

Summary:
Basal cell carcinoma (BCC) is the most common periocular skin cancer and can lead to significant morbidity. We assess the effectiveness of vismodegib, a first-in-class Hedgehog signaling pathway inhibitor, in the management of periocular and orbital BCCs based on clinical response, tolerability, and orbital content preservation. All patients with periocular or orbital BCCs who met criteria for vismodegib treatment were recruited prospectively between May 2012 and 2014 from 2 hospitals. Patients received oral vismodegib (150 mg daily) until disease progression, unacceptable toxicity, or withdrawal. All patients were followed up monthly. Patient demographics, tumor size, treatment duration including dosing regimen, adverse events, response rate, duration of response, progression-free survival, and disease-free survival were analyzed. All 15 patients had biopsy-proven BCCs with no metastatic disease at presentation. The mean age was 74 years and 10 patients (67%) had orbital involvement. The mean lesion longest dimension was 51 mm and 7 cases (47%) represented recurrence following previous surgery and/or radiotherapy. The mean treatment duration was 13 months and mean follow-up duration 36 months. Ten patients (67%) had a complete response, 3 (20%) had a partial response, and 2 had progressive disease following an initial partial response (13%). The partial response of 55% in 1 patient allowed subsequent surgical resection with clear margins. Vismodegib is effective for treating periocular and orbital BCCs with orbital salvage of patients who otherwise would have required exenteration. There is a neoadjuvant role for vismodegib but further studies are required.
INTRODUCTION
Basal cell carcinoma (BCC) is the most common type of skin cancer and accounts for 80% of nonmelanoma skin cancers.1,2 It also represents 90% of malignant eyelid tumors.3 Orbital invasion is reported in 2–4% of cases.4,5 Patients with advanced BCC (locally advanced or metastatic) may not be suitable candidates for surgical management or radiotherapy due to factors such as inoperable disease, multiple comorbidities, or low chance of cure. The treatment of advanced BCC has been revolutionized with the discovery of the Hedgehog signaling pathway and its role in BCC.6 Vismodegib (Erivedge, GDC-0449, Genentech/Roche) is a first-in-class Hedgehog signaling pathway inhibitor approved for advanced BCC in the United States and United Kingdom based on the pivotal study ERIVANCE BCC.7
The aim of this study was to assess the effectiveness of vismodegib to treat periocular and orbital BCCs based on clinical response, tolerability, and orbital content preservation.
PATIENTS AND METHODS
All consecutive patients with periocular or orbital BCCs who met criteria for vismodegib treatment were recruited prospectively between May 2012 and 2014 from 2 tertiary hospitals. Specifically, this included patients aged 18 years or older, advanced BCC considered inoperable or surgery contraindicated and radiotherapy contraindicated or inappropriate, Eastern Cooperative Oncology Group performance status 0–2. Patients were excluded if they were having concurrent antitumor therapy, completion of most recent antitumor therapy less than 21 days before initiation of treatment, or uncontrolled medical illness.
All patients received oral vismodegib (150 mg daily) until disease progression, unacceptable toxicity, or withdrawal. Between May 2012 and 2013, all recruited patients were also part of the STEVIE study (NCT01367665).8,9 All patients were followed up monthly.
Safety was assessed by the Common Terminology Criteria for Adverse Events version 4.0 from the National Cancer Institute.10 Treatment response was assessed according to Response Evaluation Criteria in Solid Tumours version 1.1.11
This study was performed in accordance with the Helsinki Declaration. Written informed consent was obtained from patients.
RESULTS
All 15 patients had biopsy-proven BCC with no metastatic disease at presentation. The first 11 patients were also part of the STEVIE study.9 Patient demographics, treatment response, and adverse events are summarized in Table 1. Indications for vismodegib treatment included inoperable disease (n = 2), significant morbidity associated with orbital exenteration and/or radiotherapy (n = 12), or low chance of surgical cure due to multiple recurrences in a patient with basal-cell nevus syndrome (n = 1; case 8). The mean age was 74 years (range, 44–90 years), and 10 patients (67%) had orbital involvement. The mean lesion longest dimension was 51 mm (range, 8–115 mm), and 7 cases (47%) represented recurrence following previous surgery and/or radiotherapy.
Table 1.
Demographic Data, Treatment Response, and Adverse Events of Vismodegib for the Management of Locally Advanced Periocular and Orbital Basal Cell Carcinomas (Data Correct as of November 01, 2016)

The mean treatment duration was 13 months (range, 2–40 months) and mean follow-up duration 36 months (range, 14–52 months). The most common adverse events (93% of patients) included dysgeusia (87%), muscle spasms (53%), alopecia (53%), and asthenia (40%). All these were mild or moderate in severity. Treatment was discontinued in 14 patients (73%) because of adverse events (n = 5; cases 1, 3, 4, 10, and 15), disease progression (n = 2; cases 9 and 12), patient request (n = 4; case 7, 11, 13, and 14), investigator request (n = 1; poor attendance of case 5), death not considered related to the study drug by the investigator (n = 1; lung cancer in case 2) or surgical clearance (n = 1; case 6).
