsky, 2005; Spence, 2008; Grundy, 2009; Read et al., 2011). Middle-aged and older women with early childbearing have worse health. As the reproductive systems of women haven’t been fully developed, it is more common for those who have their first birth before 21 to suffer complications in pregnancy and childbirth (Mirowsky, 2005). As a matter of fact, first childbirth at a young age is often related to high parity, which generates further pressures on women’s health (Read et al., 2011). However, when we include other characteristics of older women in our models, we find that this association between early childbearing and ADL impairment is mediated by educational attainment and personal income. Early childbearing may lead to a poor start in the life course (Moore et al. 1994). In the USA, some studies have indicated that early childbearing leads to truncated education and subsequent adverse social outcomes, for example, no stable job and low family income (Mirowsky, 2005). The accumulated disadvantage and stress create an enduring risk to mid-late life health.
We find no correlation between late childbearing and poor mid-late life health for Chinese females, which does not support hypothesis 3. The relationship between mid-late life health and late childbearing found in this paper is inconsistent with many studies in Western countries (Alonzo, 2002; Mirowsky, 2002), and inconsistent with findings from other Chinese data by Zeng and Vaupel (2004). This may be due to the different samples studied; in our analysis, women are aged 50 or above with an average age of 62, while those in Zeng and Vaupel’s research are over 80 with an average age of 92.
We also find that women who were healthier during adolescence enjoy better health in later life, as is the case with those who have been engaged in agricultural work in the past year. Experiences during adolescence are connected with one’s mid-late life health (Srinivasan, et al., 1996; Hayward and Gorman, 2004). There is a positive correlation between health condition during adolescence and mid-late life (Zhong, 2014). Therefore, maintaining good health during adolescence is critical to the mid-late life health of women. Women who have been engaged in agricultural work are better in health condition, suggesting that a moderate amount of physical labor is beneficial to health in later life.
There are some limitations to our study. For example, women without children are excluded from the samples. Previous research has shown that women without children are in worse health than those with children (Grundy and Tomassini, 2005). Due to limitation of available data, information on infant deaths and abortions are not considered here. It has been confirmed in some studies that women who experienced death of an infant or abortion have poor health in later life (Alonzo, 2002; Mirowsky, 2005; Sudha et al., 2006; Henretta, 2007; Hank, 2010).
Due to the steady improvement in living conditions and healthcare, and rapid development of medical knowledge, various diseases have been effectively prevented or cured, thus delaying the human aging process. However, for better mid-late life health, reproductive women should plan their number of desired children as well as the timing of births. Importantly, both families and public policy should pay more attention to the health of females during adolescence.
Footnotes
This work was supported by the HSSTP project of Shaanxi province (China)
Contributor Information
Xiaomin Li, Institute for Population and Development Studies, Xi’an Jiaotong University (China), Xi’an City, Shaanxi Province, 710049, China.
Quanbao Jiang, Institute for Population and Development Studies, Xi’an Jiaotong University, Xi’an City, Shaanxi Province, 710049, China.
