

Abstract
This document is an update to the 2011 Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2C9 and VKORC1 genotypes and warfarin dosing. Evidence from the published literature is presented for CYP2C9, VKORC1, CYP4F2, and rs12777823 genotype-guided warfarin dosing to achieve a target international normalized ratio of 2-3 when clinical genotype results are available. In addition, this updated guideline incorporates recommendations for adult and pediatric patients that are specific to continental ancestry.
Keywords: warfarin, pharmacogenetics, VKORC1, CYP2C9, CYP4F2, CYP2C, clinical implementation, pharmacogenomics
Introduction
Warfarin is a widely used anticoagulant with a narrow therapeutic index and large inter-patient variability in the dose required to achieve target anticoagulation. Common genetic variants in CYP2C9, VKORC1, CYP4F2 and the CYP2C cluster (e.g., rs12777823), plus known non-genetic factors, account for ∼50% of warfarin dose variability. This document is an update to the 2011 Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2C9 and VKORC1 genotypes and warfarin dosing and aims to assist in the interpretation and use of CYP2C9, VKORC1, CYP4F2, and rs12777823 genotypes to estimate therapeutic warfarin dose among patients with a target international normalized ratio (INR) of 2-3, should clinical genotype results be available to the clinician. The Clinical Pharmacogenetics Implementation Consortium (CPIC) of the National Institute of Health's Pharmacogenomics Research Network develops peer-reviewed gene/drug guidelines that are published and updated periodically on https://cpicpgx.org/genes-drugs/ and http://www.pharmgkb.org based upon new developments in the field (1). These guidelines were written with a global audience in mind, although the majority of the data that underpin these guidelines arise from people of European ancestry, East Asia and African Americans.
Focused Literature Review
The Supplement includes a systematic literature review on CYP2C9, VKORC1, CYP4F2 and other relevant genes/genotypes that have been associated with warfarin dosing. This systematic review forms the basis for the recommendations contained in this guideline. Although some of these genes have also been associated with dose of other coumarin anticoagulants, the recommendations below are specific to warfarin.
Drug: Warfarin
Warfarin (Coumadin® and others) is the most commonly used oral anticoagulant worldwide, with annual prescriptions in the Western world typically equaling 0.5 to 1.5% of the population (2). It is prescribed for treatment and prevention of thromboembolic disorders (3). Although highly efficacious, warfarin dosing is notoriously challenging due to its narrow therapeutic index and wide inter-individual variability in dose requirements even among patients with the same target INR (4). Complications from inappropriate warfarin dosing are among the most frequently reported adverse events to the U.S. Food and Drug Administration (FDA) and one of the most common reasons for emergency room visits (5).
Warfarin is usually dosed empirically: an initial dose is prescribed, typically followed by at least weekly measurement of the INR and subsequent dose adjustment. The initial dose is often based on population averages (e.g., 4-5 mg/day), but in some settings, it is common to use loading doses during the first few days of anticoagulation. Irrespective of the method used to initiate warfarin, stable doses to achieve an INR of 2-3 range from 1 to 20 mg/day. The iterative process to define the appropriate dose can take weeks to months and during this period, patients are at increased risk of over- or under-anticoagulation, and thus risk of bleeding or thromboembolism.
Warfarin pharmacology and pharmacokinetics
Figure 1 highlights key elements of warfarin pharmacology and pharmacokinetics. Warfarin inhibits vitamin K epoxide reductase complex (6) and is administered as a racemic mixture, with S-warfarin being more potent than R-warfarin (3).
Figure 1.
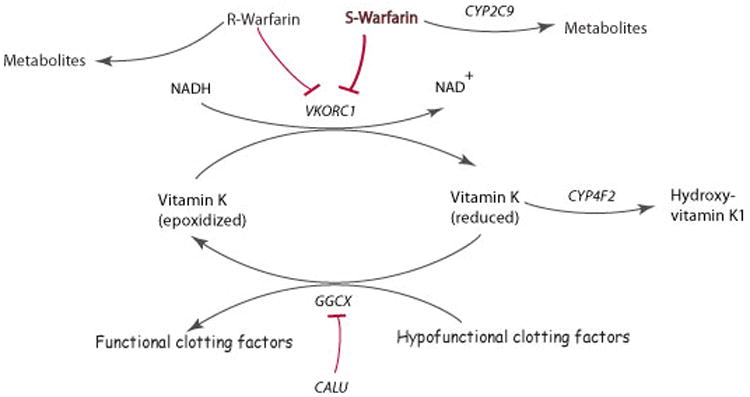
Schematic representation of warfarin metabolism and its mechanism of action.
Warfarin is administered via a racemic mixture of the R- and S- stereoisomers. S-warfarin is 3-5 times more potent than R-warfarin and is metabolized predominantly to 7- and 6- hydroxyl metabolites via CYP2C9. Warfarin exerts its anticoagulant effect through inhibition of its molecular target VKORC1, which in turn limits availability of reduced vitamin K, leading to decreased formation of functionally active clotting factors. These clotting factors are glycoproteins that are post-translationally carboxylated by gamma-glutamyl carboxylase (GGCX) to Gla-containing proteins. The endoplasmic reticulum chaperone protein calumenin (CALU) can bind to and inhibit GGCX activity. The metabolism of reduced vitamin K to hydroxyvitamin K1 is catalyzed by CYP4F2 which removes vitamin K from the vitamin K cycle (adapted from warfarin pharmacokinetics (PK) and pharmacodynamics (PD) pathways at PharmGKB, http://www.pharmgkb.org/do/serve?objId=PA451906&objCls=Drug#tabview=tab4).
