

Abstract
Objectives:
To create a food frequency questionnaire specifically designed to capture the dietary habits of Saudis and test its validity and reliability.
Methods:
This investigation is a longitudinal, test-retest study conducted in King Saud University, Riyadh, Kingdom of Saudi Arabia between December 2015 and March 2016. A list of 140 food items was included in the questionnaire where a closed-ended and open-ended approach was used. Regarding past year food frequency consumption and 24 hours dietary recall, body weight and height were collected. Internal consistency, test-retest reliability, completeness of the food list, and criterion validity were assessed.
Results:
One-hundred and thirty eight participants were interviewed to complete the 24 hours dietary recall and the constructed questionnaire. Approximately 85% of the food items reported in the dietary recall were covered in the food frequency questionnaire. The association of body mass index with meats (regression coefficients: 2.28) and dairy products consumption frequency was statistically significant (regression coefficients: 2.31). A high overall reproducibility rate of the questionnaire was detected (Pearsons’ correlation coefficient: 0.78 p<0.001).
Conclusion:
The developed questionnaire has a high reliability and reasonable validity, and suitable for use in nutritional epidemiological investigations in Saudi Arabia.
Kingdom of Saudi Arabia (KSA) witnessed a dramatic increase in the prevalence of obesity, diabetes, and metabolic syndrome during the past 2 decades.1,2 According to the World Health Organization, cardiovascular diseases and diabetes are responsible for half the deaths among the Saudi population.3 This epidemic is partially explained by the unhealthy eating behaviors of the Saudis, leading to a higher prevalence of obesity and overweight people and subsequent chronic non-communicable diseases.4-7 Several nutritional investigations were conducted in KSA to measure the eating behavior of Saudis, methods of measuring dietary habits varied between the use of 24-hours dietary recall,8 food records,6 and limited questionnaires measuring consumption of selected food items.9 A study conducted among male school children in Al-Hasa, KSA utilized the Youth and Adolescent Food Frequency Questionnaire to measure eating behavior.5 However, several food items listed in this questionnaire are not permitted in KSA or are not usually consumed in the country.10,11 Several methods are used to measure dietary habits. Dietary recall depends on the ability of individuals to recall food and beverages consumed in a specific period of time, usually the previous 24 hours.12 When using food records, participants are asked to record their food intake on a daily basis. It does not rely on memory and participants can proactively record their intake of the day.13 Food Frequency Questionnaires ask the participants how frequently they consume several food items over a fixed time period (usually a year). This method can be self-administered or completed during interviews. This method is more suitable for large-scale epidemiological studies compared with 24-hour food recall or food diaries.14 Cultural variations exhibited between geographical areas mandated development of food frequency questionnaires suitable for a particular region. For example, there are different food frequency questionnaires developed for European,15,16 Asian17-19 and American populations.20 Food frequency questionnaires developed for Arab nations are limited. Two questionnaires, developed for Lebanese population21 and Kuwaiti and Emirati populations,22 were detected. However, there is no validated and reliable food frequency questionnaire specifically created for the Saudi population. The Use of a questionnaire specifically designed for Saudis is necessary to ensure consistency of nutritional epidemiological investigations performed in this population. This study aims to create a food frequency questionnaire specifically designed to capture the nutritional habits of Saudis and to test its validity and reliability.
Methods
Study context and participants
This investigation is a longitudinal, test-retest study, which involved students from King Saud University (KSU), Riyadh, KSA. The study was conducted between December 2015 and March 2016 and involved university students of both genders and different colleges in the university. Ethical approval to conduct the study was provided by the Ethics Committee in Department of Family and Community Medicine, College of Medicine, KSU. A sample of 130 subjects was estimated to detect a Pearsons’s correlation coefficient of 0.25 assuming probability of 5% type 1 error and 90% study power to detect the effect. Providing the longitudinal nature of this study, an attempt to recruit larger sample was made to avoid reduction of sample size caused by attrition. Participants were requested to sign a consent form for approval to participate in the study. Subjects were excluded from this investigation if any prior medical history of conditions that might interfere with average eating behavior was present. These conditions involved Bulimia nervosa, Anorexia nervosa, Binge eating, inflammatory bowel disease, peptic diseases, intestinal motility disorders, cancer, hyperthyroidism and hypothyroidism.
