

Abstract
Background:
Most patients experience some degree of pain during extracorporeal shock waves lithotripsy (ESWL).
Aim:
The aim of this study was to evaluate the effect of target-controlled infusion (TCI) of remifentanil or sufentanil and patient-controlled analgesia (PCA) with sufentanil or morphine for pain relief during ESWL.
Materials and Methods:
In a double blind, randomized clinical trial, a total of 60 patients who were scheduled for elective ESWL, randomly assigned into four groups (A, B, C and D). Patients in group A and B received remifentanil and sufentanil with TCI, respectively. Also, patients in group C and D received sufentanil and morphine with PCA, respectively. All patients in four groups were assessed about the intensity of their pain with Visual Analogue Scale (VAS) in three phases; the discharge of the waves (phase A), during breaking the stones (phase B) and the end of the procedure (phase C).
Results:
Patients in morphine PCA group experienced highest pain intensity in all stages, but patients in remifentanil TCI group experienced lowest pain intensity during lithotripsy. Remifentanil/TCI group experienced the lowest pain in B and C phases and the sufentanil/TCI group had the lowest pain only in the phase A. There was no significant difference in the occurrence of complications in all four groups.
Conclusion:
The current study demonstrates that efficacy of TCI pump in the reduction of pain during ESWL is superior to the PCA pump. Among the drugs that used in this study, remifentanil has more effective in pain management in the all phases during ESWL. We believe that using remifentanil/TCI should strongly be considered to clinicians in ESWL units.
Keywords: Lithotripsy, Pain, Analgesia, Patient-Controlled, Remifentanil, ESWL
1. INTRODUCTION
Extracorporeal shock waves lithotripsy (ESWL) is a common method for treatment of the urinary tract stones with high efficacy and fewer complications than other invasive procedures (1). Most patients experience some degree of pain during this procedure (2, 3). Inadequate pain control during this procedure is associated with an increased risk of complications, reducing the efficiency of the treatment, patients’ dissatisfaction, longer hospital stay and increasing costs (4). Many drugs and methods such as local, intravenous (IV) or oral non-steroidal anti-inflammatory drugs (NSAIDs) and/or opioid agents have been used for pain management during ESWL (2). Nonetheless, the most effective analgesic regimen during ESWL has not been determined (2, 3). Among the drugs that were used for analgesia during ESWL, opioids seem to be a favorable analgesic; however the opioid administration may be problematic especially at high doses in an outpatient setting, due to a longer recovery time and side effects like nausea, hypotension respiratory depression and vomiting. Therefore different techniques have been used for decreasing the dosage of opioids during ESWL (4). The common method of delivering opioids to the patients is the administration of the drug as a bolus and repeated doses, which can lead to delivering a large dose of the drug to the patient, with higher incidence of side effects (5, 6).
An alternative to this method is to use of infusion pumps such as patient-controlled analgesia (PCA) device, with administering a bolus on demand, and low dose infusion plus bolus. It has been shown that PCA is superior to the bolus-only technique (7, 8). Also, the successful use of target-controlled infusion (TCI) device for pain management in ESWL has been reported. It has been shown that the delivery of opioids with TCI pump is associated with high tolerance of the patient to the pain and high successful rate of ESWL (9, 10). TCI utilizes a computer-controlled infusion pump to deliver a drug according to a pharmacokinetic model which takes into account the patient’s age and weight, balancing rates of infusion, distribution, and elimination to achieve a ‘‘target’’ blood concentration of the drug (2). An important point in ESWL is that the success rate of this procedure highly depends on the degree of the pain relief during the ESWL. Therefore, so many drugs and techniques with high efficacy and fewer side effects and rapid recovery rate were trying to use by clinicians. In some studies, using medication delivery device was associated with more efficiency and fewer side effects compared to the single dose injection or infusion methods (9-12), But due to the limited number of these studies, as well as compare a single dose injection method with only one drug delivery system techniques (9, 11-12), or comparing two different drug delivery systems with only one drug (10, 13). In the present study, we decided to compare two techniques of drug delivery systems (TCI/PCA) with the use of different opioids to determine which drug/technique has the maximum efficiency and the lowest side effects.