Genes: CYP2C9, VKORC1 and CYP4F2
There is substantial candidate gene literature evaluating associations with warfarin dose requirements, as well as several reported genome-wide association studies (Supplemental Tables S1-S7). The genes with the strongest literature support, and for which we make recommendations for use in warfarin dosing, are CYP2C9, VKORC1 and CYP4F2. Additionally, genome-wide association studies have identified an independently significant single nucleotide polymorphism (SNP) in the CYP2C cluster (7), which has also been incorporated into this updated recommendation.
CYP2C9 and warfarin
CYP2C9 is a hepatic drug-metabolizing enzyme in the cytochrome P450 (CYP450) superfamily (8), and is the primary metabolizing enzyme of S-warfarin (Figure 1). CYP2C9 has over 60 known variant alleles (http://www.cypalleles.ki.se/cyp2c9.htm; CYP2C9 allele definition table (9)). Individuals homozygous for the reference CYP2C9 allele (CYP2C9*1) have the “normal metabolizer” phenotype. Each named CYP2C9 star (*) allele is defined by one or more specific SNPs and to date, and 18 alleles have been associated with decreased enzyme activity (CYP2C9 allele definition table-(9)). The two most common decreased function alleles among individuals of European ancestry are CYP2C9*2 (c.430C>T; p.Arg144Cys; rs1799853) and CYP2C9*3 (c.1075A>C; p.Ile359Leu; rs1057910) (8). CYP2C9 allele frequencies differ between racial/ethnic groups (8, 10).
In vitro and in vivo studies suggest CYP2C9*2 and *3 impair metabolism of S-warfarin by ∼30-40% and ∼80-90%, respectively (8). Compared to patients homozygous for CYP2C9*1, individuals who inherit one or two copies of CYP2C9*2 or *3 are at greater risk of bleeding during warfarin therapy (11, 12), require lower doses to achieve similar levels of anticoagulation, and require more time to achieve a stable INR (11) (Supplemental Table S1). Additional CYP2C9 alleles (CYP2C9*5, *6, *8, and *11) are associated with decreased function of the CYP2C9 enzyme and contribute to dose variability. These alleles are found with the highest frequency among those of African ancestry, and collectively are more common than CYP2C9*2 and *3 in that population (CYP2C9 frequency table; (9)).
VKORC1 and warfarin
VKORC1 encodes the vitamin K epoxide reductase protein, the target enzyme of warfarin (6). VKORC1 catalyzes the conversion of vitamin K-epoxide to vitamin K, which is the rate-limiting step in vitamin K recycling (13).
A common variant upstream of VKORC1 (c.-1639G>A, rs9923231) is significantly associated with warfarin sensitivity and patients with one or two -1639A require progressively lower warfarin doses than -1639G/G homozygotes (10, 14-18). The -1639G>A polymorphism is present on a haplotype that affects VKORC1 protein expression. (18).
Other common VKORC1 SNPs or haplotypes do not further improve warfarin dose prediction (10, 16). The c.-1639G>A allele frequency varies among different ancestral populations (VKORC1 frequency table; (19)), and largely explains the differences in average dose requirements between whites, blacks and Asians (10, 17). Several rare non-synonymous VKORC1 variants confer warfarin resistance (high dose requirements) and are detailed in Supplemental Table S2 (20).
CYP4F2 and warfarin
CYP4F2 is a primary liver vitamin K oxidase that catalyzes the metabolism of vitamin K to hydroxy-vitamin K1 and removes vitamin K from the vitamin K cycle (21) (Figure 1). It acts as an important counterpart to VKORC1 in limiting excessive accumulation of vitamin K. The non-synonymous variant CYP4F2*3 (c.1297G>A; p.Val433Met; rs2108622) was first shown to affect enzyme activity and associated with warfarin dose in three independent white cohorts (22-24). Furthermore, including this CYP4F2 variant in warfarin dosing models that included CYP2C9, VKORC1 and clinical factors improved the accuracy of dose prediction (25). This correlation has been confirmed in subsequent studies with those of European and Asian ancestry, though not those of African ancestry (26, 27). Two large meta-analyses (one in Han Chinese that pulled in substantial Chinese literature) provide the best estimates for the influence data of CYP4F2*3 on warfarin dose requirements (26, 27). They suggest statistically significant but modest impacts of 8-11% higher warfarin doses in A allele carriers (Supplemental Table S3).
CYP2C rs12777823 and warfarin
rs12777823 is a SNP in the CYP2C cluster near the CYP2C18 gene on chromosome 10 and is associated with a clinically relevant effect on warfarin dose through significant alterations in warfarin clearance, independent of CYP2C9*2 and *3 (7). This association was first identified through a genome-wide association study in African Americans (p=1.51×10-8) and confirmed in a replication cohort (p=5.04×10–5); meta-analysis of the two cohorts together produced a p value of 4.5 ×10–12. This study concluded that African Americans who are heterozygous or homozygous for the rs12777823 A allele require a dose reduction of ∼ 7 or 9 mg/week, respectively (7). Regression analysis showed that addition of this SNP improves the dosing algorithm published by the International Warfarin Pharmacogenetics Consortium (IWPC) by 21%. Further studies have demonstrated the importance of this SNP in African Americans (28). Although this variant is common in other ethnic populations, an association with warfarin dose has only been detected among African Americans suggesting it is not the underlying cause but likely inherited with other variant(s) on a haplotype that influences warfarin dose in this population. Of note, an association was not observed in a cohort of Egyptians, thus it is not possible to make broad statements about this allele in people of continental African ancestry. Most African Americans are of West African ancestry; it is unknown whether similar associations are present in individuals from other parts of Africa.