Construction of the food frequency questionnaire
The design of the food frequency questionnaire was adopted from the food frequency questionnaire developed by the European Prospective Investigation into Cancer and Nutrition study (EPIC).23 This design was selected as its validity and reliability was previously tested24 and it seemed more convenient to complete compared with other observed questionnaires. Similarly, portion sizes were adopted from the EPIC food frequency questionnaire. The constructed questionnaire was developed in the Arabic language. A list of 140 food items was included in the questionnaire where a closed-ended approach was used. Nine answering options were provided for each closed-ended question where consumption frequency choices were stated as the following: never or less than a month, 1-3 per month, once a week, 2-4 per week, 5-6 per week, once a day, 2-3 per day, 4-5 per day, 6+ per day. Open-ended questions were added at the end of the questionnaire to gather information regarding other food items not listed. Questions regarding type of cooking fat, visible fat consumption, consumption of salt and vitamins were added.
Validity and reliability assessment
Validity of the questionnaire was tested on several levels. Pilot testing of the questionnaire was performed to test the initially compiled food list where 10 male and 10 female participants were recruited to investigate the ability of the respondents to complete the questionnaire, assess clarity of the questionnaire and the need to add or delete food items. Average time needed to fill in the questionnaire was tested during this stage. After the pilot stage, assessment of the questionnaire was conducted in 2 steps. Firstly, participants were requested to complete the self-administered food frequency questionnaire and a qualitative, open-ended 24-hour dietary recall. The dietary recall was performed via interviews where information related to type of food, quantity consumed and time of consumption during the previous 24 hours were recorded. Interviews were conducted via trained medical students and supervised by an expert in nutritional epidemiology. A comparison between findings of the semi-quantitative food frequency questionnaire and the qualitative dietary recall was performed to test the completeness of the food frequency questionnaire list through assessment of its comprehensiveness to capture eating habits of the study participants.
Participants were asked about their weight and height to facilitate calculation of Body mass index which was used to test the validity of the questionnaire. Assessment of BMI as a test of the validity of the questionnaire was based on the assumption that higher consumption frequency of food items rich in carbohydrates and fats might be associated with higher levels of BMI compared with higher consumption of food items with high level of fibres content such as fruits and vegetables. Two tests of reliability were conducted. Firstly, internal consistency was evaluated by Cronbach’s alpha test. Secondly, test-retest reliability was assessed via filling the questionnaire twice where the second questionnaire was filled one month after filling the first questionnaire.
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (IBM Corp, Armonk, NY, USA) version 22. A scoring system was developed to measure food consumption frequency. For example, items which are never or rarely consumed were given a score of zero while items which were consumed more than 6 times on a daily basis were given a score of 9. A sum of consumption frequency scores was calculated for each food category to tests its association with BMI and to test the reproducibility. Frequencies and proportions were calculated to describe binary and categorical variables. Means and standard deviations were calculated to illustrate continuous variables. Univariate regression analysis was performed to test the association between consumption scores and BMI. Pearson correlation coefficients were calculated to test the test-retest reliability of the questionnaire and Cronbach’s alpha test was used to assess the internal consistency of the questionnaire. A p-value of 0.05 or less was designated as statistically significant for applied statistical tests.