2. MATERIAL AND METHODS
After obtaining approval from the Institutional Ethics Committee, a total of 60 consecutive patients who were scheduled for elective ESWL treatment of kidney stones, were considered for this prospective, double-blind randomized clinical study. Patients with Class I or II of American Society of Anesthesiologists (ASA class), aged 18-60 years, of both sexes, who had a single renal stone, less than 1.5 cm, and first time to do ESWL procedure, were enrolled in the study.
Patients with history of chronic use of any analgesics or α2-agonists, calculi outside the renal pelvis, pregnancy, known allergy to the drugs used in the study, inability to understand and use the visual analog scale (VAS) as well as patient-controlled analgesia (PCA) device and occurrence of any complication during the procedure were excluded from the study. Also, patients with known allergy to any medications used in the study were excluded. This study was conducted in ESWL unit of the Imam Reza hospital, a teaching hospital affiliated to Kermanshah University of Medical Sciences, Kermanshah, Iran, between December 2013 and September 2014. This study registered in the Iranian Registry of Clinical Trials Database (IRCT201012041310N5).
Patients who fulfilled the inclusion criteria, after obtaining the informed written consent, were randomly allocated into four equally sized groups of A, B, C and D, (n=15 in each group) by a nurse anesthesia who was blind to the study groups, using sealed envelope technique and computer generated random numbers.
Patients in group A and B received sufentanil and remifentanil with TCI device, respectively. When the device switched on, the operator enters proposed patient age, weight and gender, and device calculate the blood concentration of the drug needed for the target effect. In group C and D all patients were connected to a PCA pump prior to the start of the procedure. Patients in group C, received sufentanil with 0.1µg/kg primary loading dose and background infusion rate of 0.2µg/kg /h with 20 minutes locked out interval and in group D, morphine started with a loading dose of 0.05mg/kg and background infusion rate of 1mg/h with 20 minutes locked out interval.
Patients in group C and D were instructed to use the PCA device. Also all patients were instructed to rating the intensity of their pain using the VAS (where 0 denotes to the least and 10 to the worst imaginable intensity), during procedure. After routine preoperative evaluation, patients were positioned on the lithotripsy table and baseline measurement of blood pressure (BP), heart rate (HR), electrocardiogram, oxygen saturation (SPO2) and respiratory rate (RR) were obtained. The patient was inspired with 2 L/min flow rate oxygen through a nasal cannula. Patients’ RR, HR, SPO2 and BP were recorded continuously every 5 minutes with automatic device throughout the procedure. After imaging and localization the stone, ESWL treatment was commenced. Shock waves generator voltage was started at 14 Kilovolts (kV) and rapidly increased in 2 KV increments every 500 shocks to a maximum voltage of 24 KV. VAS score was recorded in three phases of the procedure by an anesthesiology resident who was blinded to the study. Phase A, was during the discharge of waves, phase B was during the breaking of stones, and phase C was at the end of procedure. All procedures were applied by the same urologist using a third-generation lithotriptor (Dornier, Compact Sigma, Germany). The duration of the procedure was recorded for each patient that was 45 minutes averagely. Additionally, patients’ demographic characteristics including age, gender, level of shock wave energy and duration of ESWL were collected.
The primary outcome of the present study was comparison of changes in pain intensity scores at three phases between the groups. The secondary outcome was comparison of incidence of any side effects between groups.
Statistical analysis
We used the Shapiro-Wilk test to test whether data were normally distributed. Descriptive baseline characteristics for 4 group’s comparisons were tabulated as mean ± SD, or as number and percentages. Comparing between 4 groups for categorical data were statistically analyzed using chi-square or Fisher-exact test and for continuous data were statistically analyzed using Analysis of variance (ANOVA) and Kruskal–Wallis test. Using General Linear Model (GLM) score of VAS between two groups were compared by repeated measurement ANOVA test. A p value of 0.05 or less was considered statistically significant. Data were analyzed using IBM SPSS statistics version 16.
3. RESULTS
A total of 71 patients were screened during the study. Of these, 7 patients did not meet the inclusion criteria and 4 patients declined to participate in the study. Remaining 60 patients randomly allocated to the four groups. Four patients losses to follow-up during the study. In total, 56 patients completed the study and data from all these patients were analyzed (Figure 1).