Genetic Test Interpretation
CYP2C9. Clinical laboratories typically report CYP2C9 genotype results using the star (*) allele nomenclature system and an interpretation that includes a predicted metabolizer phenotype. Most FDA-approved CYP2C9 tests include only *2 and *3, which is not as informative for African ancestry populations; however, some clinical laboratories may offer expanded CYP2C9 panels validated as laboratory developed tests (LDTs) (for allele frequencies see: CYP2C9 frequency table (9)).
VKORC1
Clinical laboratories typically report VKORC1 genotype results by c.-1639G>A (or the linked 1173C>T; rs9934438) genotype (e.g., G/A) and an interpretation on warfarin sensitivity. Most commercial genotyping platforms do not detect rare VKORC1 variants that have been associated with warfarin resistance (VKORC1 frequency table (19)).
CYP4F2
Although not as commonly tested for as CYP2C9 and VKORC1, some clinical laboratories may also test for CYP4F2 using a targeted genotyping laboratory developed test to detect CYP4F2*3 (c.1297G>A, p.Val433Met; rs2108622) variant. Results are typically reported by nucleotide (e.g., G/A), amino acid (e.g., Val/Met) or star (*) allele (*1/*3) genotype and an interpretation related to warfarin dosing.
CYP2C rs12777823
Given the recent identification of the association between rs12777823 (g.96405502G>A) and warfarin dosing among African Americans, most clinical laboratories do not currently include this non-coding variant in their warfarin pharmacogenetic genotyping panels. However, the increasing accessibility of clinical research genomics programs that return actionable results and the notable effect of this variant among African Americans suggests that some patients may have genotype results for this variant in the future. Results would likely be reported by genotype (e.g., G/A) and an interpretation related to warfarin dosing.
Genetic test options
Commercially available genetic testing options change over time. Additional information about pharmacogenetic testing can be found at the Genetic Testing Registry (http://www.ncbi.nlm.nih.gov/gtr/).
Incidental findings
No diseases have been linked to common CYP2C9 variants independent of drug metabolism and response. Similarly, no diseases have been consistently linked to common VKORC1 and CYP4F2 variants that are interrogated in warfarin response tests. However, homozygosity for rare coding mutations in VKORC1 are a known cause of combined deficiency of vitamin K-dependent clotting factors-2 (VKCFD2), which is a rare and potentially fatal bleeding disorder that can be reversed by oral administration of vitamin K (29).
Linking genetic variability to variability in drug-related phenotypes
Common variants in CYP2C9, VKORC1, and CYP4F2 account for up to 18%, 30%, and 11% respectively, of the variance in stable warfarin dose among patients of European ancestry (10, 16, 17, 30, 31), but because of differing allele frequencies across populations, these variants explain less of the dose variability in patients of other ancestries. In particular, CYP2C9*2 is virtually absent in Asians, and additional CYP2C9 alleles (e.g. *5, *6, *8, and *11 alleles) occur almost exclusively in persons of African ancestry and contribute to dose variability in this population. Other genes of potential importance are discussed in the Supplemental Material.
Published in 2013, the European Pharmacogenetics of Anticoagulant Therapy (EU-PACT) and Clarification of Optimal Anticoagulation through Genetics (COAG) trials examined the efficacy of genotype-guided warfarin dosing in randomized controlled trials (32, 33). In a homogenous European population, the EU-PACT trial showed shorter time to stable dose, improved percent time in therapeutic range, and reduced number of episodes with an INR>4 using a pharmacogenetic dosing algorithm compared to standard dosing (33). The COAG trial was conducted in an ethnically diverse cohort with 27% of participants of African ancestry (32). Overall, COAG did not show a difference in time to stable dose, percent time in therapeutic range, reduction in number of episodes with INR >4 or <2, or bleeding risk with a pharmacogenetic dosing algorithm compared to a clinical algorithm. In non-blacks, the pharmacogenetic dosing algorithm arm had more patients whose stable dose was within 1 mg per day of the algorithm-predicted dose (57 vs 39%, respectively). In contrast, the pharmacogenetic dosing algorithm was less accurate at predicting within 1 mg/day of the stable dose than the clinical algorithm in blacks (38 vs 48% respectively) (32). Blacks were more likely to have an INR above range with pharmacogenetic dosing, which could be due to the genotyping panel in the COAG trial being limited to CYP2C9*2, *3 and VKORC1 c.-1639G>A. Other variants that influence warfarin dose and are more common in blacks (i.e., CYP2C9*5, *6, *8, and *11 and rs12777823) were not genotyped in the COAG trial and their absence likely led to significant overdosing in patients with these alleles (10, 34). Consequently, this updated CPIC guideline recommends against pharmacogenetic dosing of warfarin in blacks when only CYP2C9*2 and *3 genotype results are available.