Results
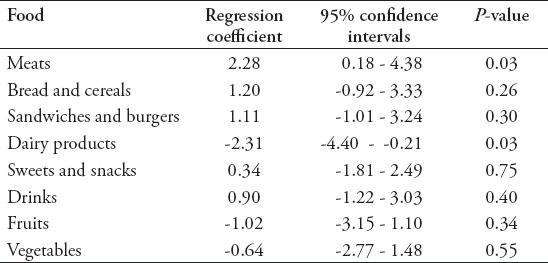
A total of 141 participants were approached in this investigation where 3 participants were excluded due to prior medical history of celiac disease and inflammatory bowel disease. Table 1 describes demographic information of the participants. Mean age of the participants was 20.66 years where proportion of male participants was higher (57%). The average BMI of the participants was 25.5 where males had a higher average BMI compared with females. During the pilot stage, participants were able to answer the questionnaire without assistance. Average time spent on completing the questionnaire varied between 15 and 20 minutes. All of the 138 participants were interviewed to complete the 24 hours dietary recall. However, only 77% (107 participants) had their follow up questionnaire completed. The qualitative dietary recall data was compiled to identify food items reported by the participants. Approximately 85% of the food items reported in the dietary recall were covered in the food frequency questionnaire. This indicates a good coverage of the questionnaire and ability to capture average eating behavior of Saudis. Table 2 summarizes the most and least frequently consumed food items in the study within each food category. Most of the participants reported a high frequency of chicken kabsa and white bread consumption. There was also reported a high frequency of food items with high calorific values, such as chocolate, added sugar, and dates. Low fat and low sugar products are not frequently consumed by the study sample, which was apparent on low consumption frequency of low fat dairy products and diet soft drinks. Assessment of the association between consumption of food items within specific food categories and BMI is illustrated in Table 3. Higher consumption of meats, bread and cereals, sandwiches and burgers, sweets, snacks and drinks were associated with a higher level of BMI. However, only association with meats consumption was statistically significant suggesting higher levels of BMI with increased consumption frequency of meats. Meat products are usually served with rice or bread in KSA, which might provide partial explanation of the association between BMI and meats frequency consumption. Consumption of dairy products, fruit and vegetables was associated with a reduced level of BMI where only dairy product association was statistically significant. The negative association between BMI and frequency of dairy products consumption can be partially explained by the availability of several low fat dairy products and the lower calorific values of several full fat dairy products in comparison with other food items such as sweets and snacks. Although a larger sample size is needed to test the weaker associations, observing a negative association between consumption frequency of dairy products, fruit and vegetables, which have lower calorific values compared with other food items in other categories, indicate a reasonable criterion validity of the current questionnaire.
Table 1.
Demographic information of the Saudi food frequency development study participants (N=138).
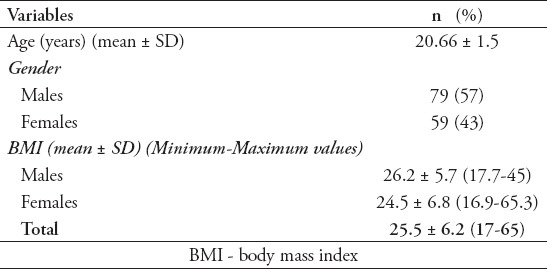
Table 2.
Summary of most and least frequently consumed food items reported via a constructed food frequency questionnaire for Saudis (N=138).
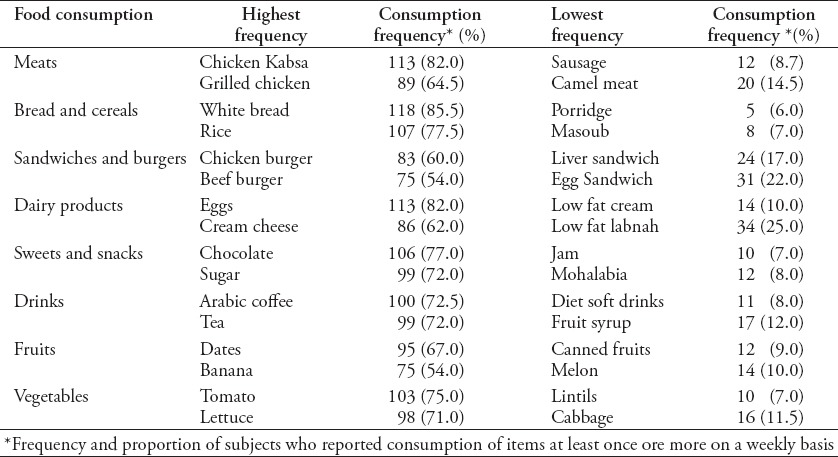
Table 3.
Univariate regression analysis of body mass index depending on consumption frequency within each food category of 138 Saudi participants who completed a developed Saudi food frequency questionnaire.
