

Abstract
Introduction:
Bosnia and Herzegovina has one of the highest unemployment rates in the Balkan region (43.2%), so unemployment is one of the most serious public concerns in our country.
Aim:
To analyze the influence of unemployment on mental health of the working age population who attend primary care center.
Material and Methods:
The study was carried out in the municipality of Bosanska Krupa, which has the highest unemployment rate in the Federation of Bosnia and Herzegovina (56%), and included 510 randomly selected working age patients (aged 23-65 years). We used the General Health Questionnaire-28 (GHQ-28) to evaluate mental health of the working age population.
Results:
There were significantly more women than men (53.5% vs. 46.5%; p=0.02). The mean age of participants was 51.04±12.84 years. The experimental group included 318 (62.35%) unemployed working age participants: 160 (50.3%) had been unemployed for more than 5 years and had had no work experience, while 158 (49.7%) unemployed participants had had a previous work experience of more than five years. The control group included 192 (37.65%) employed working age participants. Unemployment had a significant influence on mental health of the working age population. The unemployed participants had a significantly poorer mental health compared to the employed (p=0.0003). A predictor of impaired mental health was a job loss. A significantly greater mental health impairment occured in the group of unemployed participants with previous work experience of more than five years compared to the unemployed participants who had had no work experience (p=0.001) and employed (p=0.000).
Conclusion:
Unemployment has a negative impact and leads to impaired mental health of the working age population in Bosnia and Herzegovina. A job loss has a predictive role. It indicates that social and health policies must be developed in order to improve well-being of the working age population.
Keywords: unemployment, mental health, working age population
1. INTRODUCTION
Job insecurity, job loss and lack of work opportunities have characterized the Bosnian labor market in the last two decades, making unemployment one of the most serious public concerns in our country. Bosnia and Herzegovina still has one of the highest unemployment rates in the Balkan region (43.2%). The unemployment rate in Bosnia and Herzegovina is three times higher than the European rate. Most of EU member states recorded a lower unemployment rate in 2015 compared to the previous years. The unemployment rates in states of the Balkan region showed a similar trend. In contrast, Bosnia and Herzegovina recorded a slight increase in the surveyed unemployment rate in 2015 compared to 2014 (27.5% vs. 27.7%) with 514.800 unemployed working age individuals (1). Current and past adverse situations (the 1992-95 war) in Bosnia and Herzegovina can have a lasting negative effect on mental health of people, often resulting in depression, anxiety, and somatization. These psychological disorders continue to be aggravated by economic instability in the country (2).
The consequences of unemployment are not only intra-personal, such as an impact on subjective well-being and common mental health problems. Unemployment also leads to inter-personal consequences, that is, the hidden and often overlooked social processes that affect unemployed people’s social well-being (3). The harmful effects of unemployment, especially long-term unemployment, on health are well documented. Numerous studies showed that the unemployed have poorer health than the employed (4-6). The available empirical evidences suggest that there is a negative correlation between long-term unemployment, health status and mortality risk (7). There is growing evidence of the deleterious effects on mental health of the current recession which started in 2008. Overall, the financial crisis in Europe seemed to have had heterogeneous effects on health outcomes, with the evidence being most consistent for suicides and mental health (8). Results of studies showed that unemployed individuals were more likely to have depressive symptoms (9), more stress (6) and lower well-being (5) compared to employed individuals. Unemployment was associated with an increased mortality risk for those in their early and middle careers, but less for those in their late career (10), but also with poor self-rated health (11), a significantly higher cardiovascular risk (12), and with a significant all-cause mortality risk (13). Unemployed people who comitted suicides were 10 times more likely to have had poor social support, and 16 times more likely to have had any stressful life events in the past 12 months compared to living unemployed controls (14). Long-term unemployed individuals have poorer physical and mental health in relation to people who are short-term unemployed. Long-term unemployment is related to elevated all-cause mortality and mortality risk increases with the duration of unemployment among men and women (15). Meta-analysis by Milner et al. suggests that long-term unemployment is associated with greater incidence of suicide. Risk is greatest in the first five years, and persists at a lower but elevated level up to 16 years after unemployment (16). The long-term unemployed carry a markedly higher burden of disease, particularly mental illness, than employed persons and those who have been unemployed only for a short time. The burden of disease increases with the duration of unemployment. Long-term unemployed have at least twofold risk of mental illness, particularly depression and anxiety disorders, compared to employed persons. Their mortality is 1.6-fold higher. Unemployment seems to be not only an effect of illness, but also its cause (17).