Figure 1.
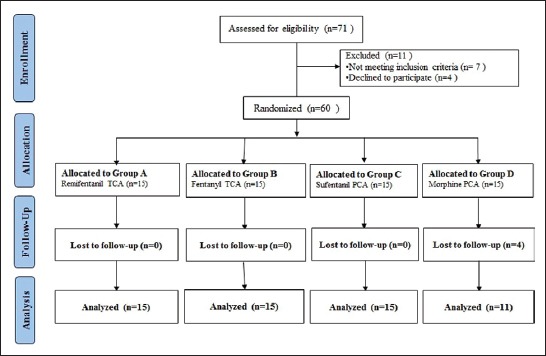
Flow chart of the study
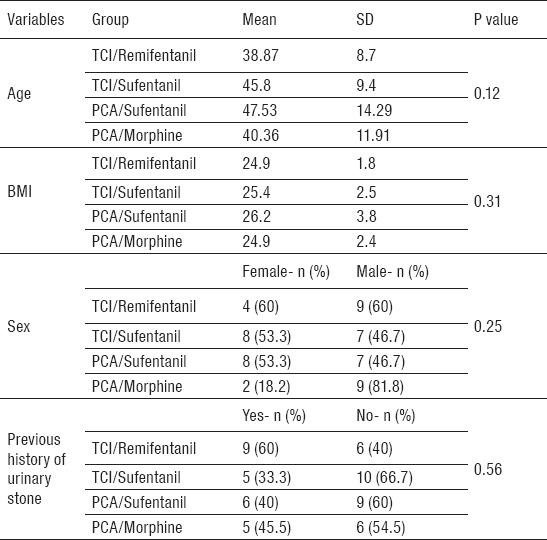
Basic demographic and clinical characteristics of patients in 4 groups are presented in Table 1. As shown in Table 1, there are no statistically significant differences between groups.
Table 1.
Basic demographic and clinical characteristics of patients in the four groups
Trend in pain intensity score changes
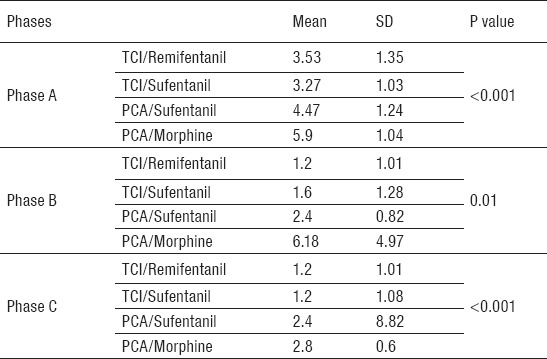
Pain intensity was measured in four groups in three phases. The results showed that the intensity of experienced pain was different in all groups in all phases. Patients in PCA/morphine group experienced the highest intensity of pain in all phases during procedure. Patients in TCI/sufentanil group experienced the lowest intensity of pain in phase A (discharge the waves). Patients in TCI/remifentanil group experienced lowest pain in phase B (breaking the stone). Patients in TCI/remifentanil and TCI/sufentanil groups experienced minimum pain and patients in PCA/morphine experienced maximum pain during phase C (end of the procedure). These differences were statistically significant (Table 2)
Table 2.
Changes of trend in pain intensity score (according to VAS) during 3 phases. Phase A: during discharge of the waves; Phase B: during breaking the stones; Phase C: at the end of the procedure
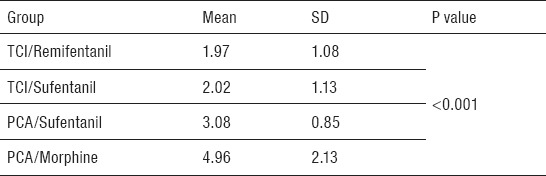
Without considering the phases of the study, the results showed that the patients in TCI/remifentanil group experienced lower pain intensity during the procedure (Table 3).
Table 3.
Changes of trend in pain intensity score (according to VAS) regardless of the phases of study
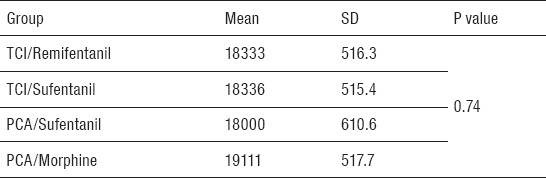
There was no significant statistical difference between the groups in terms of the amount of the voltage that used during the procedure (Table 4).