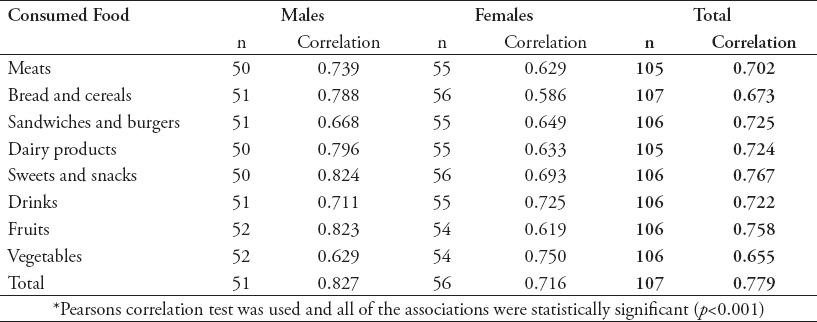
The internal consistency of the questionnaire was high as Cronbach’s alpha of the total scale was 0.938. The test-retest reliability of completed questionnaires indicates a high reproducibility of the questionnaire (Table 4). The overall reproducibility of the questionnaire was 0.78 (p<0.001). Upon investigating reproducibility among food categories, the sweets and snacks section has the highest reproducibility rate and the vegetables section had the lowest rate. When comparing male to female reproducibility rates, it appears that male participants’ reproducibility rates were higher, except for drinks and vegetables.
Table 4.
Test-retest reliability of food consumption frequency of the developed Saudi food frequency questionnaire*.
Discussion
This study was aiming to create and test the validity and reliability of a food frequency questionnaire suitable for the Saudi population. The participants were able to understand the questions and to complete the questionnaire without difficulties. The completeness of the food list was tested by comparing the semi-quantitative questionnaire to a qualitative dietary recall where 85% of the food items reported in the dietary recall were covered by the food frequency questionnaire. The criterion validity was tested by assessing the association between BMI and consumption frequency where associations with meat and dairy consumption frequency were statistically significant. The questionnaire is highly reproducible where statistically significant correlations between first and second trials were detected. This study can be compared with other studies assessing development of food frequency questionnaires for Kuwaiti and Emirati populations and Lebanese children population. Both studies developed the questionnaire in a manner similar to the current study where the food items list was compared with 24-hour dietary recall to assess completeness of the list. Additionally, the study by Dhegane et al22 used a similar approach of assigning frequency consumption scores for food categories. However, they did not assess the reliability of the questionnaire.
The number of food items covered in the current food frequency questionnaire reached up to 140 food items. This number was similar to the number of food items listed in other European questionnaires (130 food items)23 and an Australian questionnaire (129 food items).25 However, the number of food items used in the Kuwaiti food frequency questionnaire was higher (152 food items).22 A food frequency questionnaire developed in Shanghai, China was composed of 81 food items where the list covered 86% of the food items reported in the dietary recalls.17 This might indicate that the length of the food items list is affected by cultural variations between populations.
Most studies that tested validity and reliability of food frequency questionnaires used calorific values or nutrient contents when comparing food frequency questionnaires with other reference methods. The study by Katsouyanni et al16 tests the validity of a Greek food frequency questionnaire by comparing nutrient intake estimated using the questionnaire to nutrient levels obtained by venous blood and urine samples. Reasonable correlations between the 2 methods were detected. Another study made a comparison between 3-day food diaries and semi-quantitative food frequency questionnaires. Three-day food records were conducted 4 times in a year to detect seasonal variations. The overall average calorific intake calculated was similar in both methods. The Pearson correlation coefficient between the energy intake calculated in both methods was 0.42 after adjusting for gender.26 Similarly, another study assessed the association between 7-day diary records and food frequency questionnaires and revealed a similar agreement.27
This study was able to create a semi-quantitative food frequency questionnaire suitable for the Saudi population and compared its comprehensiveness with the qualitative dietary recall method. This questionnaire has a higher reproducibility rate.
Study limitations
Major limitations of this investigation are mainly related to the use of reported weight and height of the participants instead of objective measurement. Although this might introduce measurement bias of BMI, studies have reported an acceptable agreement between measured and reported weight and height.28,29 This study was not able to estimate calorific intake or nutrient intake based on the answered questionnaire. This is due to the fact that there is currently no Saudi nutritional database available for researchers to facilitate nutritional epidemiological investigations capable of correlating food consumption frequency with energy and nutrient intake.
In conclusion, developed Saudi Food Frequency Questionnaire has a high reproducibility rate. Testing suitability, completeness and criterion validity revealed straightforwardness, comprehensiveness and ability to capture dietary behavior of Saudi subjects. This data collection tool can be suitable for large scale nutritional epidemiological investigations conducted in KSA.