Shuzhuo Li, Institute for Population and Development Studies, Xi’an Jiaotong University, Xi’an City, Shaanxi Province, 710049, China
Marcus W. Feldman, Morrison Institute for Population and Resource Studies, Stanford University, Stanford, CA 94305, USA
References
- Albrektsen G, Heuch I, Hansen S, &Kvåle G. Breast cancer risk by age at birth, time since birth and time intervals between births: exploring interaction effects. British Journal of Cancer. 2005;92(1):167–175. doi: 10.1038/sj.bjc.6602302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alonzo AA. Long-term health consequences of delayed childbirth: NHANES III. Women’s Health Issues. 2002;12(1):37–45. doi: 10.1016/s1049-3867(01)00135-9. [DOI] [PubMed] [Google Scholar]
- Chen GD, Lei XY. “Fertility effect” or “supporting effect?” -Quantity of children and parental health. Frontiers of Economics in China. 2009;4(4):601–616. [Google Scholar]
- Cleary-Goldman J, Malone FD, Vidaver J, Ball RH, Nyberg DA, Comstock CH. Impact of maternal age on obstetric outcome. Obstetrics & Gynecology. 2005;105(5):983–990. doi: 10.1097/01.AOG.0000158118.75532.51. [DOI] [PubMed] [Google Scholar]
- Delbaere I, Verstraelen H, Goetgeluk S, Martens G, De Backer G, Temmerman M. Pregnancy outcome in primiparae of advanced maternal age. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2007;135(1):41–46. doi: 10.1016/j.ejogrb.2006.10.030. [DOI] [PubMed] [Google Scholar]
- Duan T. An Exploratory Discussion on the Lateralization of Rural Females in Distribution of Household Resources in the Underdeveloped Areas in Western China. Journal of Shaanxi Normal University (Philosophy and Social Sciences Edition) 2008;37(1):122–128. in Chinese. [Google Scholar]
- Geng D. Study on the children number and parental health condition. South China Population. 2013;28(3):8–16. in Chinese. [Google Scholar]
- Grundy E, Holt G. Adult life experiences and health in early old age in Great Britain. Social Science & Medicine. 2000;51(7):1061–1074. doi: 10.1016/s0277-9536(00)00023-x. [DOI] [PubMed] [Google Scholar]
- Grundy E, Tomassini C. Fertility history and health in later life: a record linkage study in England and Wales. Social Science & Medicine. 2005;61(1):217–228. doi: 10.1016/j.socscimed.2004.11.046. [DOI] [PubMed] [Google Scholar]
- Grundy E. Women’s fertility and mortality in late mid life: a comparison of three contemporary populations. American Journal of Human Biology. 2009;21(4):541–547. doi: 10.1002/ajhb.20953. [DOI] [PubMed] [Google Scholar]
- Hank K. Childbearing history, later-life health, and mortality in Germany. Population Studies. 2010;64(3):275–291. doi: 10.1080/00324728.2010.506243. [DOI] [PubMed] [Google Scholar]
- Hayward MD, Gorman BK. The long arm of childhood: the influence of early-life social conditions on men’s mortality. Demography. 2004;41(1):87–107. doi: 10.1353/dem.2004.0005. [DOI] [PubMed] [Google Scholar]
- Hayes AF, Preacher KJ, Myers TA. Mediation and the estimation of indirect effects in political communication research. Sourcebook for political communication research: Methods, measures, and analytical techniques. 2011:434–465. [Google Scholar]
- Henretta JC. Early childbearing, marital status, and women’s health and mortality after age 50. Journal of Health and Social Behavior. 2007;48(3):254–266. doi: 10.1177/002214650704800304. [DOI] [PubMed] [Google Scholar]
- Huang G. Study on the traditional customs and reproductive health. Social Sciences in Yunnan. 1996;15(4):64–69. in Chinese. [Google Scholar]
- Jiang Q, Li Y, Sánchez Barricarte JJ. Fertility intention, son preference and second childbirth–Survey findings from Shaanxi Province of China. Social Indicators Research. 2016;125(3):935–953. doi: 10.1007/s11205-015-0875-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kington R, Lillard L, Rogowski J. Reproductive history, socioeconomic status, and self-reported health status of women aged 50 years or older. American Journal of Public Health. 1997;87(1):33–37. doi: 10.2105/ajph.87.1.33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu J. The effect of number of children on quality of the Chinese rural oldest-old. Chinese Journal of Population Science. 2004;18(1):48–54. in Chinese. [Google Scholar]
