

Abstract
Intraparenchymal leiomyoma of the breast are among benign non-epithelial tumors with the lowest incidence. Although it displays a benign histology, it may be confused with malignant lesions and create diagnostic confusion. In this paper, we report a 44-year-old woman with a painless mass with a diameter of 1.5 cm in the upper medial quadrant of her right breast. The lesion was removed surgically. The lesion’s histologic examination and immunohistochemical analysis revealed a smooth muscle tumor of the breast. The patient was initially diagnosed with fibroadenoma and was followed in terms of the epicenter for six months before she underwent surgery. Her mammography and histopathology results are discussed in this report.
Keywords: Breast neoplasm, diagnosis, leiomyoma
Introduction
Leiomyoma is a non-malignant tumor of smooth muscle origin, which is an important member of mesenchymal neoplasms involving the gastrointestinal tract and uterus. Leiomyoma of the breast is an extremely rare stromal tumor, constituting less than 1% of all breast neoplasms (1). It most commonly involves the subareolar area of the breast and occurs in both sexes (2). Herein, we report a 44-year-old woman with leiomyoma of the breast and provide the lesion’s immunohistochemical and histological properties along with a discussion of the relevant literature.
Case Presentation
A 44-year-old woman was admitted with a history of a painless lump growing in her right breast for six months. She experienced neither nipple discharge nor morphological changes of the areola and nipple. She was not lactating or taking hormone therapy, either. Her family history of breast cancer was negative. On physical examination, she had a mobile, well-circumscribed mass lesion measuring 1.5×1 cm localized to the upper medial quadrant (UMQ) of the right breast, 7 cm away from the nipple. The mass had no attachment to the overlying skin and lacked any signs of inflammation. There was no axillary or supraclavicular lymph node involvement, nor was there any abnormality of the contralateral breast and axillary region.
A mammogram revealed a dense, oval, non-calcified lesion in the corresponding region (Figure 1), but no other lesions. There appeared no axillary lymphadenopathy. The final classification of the mass was considered to be in BIRADS category 4A. The clinical and mammographic findings prompted an excisional biopsy collected from the lesion. The gross examination of the mass revealed a fleshy, pale whitish tissue; the histological study of the lesion showed that it contained spindle cells forming bundles in an intermingling fashion. The microscopic examination demonstrated spindle cells without atypia, which were arranged in fascicles. There were also no necrosis, mitotic activity, or vascular invasion (Figure 2a–d). Immunohistochemical study indicated diffuse, intense staining for smooth muscle actin (SMA) (Figure 2c) and desmin (Figure 2d). Based on the results, intraparenchymal leiomyoma of the breast was diagnosed. An informed consent was obtained from the patient for the publication of this manuscript.
Figure 1.
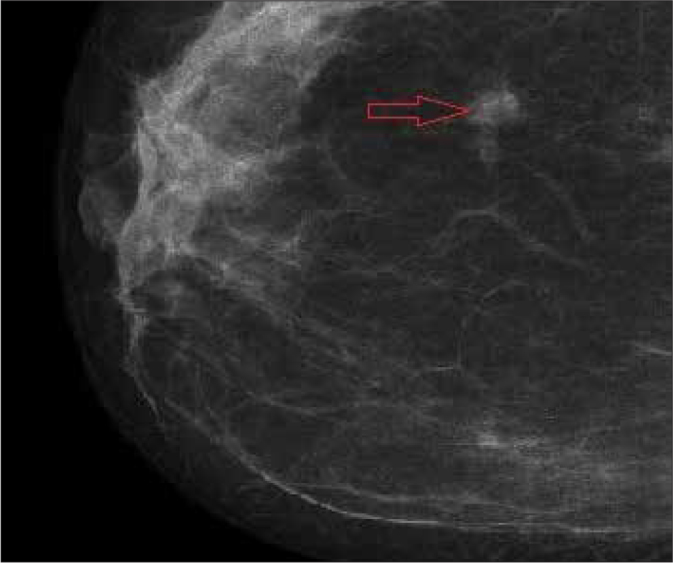
Craniocaudal mammografic view of the right breast, which shows a dense, oval mass (red arrow)
Figure 2. a–d.