Acknowledgment
Authors are grateful to the Deanship of Scientific Research, King Saud University, Riyadh, Kingdom of Saudi Arabia for funding through Vice Deanship of Scientific Research Chairs.
Footnotes
References
- 1.Al Dawish MA, Robert AA, Braham R, Al Hayek AA, Al Saeed A, Ahmed RA, et al. Diabetes Mellitus in Saudi Arabia: A Review of the Recent Literature. Curr Diabetes Rev. 2016;12:359–368. doi: 10.2174/1573399811666150724095130. [DOI] [PubMed] [Google Scholar]
- 2.M Alquaiz A, R Siddiqui A, H Qureshi R, A Fouda M, A Almuneef M, A Habib F, et al. Women Health in Saudi Arabia: A review of non-communicable diseases and their risk factors. Pak J Med Sci. 2014;30:422–431. [PMC free article] [PubMed] [Google Scholar]
- 3.World Health Organization. Diabetes Country Profiles, Saudi Arabia. [Updated 2016, Cited 2017 February 22]. Available from: http://www.who.int/diabetes/country-profiles/sau_en.pdf?ua=1 .
- 4.Bin Horaib G, Al-Khashan HI, Mishriky AM, Selim MA, Alnowaiser N, Binsaeed AA, et al. Prevalence of obesity among military personnel in Saudi Arabia and associated risk factors. Saudi Med J. 2013;34:401–407. [PubMed] [Google Scholar]
- 5.Amin TT, Al-Sultan AI, Ali A. Overweight and Obesity and their Association with Dietary Habits, and Sociodemographic Characteristics Among Male Primary School Children in Al-Hassa, Kingdom of Saudi Arabia. Indian J Community Med. 2008;33:172–181. doi: 10.4103/0970-0218.42058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Washi SA, Ageib MB. Poor diet quality and food habits are related to impaired nutritional status in 13- to 18-year-old adolescents in Jeddah. Nutr Res. 2010;30:527–534. doi: 10.1016/j.nutres.2010.07.002. [DOI] [PubMed] [Google Scholar]
- 7.Al-Hazzaa HM, Abahussain NA, Al-Sobayel HI, Qahwaji DM, Musaiger AO. Physical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and region. Int J Behav Nutr Phys Act. 2011;8:140. doi: 10.1186/1479-5868-8-140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Alkoly TA, AbdAllah AM, Alghamidi AK. Nutritional Status and Eating Behaviors among Adolescents of Some Intermediate Schools in Jeddah. Journal of King Abdulaziz University. 2011;18:1–18. [Google Scholar]
- 9.Ministry of Health. Health Information Survey. 2013. [Cited 2017 February 22]. Available from: http://www.moh.gov.sa/en/ministry/statistics/pages/healthinformatics.aspx .
- 10.Rockett HR, Breitenbach M, Frazier AL, Witschi J, Wolf AM, Field AE, et al. Validation of a youth/adolescent food frequency questionnaire. Prev Med. 1997;26:808–816. doi: 10.1006/pmed.1997.0200. [DOI] [PubMed] [Google Scholar]
- 11.Rockett HR, Wolf AM, Colditz GA. Development and reproducibility of a food frequency questionnaire to assess diets of older children and adolescents. J Am Diet Assoc. 1995;95:336–340. doi: 10.1016/S0002-8223(95)00086-0. [DOI] [PubMed] [Google Scholar]
- 12.Medical Research Council. Dietary assessment - Recalls, Council MR. [cited 2017 February 22nd]. Available from: http://dapa-toolkit.mrc.ac.uk/dietary-assessment/methods/recalls/index.php .
- 13.Council MR. Dietary assessment - Weighed food diary. [cited 2017 February 22]. Available from: http://dapa-toolkit.mrc.ac.uk/dietary-assessment/methods/weighed-food-diary/index.php .
- 14.Council MR Dietary assessment - Food frequency questionnaire. [cited 2017 February 22]. Available from: http://dapa-toolkit.mrc.ac.uk/dietary-assessment/methods/food-frequency-questionnaire/index.php .