The Genetics-In Formatics Trial (GIFT) was a randomized controlled trial examining the effectiveness and safety of genotype-guided dosing versus clinical algorithm dosing in orthopedic patients with a composite outcome that included symptomatic and asymptomatic venous thromboembolism, major hemorrhage, INR ≥ 4, and death (35). It is the first warfarin pharmacogenetics trial powered for clinical outcomes. GIFT included genotyping for CYP2C9*2 and *3, CYP4F2*3, and VKORC1-1639, but did not include the African-specific CYP2C9 alleles or rs12777823. The results of GIFT were presented in early 2017 and revealed a 27% reduction in the composite outcome with genotype-guided versus clinical algorithm dosing, documenting the clinical benefits of a genotype guided approach to warfarin dosing.(https://www.sciencedaily.com/releases/2017/03/170320091104.htm)
Therapeutic Recommendations: Adults
Recommendations for warfarin maintenance (chronic) dosage based on genetic information
We use the three-tiered rating system described previously (and in Supplemental Material) (1) in which ratings of strong, moderate, and optional are applied based on the evidence reviewed. The recommendations for dosing based on genotype contained herein include recommendations and are derived from numerous observational and prospective studies, and randomized trials that suggest the ability to more accurately identify stable therapeutic warfarin dose requirements through use of both genetic and clinical information. Data from prospective studies and randomized controlled trials are equivocal on whether the improvement in dosing prediction by pharmacogenetics dosing leads to improved clinical outcomes. The majority of the literature underpinning these guidelines arises from individuals of European ancestry, African Americans, and East Asians. However, the more limited literature in other populations generally suggests the guidelines are appropriate in them also.
Numerous studies have derived warfarin dosing algorithms that use both genetic and non-genetic factors to predict warfarin dose (16, 17, 36, 37). Two algorithms perform well in estimating stable warfarin dose (16, 17) and were created using more than 5000 subjects, though as noted above, more recent data suggest they do not perform acceptably in African Americans when used without modification for CYP2C9 alleles frequently found in the African population (32). The Gage and IWPC algorithms or minor adjustments to them have also been the algorithms used in both randomized controlled trials and most of the prospective dosing studies. Dosing algorithms using genetic information outperform non-genetic clinical algorithms and fixed-dose approaches in dose prediction, except in African Americans when the algorithm only includes CYP2C9*2 and *3 (16, 17, 32). Genetics-based algorithms also better predict warfarin dose than the FDA-approved warfarin label table (38).
Pharmacogenetic algorithm-based warfarin dosing
This guideline recommends that pharmacogenetic warfarin dosing be accomplished through the use of one of the pharmacogenetic dosing algorithms described above, as summarized in Figure 2. These algorithms, as originally published, are available in the Supplement and the dosing algorithm published by IWPC is also online at http://www.pharmgkb.org/do/serve?objId=PA162372936&objCls=Dataset#tabview=tab2. The two algorithms provide very similar dose recommendations. The clinical and genetic information used in one or both algorithms is shown in box 1. These algorithms compute the anticipated stable daily warfarin dose to one decimal and the clinician must then prescribe a regimen (e.g., an estimate of 4.3 mg/day might be given as 4 mg daily except 5 mg two days per week). An additional “dose revision” algorithm, that can be used on days 4-5 of therapy for dose refinement and uses genetic information, was tested in COAG and EU-PACT and can also be used (36) (Supplemental Table S5).
Figure 2. Dosing recommendations for Warfarin dosing based on genotype for adult patients.

a“Dose clinically” means to dose without genetic information, which may include use of a clinical dosing algorithm or standard dose approach
bData strongest for European and East Asian ancestry populations and consistent in other populations.
c45-50% of individuals with self-reported African ancestry carry CYP2C9*5,*6,*8,*11, or rs12777823. IF CYP2C9*5, *6, *8, and *11 WERE NOT TESTED, DOSE WARFARIN CLINICALLY. Note: these data derive primarily from African Americans, who are largely from West Africa. It is unknown if the same associations are present for those from other parts of Africa.
dMost algorithms are developed for the target INR 2-3.
eConsider an alternative agent in individuals with genotypes associated with CYP2C9 poor metabolism (e.g., CYP2C9*3/*3, *2/*3, *3/*3) or both increased sensitivity (VKORC1 A/G or A/A) and CYP2C9 poor metabolism.
fSee the EU-PACT trial for pharmacogenetics-based warfarin initiation (loading) dose algorithm (33) with the caveat that the loading dose PG algorithm has not been specifically tested or validated in populations of African ancestry.
gLarger dose reduction might be needed in variant homozygotes (i.e. 20-40%).
hAfrican American refers to individuals mainly originating from West Africa.
Text box. Patient characteristics utilized in the Gage (16), or IWPC (17) algorithms or both.
Age
Sex
Race
Weight
Height
Smoking status
Warfarin indication
Target INR
- Interacting drugs
- Inhibitors: Amiodarone, statins, sulfamethoxazole, azole antifungals
- Inducers: Rifampin, phenytoin, carbamazepine
- Genetic variables
- CYP2C9 genotype
- VKORC1 genotype
- Gage algorithm can also incorporate CYP4F2 and GGCX genotypes
It is important to note that these algorithms do not include CYP4F2, CYP2C9*5, *6, *8, or *11 or rs12777823, and incorporation of these should be added when results are available, as described in Figure 2. The warfarindosing.org website contains both algorithms, the Gage algorithm (16) as the primary algorithm and the IWPC algorithm (17) as the secondary algorithm and can adjust for CYP4F2, CYP2C9*5 and *6. If utilizing warfarindosing.org, the user should be clear on whether the algorithm is or is not incorporating genotypes beyond CYP2C9 *2 and *3 and VKORC1, which are the only three genotypes in the original version of both algorithms.