Microscopic view of sections of surgical specimen; positive reaction in smooth muscle cells in immunohistochemical examination (H&E:10×, H&E:5×, SMA: 20×, Desmin:20×)
Discussion and Conclusion
Leiomyomas are extremely uncommon (1). The first description of a leiomyoma of the breast parenchyma was done by Strong LW in 1913 (3). When it involves the breast tissue, it usually occurs in the subareolar area. There are multiple theories as to the origin of these tumors. Kaufman and Hirsch (4) advocated that they originate from the myocytes around the capillaries in the subcutaneous tissue of the mammary gland. According to Diaz-Arias et al. (5), there may be five alternatives: teratoid origin coupled with significant overgrowth of the myomatous elements, smooth muscle cells that migrate from the nipple during embryological life, a multipotent mesenchymal cell, angiomatous smooth muscle and myoepithelial cells. Although the common location of this tumor around the nipple suggests a relationship with a high amount of smooth muscle cells in these regions, the histological evolution of these lesions remains obscure (6). Tumors of smooth muscle origin are rare in general and even rarer in the human breast. Their ratio is less than 1% among all breast tumors. They usually involve the right breast and are usually seen in women of 30–60 years of age with an average age of 47.5 years; consistent with this, our patient was 44 years old. Parenchymal leiomyomas have a well-defined border and usually measure 1.0–14.0 cm in diameter (7). As no definite radiological criteria exist for their identification, histopathological and immunohistochemical studies are necessary. The histopathological properties of all leiomyomas are the same irrespective of the involved organ. The cells of this tumor have an eosinophilic cytoplasm and form intermingling bundles. They are stained positively for vimentin, desmin and SMA (5). h-Caldesmon (h-CD) is a protein combined with actin and tropomyosin that regulates cellular contraction. h-CD has been thought to be expressed exclusively in vascular and visceral smooth muscle cells (SMC). h-CD is also a specific marker of both SMC and its neoplasms and that immunohistochemical detection of h-CD may facilitate the differential diagnosis between leiomyosarcomas and other tumors with SMClike differentiation, including myofibroblastic tumors (8).
This tumor’s differential diagnoses include adenomyoepithelioma, phyllodes tumor, adenoleiomyoma, fibroadenoma with prominent smooth muscle, fibromatosis, benign spindle cell tumor of the breast, fibrous histiocytoma, myoid hamartoma, myoepithelioma, fibromatosis-like low-grade metaplastic carcinoma and leiomyosarcoma of the breast (9).
Among these, the most important one is leiomyosarcoma, which shows similar properties with leiomyomas in that it appears as a dense, well-demarcated non-invasive lesion on mammography and arises many years before being diagnosed. The distinction between the two is important since leiomyosarcomas may show local recurrence or distant metastasis by hematogenous route long after excision. These tumors also feature marked cellular atypia, high grade of mitosis (2–16 mitotic figures per 10 high-power fields), atypical mitoses, vascular invasion, and necrosis (10). Son et al. (11) reported an increase in the prevalence of leiomyomas of breast with tamoxifen use. A similar potential association was also reported for antiobesity drugs sibutramine and orlistat (6). These tumors are best treated with simple excision, and extensive surgery is not justified given the benign nature of these lesions. No evidence yet has been reported as to any potential of the tumor for malignant transformation or distant spread (9).
In conclusion, intraparenchimal leiomyoma of the breast is quite rare, but it can mimic other lesions of the mammary gland, both clinically and radiologically. Malignant and benign lesions cannot be reliably distinguished using physical examination or imaging studies. Hence, simple excision followed by a careful histological evaluation is necessary for a definitive diagnosis.
Footnotes
Informed Consent: Informed consent was obtained from patient who participated in this study.
Peer-review: Externally peer-reviewed.
Conflict of Interest: No conflict of interest was declared by the authors.
Author Contributions: Concept - M.T.K., M.Y., T.S.Y.; Design - M.T.K., A.A., T.S.Y., A.I.A.; Supervision - M.T.K., M.A.G., T.S.Y.; Funding - M.T.K., M.Y., M.A.G.; Materials - M.T.K., M.Y., M.A.G., A.I.A.; Data Collection and/or Processing - M.T.K., A.A., A.I.A.; Analysis and/or Interpretation - M.T.K., M.Y., M.A.G., A.A.; Literature Review - M.T.K., M.Y., M.A.G.; Writer - M.T.K.; Critical Review - M.T.K., T.S.Y.