Relationship between unemployment and a consequent increase of mental health disorders is obvious in primary care settings where it often remains unrecognized in most cases. The aim of this study was to analyze the influence of unemployment on mental health of the working age population attending primary care setting.
2. MATERIAL AND METHODS
This cross-sectional study was carried out in the municipality of Bosanska Krupa, which has the highest unemoloyment rate in the Federation of Bosnia and Herzegovina (56%). The study included 510 randomly selected working age patients (aged 23-65 years) who attended the primary care center between July–December 2013. Exclusion criteria were: working age population younger than 23 and older than 65 years, established diagnosis of mental health disorders, cancer, neurological diseases (Parkinson’s disease, multiple sclerosis, stroke) and endocrine diseases (hyperthyreosis, hypothyreossis, hyper and hypofunction of suprarenal gland), or taking medications which can cause depression or anxiety (beta blockers, corticosteroids, ephedrin, aminophyllin, antihistamines, thyroid hormones, etc). The participants were divided into groups: 192 participants who were employed for more than 5 years (control group) and 318 unemployed participants (experimental group): 160 participants who had been unemployed for more than 5 years and had had no work experience and 158 unemployed participants with previous work experience of more than 5 years. The study was conducted in accordance with the code of ethics for this type of research (18).
To collect data about demographic characteristics and employment status of the participants (age, gender, duration of unemployment and previous work experience) we used the questionnaire created for this study. The General Health Questionnaire-28 (GHQ-28), translated into the Bosnian language, was used to evaluate mental health of the working age population (19). The reliability of GHQ-28 was tested by Cronbach alpha coefficient consistency and had satisfactory reliability equal to α=0.89 (Cronbach’s alpha). Developed as a screening tool to detect those likely to have or to be at risk of developing mental health disorders, the GHQ-28 is a 28-item measure of emotional distress in medical settings. The GHQ-28 has been divided into four subscales: somatic symptoms (items 1–7), anxiety/insomnia (items 8–14), social dysfunction (items 15–21), and severe depression (items 22–28). Each subscale consisted of seven questions with offered answers (1–not at all; 2–not more than usual; 3–some more than usual; 4–a lot more than usual). Evaluation of responses was provided according to the Likert scale. Scores by Likert scale were converted into binary values (0, 0, 1, 1) and the sum of scores was used to interpret severity of psychological distress. Total score (sum of four observed subscales) was used to determine mental health status which was considered as a dependent variable, while employment status was considered as an independent variable. Total score, which represented mental health status, varied between 28 and 112. The higher score indicated poorer mental health status of participants.
All data were analyzed using the statistical software package SPSS 20.0 (SPSS Inc., Chicago, IL, USA). We used standard tests of descriptive statistics. The chi-squared test with significance p<0.05 and independent samples t-test respectively were used for comparing proportions and arithmetic means between groups. To determine significance of arithmetic means differences between three or more groups we used univariate analysis of variance (ANOVA), and to test the impact of two or more variables to another variable we used Two Factor ANOVA. We expressed effect size as the difference between groups with a 95% confidence interval.