Pharmacogenetics-informed loading (or initiation) dose calculations
The use of a different initial warfarin dose (or “loading dose”) is somewhat controversial and plays different roles in different regions of the world, based on experience and local standards. Recent data from a diverse U.S. based cohort suggest that failure to provide a loading dose in patients with zero or one variant alleles in VKORC1 or CYP2C9 may delay time to therapeutic INR and reduce time in therapeutic range in the initial month of therapy (39). A genetically-guided loading dose approach was developed by Avery et al. (37) and a slightly modified version was successfully implemented in the EU-PACT trial (33). In COAG CYP2C9 variant alleles were not considered for the initial dose, providing a small loading dose on day 1. Whether differences in loading dose strategies between the EU-PACT and COAG trials contributed to differing results is not known. If loading doses are to be used, a genetically-informed approach to calculating the loading dose may be helpful. The majority of the experience with a genetically-informed loading regimen is in those of European ancestry. Determination of maintenance dose would be as described above.
Non-African ancestry recommendation
In patients who self-identify as non-African ancestry, the recommendation, as summarized in Figure 2, is to: 1) calculate warfarin dosing using a published pharmacogenetic algorithm (16, 17), including genotype information for VKORC1-1639G>A and CYP2C9*2 and *3. In individuals with genotypes associated with CYP2C9 poor metabolism (e.g., CYP2C9 *2/*3, *3/*3) or both increased sensitivity (VKORC1-1639 A/A) and CYP2C9 poor metabolism, an alternative oral anticoagulant might be considered. The bulk of the literature informing these recommendations is in European and Asian ancestry populations, but consistent data exist for other non-African populations. These recommendations are graded as STRONG. 2) If a loading dose is to be utilized, the EU-PACT loading dose algorithm that incorporates genetic information could be used (33). This recommendation is OPTIONAL. 3) While CYP2C9*5, *6, *8, or*11 variant alleles are commonly referred to as African specific alleles, they can occur among individuals who do not identify as, or know of their, African ancestry. If these variant alleles are detected, decrease calculated dose by 15-30% per variant allele or consider an alternative agent. Larger dose reductions might be needed in patients homozygous for variant alleles (i.e. 20-40%, e.g. CYP2C9*2/*5). This recommendation is graded as OPTIONAL. 4) If the CYP4F2*3 (i.e., c.1297A, p.433Met) allele is also detected, increase the dose by 5-10%. This recommendation is also considered OPTIONAL. 5) The data do not suggest an association between rs12777823 genotype and warfarin dose in non-African Americans, thus rs12777823 should not be considered in these individuals (even if available).
African ancestry recommendation
In patients of African ancestry, CYP2C9*5, *6, *8, *11 are important for warfarin dosing. If these genotypes are not available, warfarin should be dosed clinically without consideration for genotype. If CYP2C9*5, *6, *8, and *11 are known, then the recommendation, as shown in Figure 2, is to: 1) calculate warfarin dose using a validated pharmacogenetic algorithm, including genotype information for VKORC1 c.-1639G>A and CYP2C9*2 and *3 (16, 17); 2) if the individual carriers a CYP2C9*5, *6, *8, or *11 variant allele(s), decrease calculated dose by 15-30%. Larger dose reductions might be needed in patients who carry two variant alleles (e.g., CYP2C9*5/*6) (i.e. 20-40% dose reduction). 3) In addition, rs12777823 is associated with warfarin dosing in African Americans (mainly originating from West Africa). Thus, in African Americans a dose reductions of 10-25% in those with rs12777823 A/G or A/A genotype is recommended. These recommendations are considered MODERATE.
In individuals with genotypes that predict CYP2C9 poor metabolism or who have increased warfarin sensitivity (VKORC1 c.-1639 A/A) and CYP2C9 poor metabolism, an alternative oral anticoagulant should be considered (see Supplemental material for definitions of strength of recommendations). As noted above, for non-African ancestry, if a loading dose is to be used, the EU-PACT algorithm (33) that incorporates genetic information could be used to calculate loading dose. This recommendation is OPTIONAL. The data do not support an impact on clinical phenotype for CYP4F2 on warfarin dosing in those of African ancestry and so no recommendation is made for use of CYP4F2 genotype data in blacks.
Recommendations for Pediatric Patients
As detailed in Supplemental Table S7, there is strong evidence for the use of CYP2C9*2 and *3 and VKORC1-1639G>A genotype to guide warfarin dosing in children of European ancestry. The studies in Japanese pediatric individuals are conflicting as VKORC1 and CYP2C9 could not be adequately evaluated due to the low numbers of CYP2C9 variant carriers. For other ethnicities, there is no evidence documenting that VKORC1 and CYP2C9 are important. Furthermore, there are no data in children that included CYP2C9*5, *6, *8, or *11 genotyping. Based on the current evidence, in children of European ancestry and if CYP2C9*2 and *3 and VKORC1-1639 genotype are available, calculate warfarin dosing based on a validated published pediatric pharmacogenetic algorithm (Figure 3) (40, 41). A dosing tool that can be used in children of European ancestry is available at http://www.warfarindoserevision.com (42).
Figure 3. Dosing recommendations for Warfarin dosing based on genotype for pediatric patients.

aData strongest for European ancestry populations and consistent in most Japanese studies.
b“Dose clinically” means to dose without genetic information, which may include use of a clinical dosing algorithm or standard dose approach
cValidated published pediatric pharmacogenetic algorithms include Hamberg et al.(42) and Biss et al.(41)
dNo studies in children included CYP2C9*5, *6, *8, or *11 genotyping.