- McElroy Susan W. Early childbearing, high school completion and college enrollment: evidence from 1980 High School Sophomores. Economics of Education Review. 1996;15(3):303–24. [Google Scholar]
- Mirowsky J. Parenthood and health: The pivotal and optimal age at first birth. Social Forces. 2002;81(1):315–349. [Google Scholar]
- Mirowsky J. Age at first birth, health, and mortality. Journal of Health and Social Behavior. 2005;46(1):32–50. doi: 10.1177/002214650504600104. [DOI] [PubMed] [Google Scholar]
- Moore Kristin A, Myers David E, Morrison Donna Ruane, Nord Christine Winquist, Brown Brett, Edmonston Barry. Age at First Childbirth and Later Poverty. Journal of Research on Adolescence. 1994;3(4):393–422. doi: 10.1207/s15327795jra0304_5. [DOI] [PubMed] [Google Scholar]
- Population Census Office under the State Council (PCO) Tabulation on the 2010 Population Census of the People’s Republic of China. Beijing: China Statistics Press; 2012. [Google Scholar]
- Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior research methods. 2008;40(3):879–891. doi: 10.3758/brm.40.3.879. [DOI] [PubMed] [Google Scholar]
- Qi X. Study on the fertility culture between the east and the west. Beijing: China Population Publishing House; 2006. pp. 48–60. in Chinese. [Google Scholar]
- Read S, Grundy E, Wolf DA. Fertility history, health, and health changes in later life: A panel study of British women and men born 1923–49. Population Studies. 2011;65(2):201–215. doi: 10.1080/00324728.2011.572654. [DOI] [PubMed] [Google Scholar]
- Santow G. Social roles and physical health: the case of female disadvantage in poor countries. Social Science & Medicine. 1995;40(2):147–161. doi: 10.1016/0277-9536(94)e0069-5. [DOI] [PubMed] [Google Scholar]
- Srinivasan SR, Bao W, Wattigney WA, Berenson GS. Adolescent overweight is associated with adult overweight and related multiple cardiovascular risk factors: the Bogalusa Heart Study. Metabolism. 1996;45(2):235–240. doi: 10.1016/s0026-0495(96)90060-8. [DOI] [PubMed] [Google Scholar]
- Snowdon DA, Kane RL, Beeson WL, Burke GL, Sprafka JM, Potter J, Phillips RL. Is early natural menopause a biologic marker of health and aging? American Journal of Public Health. 1989;79(6):709–714. doi: 10.2105/ajph.79.6.709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spence NJ. The long-term consequences of childbearing–physical and psychological well-being of mothers in later life. Research on Aging. 2008;30(6):722–751. doi: 10.1177/0164027508322575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sudha S, Mutran EJ, Williams IC, Suchindran C. Childbearing history and self-reported well-being in later life–Contrasting Older African American and White Women. Research on Aging. 2006;28(5):599–621. [Google Scholar]
- Yao Y. Study on the fertility culture and birth custom problems. Population Journal. 2000;22(2):15–18. in Chinese. [Google Scholar]
- Zhao L. Master’s Thesis. Sichuan Normal University; 2009. Research on Women’s Health Care at the Early Days of New China (1949–1959) in Chinese. [Google Scholar]
- Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: The China health and retirement longitudinal study (CHARLS) International journal of epidemiology. 2014;43(1):61–68. doi: 10.1093/ije/dys203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeng Y, Vaupel JW. Association of late childbearing with healthy longevity among the oldest-old in China. Population Studies. 2004;58(1):37–53. doi: 10.1080/0032472032000175437. [DOI] [PubMed] [Google Scholar]
- Zheng Z. Consideration on reproductive health research: Decomposition and integration. Population Research. 1997;21(6):63–67. in Chinese. [Google Scholar]
- Zhuang Y. PhD Dissertation. Xiamen University; 2006. Study on the Cost of Social Procreation. in Chinese. [Google Scholar]
- Zhong Y. PhD Dissertation. Shandong University; 2014. Study on the Relationship between Socioeconomic Status in Childhood and the Middle Aged and Later Health. in Chinese. [Google Scholar]