3. RESULTS
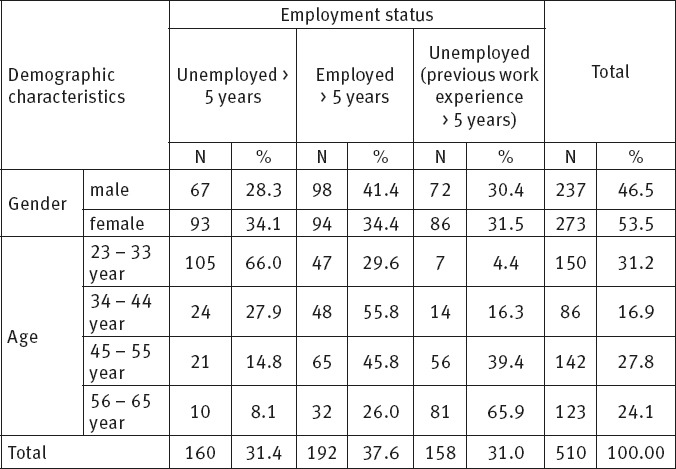
The study population comprised 510 randomly selected working age participants: 237 men and 273 women. There were significantly more women than men (53.5% vs. 46.5%; p=0.02). The mean age of participants was 51.04±12.84 years. The experimental group included 318 (62.35%) unemployed working age participants: 160 (50.3%) participants had been unemployed for more than 5 years and had had no work experience, and 158 (49.7%) unemployed participants who had had previous work experience of more than 5 years. The control group included 192 (37.65%) employed working age participants who had been employed for more than 5 years. Demographic characteristics of participants related to employment status are shown in Table 1.
Table 1.
Demographic characteristics of participants related to employment status
Unemployment was associated with worsening of mental health. The unemployed participants had poorer mental health status compared to the employed participants. The difference of mean mental health scores between unemployed and employed participants was statistically significant (52.64±13.38 vs. 48.43±10.97; t=3.65919; [95% CI: 1.852365-6.147635]; p=0.0003).
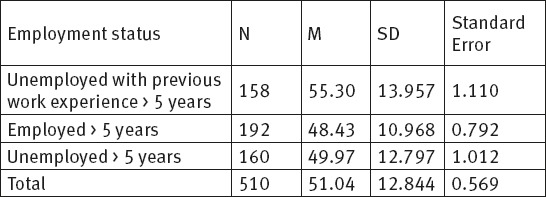
The unemployed participants with previous work experience had the highest mean mental health score for GHQ-28 (M=55.30), and consequently the highest impairment of mental health status. The employed participants had the lowest mean mental health score (M=48.43), while the unemployed participants with no work experience had the mean mental health score ranging between the values of the other two groups (M=49.97). The highest individual differences, measured by standard deviations, were observed in the group of unemployed participants with previous work experience (SD=13.957). The lowest individual differences were found in the employed participants group (SD=10.968) (Table 2).
Table 2.
Mean mental health score of participants related to employment status
The differences of the mean mental health status between groups of participants related to employment status were significant and can be generalized to the population represented by this sample (F=13.907; p=0.000). Data are shown in Table 3.
Table 3.
Significance of mean mental health scores differences between groups related to employment status
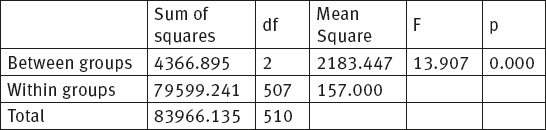
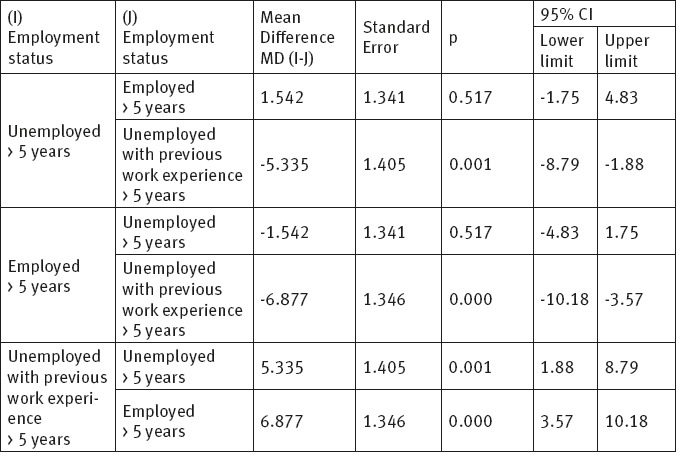
Table 4. shows significant differences of mean mental health status between: a) the group of unemployed participants with previous work experience and the group of employed participants (the mean difference was the highest: MD=-6.877; p=0.000); b) the group of unemployed participants with previous work experience and group of unemployed participants with no work experience (MD=-5.335; p=0001). It indicated that unemployed individuals with previous work experience of more than 5 years had the poorest mental health status compared to the other two groups. The difference of the mean mental health status between the group of unemployed participants with no work experience and the group of employed participants was the lowest (MD=-1.542) and was not significant (p=0.517). It indicated that a job loss had the predictive role for mental health impairment of the working age population.