Other considerations
Given the effects of CYP2C9 on warfarin clearance, and given that the CYP2C9 variant alleles are associated with reduced warfarin clearance, CYP2C9 genotype may influence time to onset and offset of anticoagulation, as measured by INR (43). The Supplemental Material summarizes other considerations in the dosing of warfarin, including clinical factors and interacting drugs, some of which are included in the pharmacogenetic dosing algorithms (see Text Box). Other genes of potential importance are detailed in the Supplemental Material and Supplemental table S6, including CALU and GGCX. Most clinical genotyping platforms do not include these genes, nor do the dosing tables or published algorithms. The Supplemental Material also discusses incorporation of genetic information into the initial dose, and alternatives to warfarin.
Potential Benefits and Risks for the Patient
Incorporation of genetic information has the potential to shorten the time to stable INR, increase the time within the therapeutic INR range, and reduce under-dosing or over-dosing during the initial treatment period (33). If these benefits are achieved, they could result in a reduced risk of bleeding and thromboembolic events (12, 44). There are also potential risks. For example, using genetic information to guide dosing may lead to false security and inadequate INR monitoring. In particular, there are risks of using pharmacogenetic dosing in those of African ancestry if only CYP2C9 *2 and *3 alleles are included. Genetic-guided dosing may increase the risk for over-dosing or under-dosing, especially in individuals who carry rare or untested variants and are assigned as “wild-type” by default (17, 32). The cost-benefit of genetic-guided therapy depends on the cost of genotyping and the reduction in adverse events (45), and most insurance plans do not currently pay for warfarin pharmacogenetic testing. Although there is substantial evidence associating CYP2C9 and VKORC1 variants with warfarin dosing, randomized clinical trials have demonstrated inconsistent results in terms of clinical outcomes (see Linking genetic variability to variability in drug-related phenotypes). Although genotyping is reliable when performed in qualified laboratories, an additional risk is an error in genotyping or reporting of genotype. Genotypes are life-long test results, so such error could have long-term adverse health implications.
Caveats: Appropriate Use and/or Potential Misuse of Genetic Tests
Many pharmacogenetic dosing algorithms are developed for a target INR of 2-3 (17) and so their utility for estimating therapeutic warfarin doses with other target INR ranges is uncertain; however, some algorithms accommodate the target INR explicitly (16, 42). Pharmacogenetic-guided warfarin dosing does not alter the requirements for regular INR monitoring. There are patients for whom genetic testing is likely to be of little or no benefit, including those who already have had long-term treatment with stable warfarin doses and those who are unable to achieve stable dosing due to variable adherence. The greatest potential benefit is early in the course of therapy (before therapy initiation or in the early days of therapy) (36). It is likely that patients on therapy for many weeks to months, with careful INR monitoring, will derive little benefit from subsequent warfarin pharmacogenetics testing (46).
Supplementary Material
Acknowledgments
This work was funded by the National Institutes of Health (NIH) for CPIC (R24GM115264) and PharmGKB (R24GM61374). Relevant funding for other authors includes: NIH grants U01 GM074492 and U01 HG 007269 (JAJ), K23GM104401 (SAS), GM109145 (CMS), R01HL092173 and K24HL133373 (NAL), R01 HL097036 (BFG) and grants from the Swedish Research Council (Medicine 521-2011-2440 and 521-2014-3370), the Swedish Heart and Lung Foundation (20120557 and 20140291), and the Thuréus' Foundation (MW), the UK Department of Health and Medical Research Council (MP), and the EU FP7 programme for funding EU-PACT (MP, MW).
Footnotes
Disclaimer: Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines reflect expert consensus based on clinical evidence and peer-reviewed literature available at the time they are written and are intended only to assist clinicians in decision-making and to identify questions for further research. New evidence may have emerged since the time a guideline was submitted for publication. Guidelines are limited in scope and are not applicable to interventions or diseases not specifically identified. Guidelines do not account for all individual variations among patients and cannot be considered inclusive of all proper methods of care or exclusive of other treatments. It remains the responsibility of the health care provider to determine the best course of treatment for a patient. Adherence to any guideline is voluntary, with the ultimate determination regarding its application to be made solely by the clinician and the patient. CPIC assumes no responsibility for any injury to persons or damage to persons or property arising out of or related to any use of CPIC's guidelines, or for any errors or omissions.
Conflicts of interest: J.A.J. is on the CPIC Steering Committee and has no conflicts of interest related to this guideline. T.E.K and M.W.C. are paid scientific advisors to the Rxight™ Pharmacogenetic Program. S.A.S. is a director of a clinical laboratory that performs CYP2C9 and VKORC1 genetic testing. All other authors declare no conflicts of interest related to this guideline.