Table 4.
The amount of voltage used in 4 groups during the procedure (Volt)
Side effects
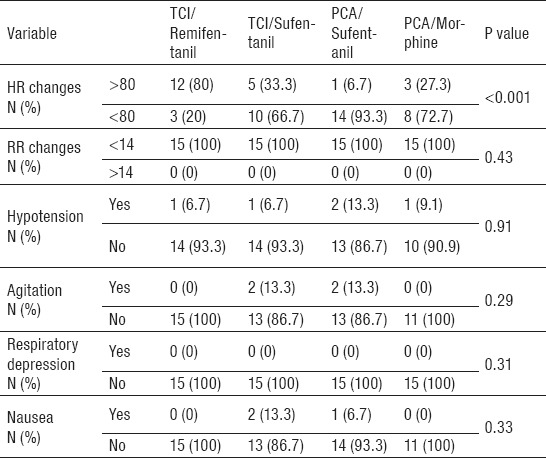
Side effects of opioids such as agitation, respiratory depression, hypotension, nausea and HR changes were evaluated in 4 study groups. There were no statistically significant differences between study groups (Table 5).
Table 5.
Frequency of side effects in four study groups
4. DISCUSSION
During ESWL, the amount of voltage used for the breaking of the stones has a direct relationship with the success rate of technique. Delivering the enough voltage to perform a successful fragmentation of the stones depends on the degree of the patient’s pain relief during the procedure. Providing enough depth of analgesia allows the urologists to deliver higher voltage energy for breaking the stones without any motion of the patient during the procedure. Due to the high intensity of pain that is applied by the first generation of lithotripters, ESWL required general or spinal-epidural anesthesia, but with the use of the new generation of the lithotripters that needs low energy for lithotripsy, we can use the topical and local methods such as oral medications and infiltration of local anesthetics and intravenous administration of sedative drugs for stone breaking. Therefore, ESWL has become an outpatient procedure (7, 8).
In this study we compared two drug delivery techniques, PCI and TCI, with three different drugs to identify the amount of analgesia and side effects of each technique, to determine the best drug/technique between these two methods and four drugs. Because there is a small lag time between feeling of the pain and delivering the drugs with PCA pump and use of background infusion to deliver drugs with PCA, it can provide constant drug concentration in the effect site of the drug. Using PCA pump is superior to the use of single dose administration of opioids with the lowest side effects such as respiratory depression. The shorter lag time between the feeling of pain and drug delivery provide a large degree of pain relief and patient satisfaction. The only disadvantage of the PCA pump is the high cost of this method. Although using this method reduces the dosage of drugs need for pain control and resulting in a reduction of side effects of this treatment, finally reduce the overall costs. In studies conducted by the Chin and Tokumine, using PCA pump was suggested during breaking of urinary stones with ESWL (9, 12).
In the present study, the intensity of pain was determined in three phases, A, B, and C. Phase A was during the discharge of waves, phase B was during breaking the stones and phase C was at end of the procedure. According to the VAS score, patients in the TCI group experienced lower pain, in comparison with the PCA group in three phases of the study. Using TCI pump reduce individual differences in pharmacokinetics of drugs, the drugs reach earlier to a therapeutic level and fix concentration in site effect that is one of the reasons that make TCI method preference to PCA method. Among the opioids that were used in the present study, TCI/sufentanil was more effective than TCI/remifentanil in phase A of the study. One possible explanation for this may be the higher potency of sufentanil compared with remifentanil (14) which make this opioid superior to other opioids to eliminate pain in phase A in this study. But at the phase B of the study TCI/remifentanil was more effective than TCI/sufentanil because at this time sufentanil start to metabolize and distribute to the peripheral tissues, but at the same time remifentanil started to act in the effect site. In C phase, due to reducing the severity of pain at the end of the procedure sufentanil and remifentanil has the same effect on pain perception.