Table 4.
Comparisons of mean differences of mental health scores between groups related to employment status
4. DISCUSSION
Economic recessions and crises have a negative impact on mental health. Global unemployment remains very high, particularly among developed economies, with the situation in Europe being the most challenging (20). Our findings indicate a different effect of the economic crisis on mental health according to employment status and show that unemployment has been associated with worsening of mental health of the working age population. We found that unemployment had a significant negative impact on mental health of the working age population. The unemployed working age participants had significantly poorer mental health compared to the employed participants. The participants who were unemployed with previous work experience of more than 5 years had the highest mean mental health score for GHQ-28 (M=55.30), and consequently the highest impairment of mental health status. The participants who had been employed for more than 5 years had the lowest mean mental health score (M=48.43). Similar to our results, Córdoba-Doña et al. concluded that current economic recession was associated with poorer mental health differentially according to labour market status (21). SESPAS report 2014 suggested that economic difficulties contributed to poorer mental health. The most important risk factor for this increase was unemployment (22). Our results showed that mental health status of unemployed participants with previous work experience of more than 5 years was significantly worsened compared to the unemployed with no work experience and employed participants. The difference of mean mental health status among unemployed with no work experience and employed participants can not be expected in the population. It indicated that a job loss had predictive role for mental health impairment of the working age population.
This research has confirmed a positive correlation between unemployment and poorer mental health of the working age population. Differences of mean mental health status between groups of participants related to employment status were significant and can be generalized to the population represented by this sample. Similar results were from cross-sectional study, carried out at the primary health care level in Australia, which showed that unemployed patients had a higher average score for GHQ-12 questionnaire in relation to the employed (3.8 vs. 2.4; p <0.001) (23). A study about health-related quality of life (HRQL) and economic downturns found that an increase in the average state unemployment rate worsened an individual’s HRQL (24). Most prospective studies, in which unemployment was assumed to cause health disorders, confirmed that job loss and long-term lack of salaries, especially for long periods of time, can result in a deterioration of mood and self-assessment of health with appearance of mental and somatic disorders in the initially healthy people. A preliminary analysis of unemployed population of Warsaw indicated that the unemployed perceived their health, physical and mental well-being as worse compared to the employed (25, 26).
5. CONCLUSION
Unemployment has a significant influence on mental health of the working age population in Bosnia and Herzegovina. Unemployed individuals have a markedly higher impairment of mental health than the employed. Job loss has a predictive role. Impaired mental health that occurs as a result of unemployment in working age population represents a serious challenge for public health and family medicine teams in Bosnia and Herzegovina. Results of this study suggest the need for generally available health care, rapid special health-promoting measures for unemployed patients and social interventions. With one of the highest unemployment rates in the Balkan region, Bosnia and Herzegovina must develop social and health policies in order to improve well-being of its population.
Footnotes
• Conflict of interest: The authors have no conflict of interest to declare.