References
- 1.Relling MV, Klein TE. CPIC: Clinical Pharmacogenetics Implementation Consortium of the Pharmacogenomics Research Network. Clin Pharmacol Ther. 2011;89:464–7. doi: 10.1038/clpt.2010.279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pengo V, Pegoraro C, Cucchini U, Iliceto S. Worldwide management of oral anticoagulant therapy: the ISAM study. Journal of thrombosis and thrombolysis. 2006;21:73–7. doi: 10.1007/s11239-006-5580-y. [DOI] [PubMed] [Google Scholar]
- 3.Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. (8th) 2008;133:160S–98S. doi: 10.1378/chest.08-0670. [DOI] [PubMed] [Google Scholar]
- 4.Kearon C, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149:315–52. doi: 10.1016/j.chest.2015.11.026. [DOI] [PubMed] [Google Scholar]
- 5.Shehab N, Sperling LS, Kegler SR, Budnitz DS. National estimates of emergency department visits for hemorrhage-related adverse events from clopidogrel plus aspirin and from warfarin. Arch Intern Med. 2010;170:1926–33. doi: 10.1001/archinternmed.2010.407. [DOI] [PubMed] [Google Scholar]
- 6.Rost S, et al. Mutations in VKORC1 cause warfarin resistance and multiple coagulation factor deficiency type 2. Nature. 2004;427:537–41. doi: 10.1038/nature02214. [DOI] [PubMed] [Google Scholar]
- 7.Perera MA, et al. Genetic variants associated with warfarin dose in African-American individuals: a genome-wide association study. Lancet. 2013;382:790–6. doi: 10.1016/S0140-6736(13)60681-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lee CR, Goldstein JA, Pieper JA. Cytochrome P450 2C9 polymorphisms: a comprehensive review of the in-vitro and human data. Pharmacogenetics. 2002;12:251–63. doi: 10.1097/00008571-200204000-00010. [DOI] [PubMed] [Google Scholar]
- 9.Gene Refernece Materials for CYP2C9. [Accessed November 4, 2016];2016 < https://www.pharmgkb.org/page/cyp2c9RefMaterials>.
- 10.Limdi NA, et al. Warfarin pharmacogenetics: a single VKORC1 polymorphism is predictive of dose across 3 racial groups. Blood. 2010;115:3827–34. doi: 10.1182/blood-2009-12-255992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Aithal GP, Day CP, Kesteven PJ, Daly AK. Association of polymorphisms in the cytochrome P450 CYP2C9 with warfarin dose requirement and risk of bleeding complications. Lancet. 1999;353:717–9. doi: 10.1016/S0140-6736(98)04474-2. [DOI] [PubMed] [Google Scholar]
- 12.Mega JL, et al. Genetics and the clinical response to warfarin and edoxaban: findings from the randomised, double-blind ENGAGE AF-TIMI 48 trial. Lancet. 2015;385:2280–7. doi: 10.1016/S0140-6736(14)61994-2. [DOI] [PubMed] [Google Scholar]
- 13.Wajih N, Hutson SM, Owen J, Wallin R. Increased production of functional recombinant human clotting factor IX by baby hamster kidney cells engineered to overexpress VKORC1, the vitamin K 2,3-epoxide-reducing enzyme of the vitamin K cycle. The Journal of biological chemistry. 2005;280:31603–7. doi: 10.1074/jbc.M505373200. [DOI] [PubMed] [Google Scholar]
- 14.Wadelius M, et al. Common VKORC1 and GGCX polymorphisms associated with warfarin dose. Pharmacogenomics J. 2005;5:262–70. doi: 10.1038/sj.tpj.6500313. [DOI] [PubMed] [Google Scholar]
- 15.Yuan HY, et al. A novel functional VKORC1 promoter polymorphism is associated with inter-individual and inter-ethnic differences in warfarin sensitivity. Human molecular genetics. 2005;14:1745–51. doi: 10.1093/hmg/ddi180. [DOI] [PubMed] [Google Scholar]
- 16.Gage BF, et al. Use of pharmacogenetic and clinical factors to predict the therapeutic dose of warfarin. Clin Pharmacol Ther. 2008;84:326–31. doi: 10.1038/clpt.2008.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Klein TE, et al. Estimation of the warfarin dose with clinical and pharmacogenetic data. The New England journal of medicine. 2009;360:753–64. doi: 10.1056/NEJMoa0809329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rieder MJ, et al. Effect of VKORC1 haplotypes on transcriptional regulation and warfarin dose. N Engl J Med. 2005;352:2285–93. doi: 10.1056/NEJMoa044503. [DOI] [PubMed] [Google Scholar]
- 19.Gene Reference Materials for VKORC1. [Accessed November 4, 2016]; < https://www.pharmgkb.org/page/vkorc1RefMaterials>.
- 20.Scott SA, Edelmann L, Kornreich R, Desnick RJ. Warfarin pharmacogenetics: CYP2C9 and VKORC1 genotypes predict different sensitivity and resistance frequencies in the Ashkenazi and Sephardi Jewish populations. American journal of human genetics. 2008;82:495–500. doi: 10.1016/j.ajhg.2007.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.McDonald MG, Rieder MJ, Nakano M, Hsia CK, Rettie AE. CYP4F2 is a vitamin K1 oxidase: An explanation for altered warfarin dose in carriers of the V433M variant. Molecular pharmacology. 2009;75:1337–46. doi: 10.1124/mol.109.054833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Caldwell MD, et al. CYP4F2 genetic variant alters required warfarin dose. Blood. 2008;111:4106–12. doi: 10.1182/blood-2007-11-122010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Stec DE, Roman RJ, Flasch A, Rieder MJ. Functional polymorphism in human CYP4F2 decreases 20-HETE production. Physiol Genomics. 2007;30:74–81. doi: 10.1152/physiolgenomics.00003.2007. [DOI] [PubMed] [Google Scholar]
- 24.Gene Refernece Materials for CYP4F2. [Accessed November 4, 2016]; < https://www.pharmgkb.org/page/cyp4f2RefMaterials>.