In the study by Cortinez et al. that remifentanil, and fentanyl used in TCI pump, has been shown that TCI/remifentanil has more effective than TCI/fentanyl for pain control (10). Unlike the equal potency of remifentanil and fentanyl, different pharmacokinetic properties of remifentanil can cause this result.
In the present study, morphine has lower efficacy in pain control during all three phases of ESWL. Morphine is an available and inexpensive analgesic but it seems that the long onset time of morphine to reach its peak effect is one of the causes of inadequate pain relief during ESWL. One of the serious complications of opioid usage is respiratory depression that manifests with hypoxia and hypercarbia (15, 16). To reduce this complication, in all patients we used supplementary oxygen with nasal cannula during the procedure. During this study, we did not observe any respiratory depression with all types of drugs/techniques, but in Cortinez et al. study, this complication observed in TCI/fentanyl more than TCI/remifentanil (10).
Beloeil et al. compared sufentanil and remifentanil for respiratory depression but no difference was observed in terms of respiratory depression between two drugs (17). Remifentanil reach immediately to site effect, but there is no enough time to compensating PACO2 rising. The sensitivity of µ receptors and fentanyl-induced muscle rigidity are other possible causes of respiratory depression caused by fentanyl. With reducing the speed of injection, we can provide enough time to compensate hypercarbia, by increasing the time for reaching opioids to the effect site (14). Another side effect of opioids is nausea and vomiting (18). In the present study there are no differences in the incidence of postoperative nausea and vomiting in all groups. To reduce this complication during the study, patients were kept NPO, and do not have any oral feeding up to 15 minutes after the procedure. In the Cortinez study, higher nausea and vomiting observed with fentanyl compared with remifentanil (10).
A limitation of the present study was the relatively small number of patients in the study groups. Therefore, further studies with larger sample size will be suggested to evaluate the efficacy and safety of these techniques and drugs.
5. CONCLUSION
The current study demonstrated that efficacy of TCI pump in the reduction of pain intensity during ESWL compared with the PCA pump. Also, among the drugs that used in this study, remifentanil had more efficacies in all phases of ESWL than other drugs. We believe that using TCI/remifentanil should strongly be considered by clinicians in ESWL units for pain management during this procedure.
Footnotes
•Conflicts of interest: All authors declare no conflict of interest; no conflict of interest exists for any of the authors associated with the manuscript. The funding organization had no role in the design and conduct of the study, or in the collection, analysis, and interpretation of the data.
•Author’s contributions: Study conception and design: AF and AS. Acquisition of data: AF. Statistical analysis and interpretation of data: AF and AS. Drafting of the manuscript: AF and AS. Critical revision of the manuscript for important intellectual content: AF and AS.
•Clinical trial registration number: IRCT201012041310N5
REFERENCES
- 1.Yesil S, Polat F, Ozturk U, Dede O, Imamoglu M, Bozkirli I. Effect of Different Analgesics on Pain Relief During Extracorporeal Shock Wave Lithotripsy. Hippokratia. 2014;18(2):107. [PMC free article] [PubMed] [Google Scholar]
- 2.Yardy G, Shah N, Wiseman O. Analgesia for shock wave lithotripsy. Br J Med Surg Urol. 2010;3(5):198–203. [Google Scholar]
- 3.Monk TG, Ding Y, White PF, Albala DM, Clayman RV. Effect of topical eutectic mixture of local anesthetics on pain response and analgesic requirement during lithotripsy procedures. Anesth Analg. 1994;79(3):506–11. doi: 10.1213/00000539-199409000-00018. [DOI] [PubMed] [Google Scholar]