Financial Disclosure: The authors declared that this study has received no financial support.
References
- 1.Sidoni A, Lüthy L, Bellezza G, Consiglio MA, Bucciarelli E. Leiomyoma of the breast: case report and review of the literature. Breast. 1999;8:289–290. doi: 10.1054/brst.1999.0061. https://doi.org/10.1054/brst.1999.0061. [DOI] [PubMed] [Google Scholar]
- 2.Ende L, Mercado C, Axelrod D, Darvishian F, Levine P, Cangiarella J. Intraparenchymal leiomyoma of the breast: a case report and review of the literature. Ann Clin Lab Sci. 2007;37:268–273. [PubMed] [Google Scholar]
- 3.Shah SD, Gupta A, Roy S, Mukhopadhyay S. Intraparenchymal leiomyoma of the breast: a case report. Indian J Surg. 2013;75:88–9. doi: 10.1007/s12262-011-0367-6. https://doi.org/10.1007/s12262-011-0367-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kaufman HL, Hirsch EF. Leiomyoma of the breast. J Surg Oncol. 1996;62:62–64. doi: 10.1002/(SICI)1096-9098(199605)62:1<62::AID-JSO13>3.0.CO;2-V. https://doi.org/10.1002/(SICI)1096-9098(199605)62:1<62::AID-JSO13>3.0.CO;2-V. [DOI] [PubMed] [Google Scholar]
- 5.Diaz-Arias AA, Hurt MA, Loy TS, Seeger RM, Bickel JT. Leiomyoma of the breast. Hum Pathol. 1989;20:396–399. doi: 10.1016/0046-8177(89)90052-x. https://doi.org/10.1016/0046-8177(89)90052-X. [DOI] [PubMed] [Google Scholar]
- 6.Pourbagher A, Pourbagher MA, Bal N, Oguzkurt L, Ezer A. Leiomyoma of the breast parenchyma. ACR. 2015;185:1595–1597. doi: 10.2214/AJR.04.1453. [DOI] [PubMed] [Google Scholar]
- 7.Vecchio GM, Cavaliere A, Cartaginese F, Lucaccioni A, Lombardi T, Parenti R, Salvatorelli L, Magro G. Intraparenchymal leiomyoma of the breast: report of a case with emphasis on needle core biopsy-based diagnosis. Pathologica. 2013;105:122–127. [PubMed] [Google Scholar]
- 8.Watanabe K, Kusakabe T, Hoshi N, Saito A, Suzuki T. h-Caldesmon in leiomyosarcoma and tumors with smooth muscle cell–like differentiation: its specific expression in the smooth muscle cell tumor. Hum Pathol. 1999;30:392–396. doi: 10.1016/s0046-8177(99)90113-2. https://doi.org/10.1016/S0046-8177(99)90113-2. [DOI] [PubMed] [Google Scholar]
- 9.Granic M, Stefanovic-Radovic M, Zdravkovic D, Ivanovic N, Nikolic D, Radovanovic D, Stojiljkovic M. Intraparenchimal leiomyoma of the breast. Arch Iran Med. 2015;18:608–612. [PubMed] [Google Scholar]
- 10.Stafyla VK, Gauvin JM, Farley DR. A 53–year– old woman with a leiomyosarcoma of the breast. Curr Surg. 2004;61:572–575. doi: 10.1016/j.cursur.2004.05.008. https://doi.org/10.1016/j.cursur.2004.05.008. [DOI] [PubMed] [Google Scholar]
- 11.Son EJ, Oh KK, Kim EK, Son HJ, Jung WH, Lee HD. Leiomyoma of the breast in a 50-year-old woman receiving tamoxifen. Am J Roentgenol. 1998;171:1684–1686. doi: 10.2214/ajr.171.6.9843313. https://doi.org/10.2214/ajr.171.6.9843313. [DOI] [PubMed] [Google Scholar]