REFERENCES
- 1.Council of ministers. Economic trends. Annual report 2015 [Internet] Sarajevo: Directorate for economic planning; 2016. Bosnia and Herzegovina. Available at: http://www.dep.gov.ba/dep_publikacije/ekonomski_trendovi/?id=1754 . [Google Scholar]
- 2.Broers T, Hodgetts G, Batic-Mujanovic O, Petrovic V, Hasanagic M, Godwin M. Prevalence of mental and social disorders in adults attending primary care centers in Bosnia and Herzegovina. Croat Med J. 2006 Un;47:478–84. [PMC free article] [PubMed] [Google Scholar]
- 3.Giuntoli G, Hughes S, Karban K, South J. Towards a middle-range theory of mental health and well-being effects of employment transitions: Findings from a qualitative study on unemployment during the 2009-2010 economic recession. Health (London) 2015;19(4):389–412. doi: 10.1177/1363459314554314. doi:10.1177/1363459314554314. [DOI] [PubMed] [Google Scholar]
- 4.Van Hal G. The true cost of the economic crisis on psychological well-being: a review. Psychol Res Behav Manag. 2015 Jan;8:17–25. doi: 10.2147/PRBM.S44732. doi:10.2147/PRBM.S44732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Oliffe JL, Han CS. Beyond workers’ compensation: men’s mental health in and out of work. Am J Mens Health. 2014 Jan;8(1):45–53. doi: 10.1177/1557988313490786. doi:10.1177/1557988313490 786. [DOI] [PubMed] [Google Scholar]
- 6.Pelzer B, Schaffrath S, Vernaleken I. Coping with unemployment: The impact of unemployment on mental health, personality, and social interaction skills. Work. 2014;48(2):289–95. doi: 10.3233/WOR-131626. doi:10.3233/WOR-131626. [DOI] [PubMed] [Google Scholar]
- 7.Minelli L, Pigini C, Chiavarini M, Bartolucci F. Employment status and perceived health condition: longitudinal data from Italy. BMC Public Health. 2014 Sep;14:946. doi: 10.1186/1471-2458-14-946. doi:10.1186/1471-2458-14-946. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Parmar D, Stavropoulou C, Ioannidis JP. Health outcomes during the 2008 financial crisis in Europe: systematic literature review. BMJ. 2016 Sep;354:4588. doi: 10.1136/bmj.i4588. doi:10.1136/bmj.i4588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kim SS, Muntaner C, Kim H, Jeon CY, Perry MJ. Gain of employment and depressive symptoms among previously unemployed workers: a longitudinal cohort study in South Korea. Am J Ind Med. 2013 Oct;56(10):1245–50. doi: 10.1002/ajim.22201. doi:10.1002/ajim. 22201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Roelfs DJ, Shor E, Davidson KW, Schwartz JE. Losing life and livelihood: a systematic review and meta-analysis of unemployment and all-cause mortality. Soc Sci Med. 2011 Mar;72(6):840–54. doi: 10.1016/j.socscimed.2011.01.005. doi:10.1016/j.socscimed.2011.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Giatti L, Barreto SM, César CC. Unemployment and self-rated health: neighborhood influence. Soc Sci Med. 2010 Aug;71(4):815–23. doi: 10.1016/j.socscimed.2010.05.021. doi:10.1016/j.socscimed.2010. 05.021. [DOI] [PubMed] [Google Scholar]
- 12.Noelke C, Avendano M. Who suffers during recessions? Economic downturns, job loss, and cardiovascular disease in older Americans. Am J Epidemiol. 2015 Nov;182(10):873–82. doi: 10.1093/aje/kwv094. doi:10.1093/aje/kwv094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Clemens T, Popham F, Boyle P. What is the effect of unemployment on all-cause mortality? A cohort study using propensity score matching. Eur J Public Health. 2015 Feb;25(1):115–21. doi: 10.1093/eurpub/cku136. doi:10.1093/eurpub/cku136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pompili M, Innamorati M, Di Vittorio C, Baratta S, Masotti V, Badaracco A, et al. Unemployment as a risk factor for completed suicide: a psychological autopsy study. Arch Suicide Res. 2014;18(2):181–92. doi: 10.1080/13811118.2013.803449. doi:10.1080/13811118.2013.803449. [DOI] [PubMed] [Google Scholar]