- 4.Ozsaker E, Diramali A. The effect of transcutaneous electrical nerve stimulation for pain relief during extracorporeal shock-wave lithotripsy procedure. Pain Manag Nurs. 2014;15(1):59–68. doi: 10.1016/j.pmn.2012.06.003. [DOI] [PubMed] [Google Scholar]
- 5.Bach C, Zaman F, Kachrilas S, Kumar P, Buchholz N, Masood J. Drugs for pain management in shock wave lithotripsy. Pain Res Treat. 2011;2011:259426. doi: 10.1155/2011/259426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hosseininejad SM, Emami Zeydi A. Can intracutaneous sterile water injection be used as a possible treatment for acute renal colic pain in the emergency department? A short literature review. Urol Ann. 2015;7(1):130–2. doi: 10.4103/0974-7796.148669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Aboumarzouk OM, Hasan R, Tasleem A, Mariappan M, Hutton R, Fitzpatrick J, et al. Analgesia for patients undergoing shockwave lithotripsy for urinary stones - a systematic review and meta-analysis. Int Braz J Urol. 2017:43. doi: 10.1590/S1677-5538.IBJU.2016.0078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gupta NP, Kumar A. Analgesia for pain control during extracorporeal shock wave lithotripsy: Current status. Indian J Urol. 2008;24(2):155–8. doi: 10.4103/0970-1591.40607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chin C, Tay K, Ng F, Lim P, Chng H. Use of patient-controlled analgesia in extracorporeal shockwave lithotripsy. Br J Urol. 1997;79(6):848–51. doi: 10.1046/j.1464-410x.1997.00212.x. [DOI] [PubMed] [Google Scholar]
- 10.Cortinez L, Munoz H, De la Fuente R, Acuna D, Dagnino J. Target-controlled infusion of remifentanil or fentanyl during extra-corporeal shock-wave lithotripsy. Eur J Anaesthesiol. 2005;22(01):56–61. doi: 10.1017/s0265021505000128. [DOI] [PubMed] [Google Scholar]
- 11.Tokumine J, Iha H, Okuda Y, Shimabukuro T, Shimabukuro T, Ishigaki K, et al. Appropriate method of administration of propofol, fentanyl, and ketamine for patient-controlled sedation and analgesia during extracorporeal shock-wave lithotripsy. J Anesth. 2000;14(2):68–72. doi: 10.1007/s005400050069. [DOI] [PubMed] [Google Scholar]
- 12.Kortis HI, Amory DW, Wagner BK, Levin R, Wilson E, Levin A, et al. Use of patient-controlled analgesia with alfentanil for extracorporeal shock wave lithotripsy. J Clin Anesth. 1995;7(3):205–10. doi: 10.1016/0952-8180(95)00008-6. [DOI] [PubMed] [Google Scholar]
- 13.Irwin MG, Campbell RC, Lun TS, Yang JC. Patient maintained alfentanil target-controlled infusion for analgesia during extracorporeal shock wave lithotripsy. Can J Anaesth. 1996;43(9):919–24. doi: 10.1007/BF03011805. [DOI] [PubMed] [Google Scholar]
- 14.Lentschener C, Ghimouz A, Bonnichon P, Pépion C, Gomola A, Ozier Y. Remifentanil-propofol vs. sufentanil-propofol: optimal combinations in clinical anesthesia. Acta Anaesthesiol Scand. 2003;47(1):84–9. doi: 10.1034/j.1399-6576.2003.470115.x. [DOI] [PubMed] [Google Scholar]
- 15.Hasanzadeh Kiabi F, Soleimani A, Habibi MR, Emami Zeydi A. Can vitamin C be used as an adjuvant for managing postoperative pain? A short literature review. Korean J Pain. 2013;26(2):209–10. doi: 10.3344/kjp.2013.26.2.209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sharifi H, Firouzian A, Emami Zeydi A. Aromatherapy as a promising adjunctive treatment for acute renal colic pain: an issue that merits further research. Urolithiasis. 2017;45(2):231–2. doi: 10.1007/s00240-016-0917-2. [DOI] [PubMed] [Google Scholar]
- 17.Beloeil H, Corsia G, Coriat P, Riou B. Remifentanil compared with sufentanil during extra-corporeal shock wave lithotripsy with spontaneous ventilation: a double-blind, randomized study. Br J Anaesth. 2002;89(4):567–70. doi: 10.1093/bja/aef202. [DOI] [PubMed] [Google Scholar]
- 18.Firouzian A, Alipour A, Rashidian Dezfouli H, Zamani Kiasari A, Gholipour Baradari A, Emami Zeydi A, et al. Does lidocaine as an adjuvant to morphine improve pain relief in patients presenting to the ED with acute renal colic? A double-blind, randomized controlled trial. Am J Emerg Med. 2016;34(3):443–8. doi: 10.1016/j.ajem.2015.11.062. [DOI] [PubMed] [Google Scholar]