- 15.Johansson I, Hallmans G, Wikman A, Biessy C, Riboli E, Kaaks R. Validation and calibration of food-frequency questionnaire measurements in the Northern Sweden Health and Disease cohort. Public Health Nutr. 2002;5:487–496. doi: 10.1079/phn2001315. [DOI] [PubMed] [Google Scholar]
- 16.Katsouyanni K, Rimm EB, Gnardellis C, Trichopoulos D, Polychronopoulos E, Trichopoulou A. Reproducibility and relative validity of an extensive semi-quantitative food frequency questionnaire using dietary records and biochemical markers among Greek schoolteachers. Int J Epidemiol. 1997;26:S118–S127. doi: 10.1093/ije/26.suppl_1.s118. [DOI] [PubMed] [Google Scholar]
- 17.Shu XO, Yang G, Jin F, Liu D, Kushi L, Wen W, et al. Validity and reproducibility of the food frequency questionnaire used in the Shanghai Women’s Health Study. Eur J Clin Nutr. 2004;58:17–23. doi: 10.1038/sj.ejcn.1601738. [DOI] [PubMed] [Google Scholar]
- 18.Ahn Y, Kwon E, Shim JE, Park MK, Joo Y, Kimm K, et al. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur J Clin Nutr. 2007;61:1435–14341. doi: 10.1038/sj.ejcn.1602657. [DOI] [PubMed] [Google Scholar]
- 19.Wakai K. A Review of Food Frequency Questionnaires Developed and Validated in Japan. J Epidemiol. 2009;19:1–11. doi: 10.2188/jea.JE20081007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Institute NC. Usual Dietary Intakes: NHANES Food Frequency Questionnaire (FFQ) 2015. [cited 2016 May 27]. Available from: http://epi.grants.cancer.gov/diet/usualintakes/ffq.html?&url=/diet/usualintakes/ffq.html .
- 21.Moghames P, Hammami N, Hwalla N, Yazbeck N, Shoaib H, Nasreddine L, et al. Validity and reliability of a food frequency questionnaire to estimate dietary intake among Lebanese children. Nutr J. 2016;15:4. doi: 10.1186/s12937-015-0121-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Dehghan M, Al Hamad N, Yusufali A, Nusrath F, Yusuf S, Merchant AT. Development of a semi-quantitative food frequency questionnaire for use in United Arab Emirates and Kuwait based on local foods. Nutr J. 2005;4:18. doi: 10.1186/1475-2891-4-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Cambridge UO. The EPIC-Norfolk Food Frequency Questionnaire and FETA Software. 2014. [cited d2016 May 27]. Available from: http://www.srl.cam.ac.uk/epic/epicffq/
- 24.Ocke MC, Bueno-de-Mesquita HB, Pols MA, Smit HA, van Staveren WA, Kromhout D. The Dutch EPIC food frequency questionnaire. II. Relative validity and reproducibility for nutrients. Int J Epidemiol. 1997;26:S49–S58. doi: 10.1093/ije/26.suppl_1.s49. [DOI] [PubMed] [Google Scholar]
- 25.Marks GC, Hughes MC, van der Pols JC. The effect of personal characteristics on the validity of nutrient intake estimates using a food-frequency questionnaire. Public Health Nutr. 2006;9:394–402. doi: 10.1079/phn2006839. [DOI] [PubMed] [Google Scholar]
- 26.Yang YJ, Kim MK, Hwang SH, Ahn Y, Shim JE, Kim DH. Relative validities of 3-day food records and the food frequency questionnaire. Nutr Res Pract. 2010;4:142–148. doi: 10.4162/nrp.2010.4.2.142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Brunner E, Stallone D, Juneja M, Bingham S, Marmot M. Dietary assessment in Whitehall II: comparison of 7 d diet diary and food-frequency questionnaire and validity against biomarkers. Br J Nutr. 2001;86:405–414. doi: 10.1079/bjn2001414. [DOI] [PubMed] [Google Scholar]
- 28.Dahl AK, Hassing LB, Fransson EI, Pedersen NL. Agreement between self-reported and measured height, weight and body mass index in old age—a longitudinal study with 20 years of follow-up. Age and Ageing. 2010;39:445–451. doi: 10.1093/ageing/afq038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Yoong SL, Carey ML, D’Este C, Sanson-Fisher RW. Agreement between self-reported and measured weight and height collected in general practice patients: a prospective study. BMC Med Res Methodol. 2013;13:38. doi: 10.1186/1471-2288-13-38. [DOI] [PMC free article] [PubMed] [Google Scholar]