- 15.Garcy AM, Vågerö D. The length of unemployment predicts mortality, differently in men and women, and by cause of death: A six year mortality follow-up of the Swedish 1992–1996 recession. Soc Sci Med. 2012 Jun;74(12):1911–20. doi: 10.1016/j.socscimed.2012.01.034. doi:101016/j.socscimed.2012.01.034. [DOI] [PubMed] [Google Scholar]
- 16.Milner A, Page A, LaMontagne AD. Long-term unemployment and suicide: a systematic review and meta-analysis. PloS One. 2013 Jan;8(1):e51333. doi: 10.1371/journal.pone.0051333. doi:101371/journal.pone.0051333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Herbig B, Dragano N, Angerer P. Health in the long-term unemployed. Dtsch Arztebl Int. 2013 Jun;110(23-24):413–9. doi: 10.3238/arztebl.2013.0413. doi:10.3238/arztebl.2013.0413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.World Medical Association Declaration of Helsinki. Recommendations guiding physicians in biomedical research involving human subjects. Cardiovasc Res. 1997 Jul;35(1):2–3. doi: https://doi.org/10.1016/S0008-6363(97)00109-0. [PubMed] [Google Scholar]
- 19.Goldberg DP, Gater R, Sartorius N, Ustun TB, Piccinelli M, Gureje O, et al. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol Med. 1997 Jan;27(1):191–7. doi: 10.1017/s0033291796004242. [DOI] [PubMed] [Google Scholar]
- 20.United Nations. World economic situation and prospects 2013 [Internet] New York: United Nations; 2014. Available at: http://www.un.org/en/development/desa/policy/wesp/wesp_current/wesp2014.pdf . [Google Scholar]
- 21.Córdoba-Doña JA, Escolar-Pujolar A, San Sebastián M, Gustafsson PE. How are the employed and unemployed affected by the economic crisis in Spain? Educational inequalities, life conditions and mental health in a context of high unemployment. BMC Public Health. 2016 Mar;16:267. doi: 10.1186/s12889-016-2934-z. doi:10.1186/s12889-016-934-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gili M, García Campayo J, Roca M. Economic crisis and mental health SESPAS report 2014. Gac Sanit. 2014 Jun;28(Suppl 1):104–8. doi: 10.1016/j.gaceta.2014.02.005. doi:10.1016/j.gaceta.2014.02. 005. [DOI] [PubMed] [Google Scholar]
- 23.Comino EJ, Harris E, Chey T, Manicavasagar V, Penrose Wall J, Powell Davies G, et al. Relationship between mental health disorders and unemployment status in Australian adults. Aust N Z J Psychiatry. 2003 Apr;37(2):230–5. doi: 10.1046/j.1440-1614.2003.01127.x. [DOI] [PubMed] [Google Scholar]
- 24.Davalos ME, French MT. This recession is wearing me out!Health-related quality of life and economic downturns. J Ment Health Policy Econ. 2011 Jun;14(2):61–72. [PubMed] [Google Scholar]
- 25.Carlier BE, Schuring M, Lotters FJ, Bakker B, Borgers N, Burdorf A. The influence of re-employment on quality of life and self-rated health: a longitudinal study among unemployed persons in the Netherlands. BMC Public Health. 2013 May;13:503. doi: 10.1186/1471-2458-13-503. doi:10.1186/1471-2458-13-503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Supranowicz P. Occupational activity and health of Warsaw inhabitants. Part I. Unemployment: a preliminary analysis. Przegl Epidemiol. 2014;68(3):481–6. 583-6. [PubMed] [Google Scholar]