- 25.Borgiani P, et al. CYP4F2 genetic variant (rs2108622) significantly contributes to warfarin dosing variability in the Italian population. Pharmacogenomics. 2009;10:261–6. doi: 10.2217/14622416.10.2.261. [DOI] [PubMed] [Google Scholar]
- 26.Danese E, et al. Impact of the CYP4F2 p.V433M polymorphism on coumarin dose requirement: systematic review and meta-analysis. Clin Pharmacol Ther. 2012;92:746–56. doi: 10.1038/clpt.2012.184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zhang JE, et al. Effects of CYP4F2 genetic polymorphisms and haplotypes on clinical outcomes in patients initiated on warfarin therapy. Pharmacogenet Genomics. 2009;19:781–9. doi: 10.1097/FPC.0b013e3283311347. [DOI] [PubMed] [Google Scholar]
- 28.Alzubiedi S, Saleh MI. Pharmacogenetic-guided Warfarin Dosing Algorithm in African-Americans. J Cardiovasc Pharmacol. 2016;67:86–92. doi: 10.1097/FJC.0000000000000317. [DOI] [PubMed] [Google Scholar]
- 29.Oldenburg J, et al. Congenital deficiency of vitamin K dependent coagulation factors in two families presents as a genetic defect of the vitamin K-epoxide-reductase-complex. Thrombosis and haemostasis. 2000;84:937–41. [PubMed] [Google Scholar]
- 30.Wadelius M, et al. The largest prospective warfarin-treated cohort supports genetic forecasting. Blood. 2008 doi: 10.1182/blood-2008-04-149070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Liang R, Wang C, Zhao H, Huang J, Hu D, Sun Y. Influence of CYP4F2 genotype on warfarin dose requirement-a systematic review and meta-analysis. Thromb Res. 2012;130:38–44. doi: 10.1016/j.thromres.2011.11.043. [DOI] [PubMed] [Google Scholar]
- 32.Kimmel SE, et al. A pharmacogenetic versus a clinical algorithm for warfarin dosing. N Engl J Med. 2013;369:2283–93. doi: 10.1056/NEJMoa1310669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Pirmohamed M, et al. A randomized trial of genotype-guided dosing of warfarin. N Engl J Med. 2013;369:2294–303. doi: 10.1056/NEJMoa1311386. [DOI] [PubMed] [Google Scholar]
- 34.Drozda K, et al. Poor warfarin dose prediction with pharmacogenetic algorithms that exclude genotypes important for African Americans. Pharmacogenet Genomics. 2015;25:73–81. doi: 10.1097/FPC.0000000000000108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Do EJ, et al. Genetics informatics trial (GIFT) of warfarin to prevent deep vein thrombosis (DVT): rationale and study design. Pharmacogenomics J. 2012;12:417–24. doi: 10.1038/tpj.2011.18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lenzini P, et al. Integration of genetic, clinical, and INR data to refine warfarin dosing. Clin Pharmacol Ther. 2010;87:572–8. doi: 10.1038/clpt.2010.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Avery PJ, et al. A proposal for an individualized pharmacogenetics-based warfarin initiation dose regimen for patients commencing anticoagulation therapy. Clin Pharmacol Ther. 2011;90:701–6. doi: 10.1038/clpt.2011.186. [DOI] [PubMed] [Google Scholar]
- 38.Finkelman BS, Gage BF, Johnson JA, Brensinger CM, Kimmel SE. Genetic warfarin dosing: tables versus algorithms. J Am Coll Cardiol. 2011;57:612–8. doi: 10.1016/j.jacc.2010.08.643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Arwood MJ, et al. Anticoagulation endpoints with clinical implementation of warfarin pharmacogenetic dosing in a real-world setting: A proposal for a new pharmacogenetic dosing approach. Clin Pharmacol Ther. 2016 doi: 10.1002/cpt.558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Hamberg AK, et al. Warfarin dose prediction in children using pharmacometric bridging--comparison with published pharmacogenetic dosing algorithms. Eur J Clin Pharmacol. 2013;69:1275–83. doi: 10.1007/s00228-012-1466-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Biss TT, et al. VKORC1 and CYP2C9 genotype and patient characteristics explain a large proportion of the variability in warfarin dose requirement among children. Blood. 2012;119:868–73. doi: 10.1182/blood-2011-08-372722. [DOI] [PubMed] [Google Scholar]
- 42.Hamberg AK, Wadelius M, Friberg LE, Biss TT, Kamali F, Jonsson EN. Characterizing variability in warfarin dose requirements in children using modelling and simulation. Br J Clin Pharmacol. 2014;78:158–69. doi: 10.1111/bcp.12308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hamberg AK, et al. A pharmacometric model describing the relationship between warfarin dose and INR response with respect to variations in CYP2C9, VKORC1, and age. Clin Pharmacol Ther. 2010;87:727–34. doi: 10.1038/clpt.2010.37. [DOI] [PubMed] [Google Scholar]
- 44.Oden A, Fahlen M. Oral anticoagulation and risk of death: a medical record linkage study. BMJ. 2002;325:1073–5. doi: 10.1136/bmj.325.7372.1073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Eckman MH, Rosand J, Greenberg SM, Gage BF. Cost-effectiveness of using pharmacogenetic information in warfarin dosing for patients with nonvalvular atrial fibrillation. Ann Intern Med. 2009;150:73–83. doi: 10.7326/0003-4819-150-2-200901200-00005. [DOI] [PubMed] [Google Scholar]
- 46.Ferder NS, et al. Ability of VKORC1 and CYP2C9 to predict therapeutic warfarin dose during the initial weeks of therapy. J Thromb Haemost. 2010;8:95–100. doi: 10.1111/j.1538-7836.2009.03677.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.