Ten patients (67%) had a complete response, 3 (20%) had a partial response, and 2 had progressive disease following an initial partial response (13%). The treatment response rates are illustrated in Figure 1.
Fig. 1.
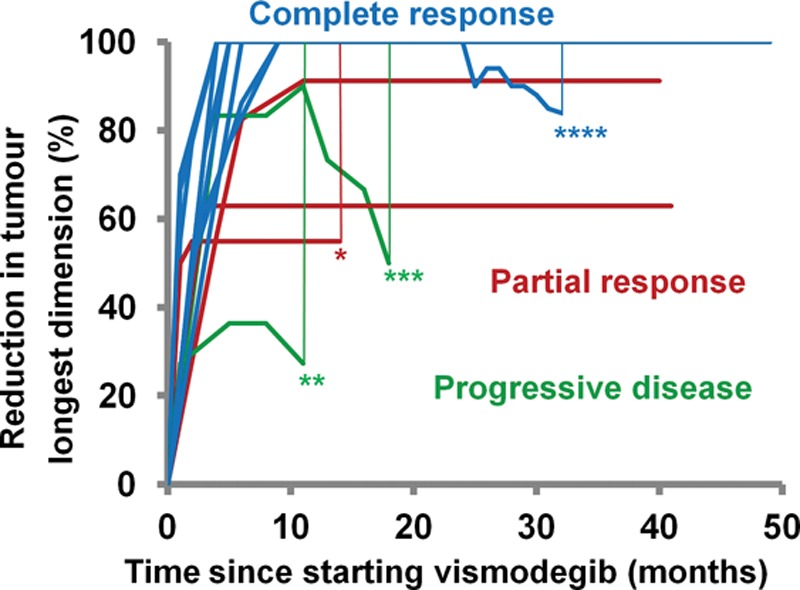
BCC shrinkage in 15 patients treated with vismodegib. A partial response of 55% in 1 case allowed subsequent surgical clearance (*). Two patients had disease progression following a partial response of 90% (**) and 36% (***). They both underwent subsequent orbital exenteration and remain disease free at 2 years postoperative follow-up. There was 1 case of recurrence that required orbital exenteration (****) following a complete response of 21 months. The patient died 7 months later.
Recurrence occurred in 1 patient 21 months after a complete response and 10 months following stopping vismodegib (case 7). There was disease progression despite restarting vismodegib so the patient required orbital exenteration, frontal craniectomy, and reconstruction with a free anterolateral thigh flap. The patient died 7 months later.
Two patients had disease progression following a partial response of 90% and 36% for 14 and 11 months respectively (case 9 and 12). They both underwent subsequent orbital exenteration and free anterolateral thigh flap reconstruction. Both patients remain disease free at 2 years postoperative follow-up.
All 3 cases requiring orbital exenteration had initial orbital invasion. The 7 other patients with orbital invasion demonstrated complete response [Fig. 2 showing case 1; see figure, Supplemental Digital Content 1, which displays BCC of right medial canthus with orbital invasion (case 3). Pre-vismodegib (a) and 4 months since treatment initiation (b). One year later (c), http://links.lww.com/PRSGO/A490]. The partial response of 55% in 1 patient (case 6) allowed subsequent surgical resection with clear margins (see figure, Supplemental Digital Content 2, which displays BCC of left eyelids with orbital invasion. Pre-vismodegib (a) and 3 months since treatment initiation (b). A partial response of 55% allowed subsequent surgical clearance at 14 months (c), http://links.lww.com/PRSGO/A491; see figure, Supplemental Digital Content 3, which shows magnetic resonance imaging of the same patient. Pre-vismodegib (a) and 12 months since treatment initiation (b), http://links.lww.com/PRSGO/A492).
Fig. 2.
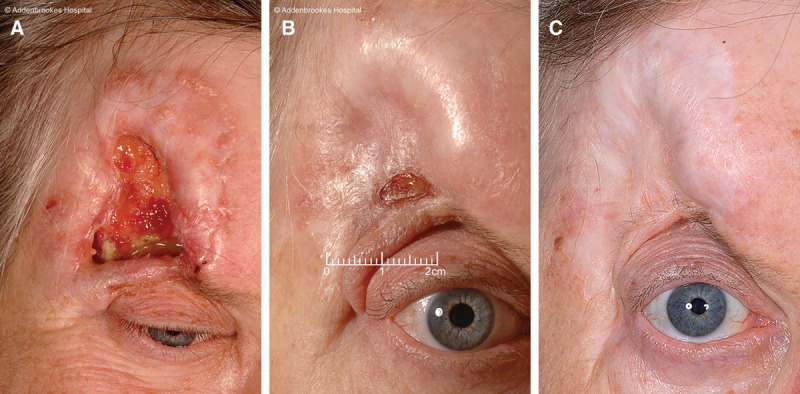
BCC of right forehead and upper eyelid with orbital invasion (case 1). Pre-vismodegib (A) and 4 months since treatment initiation (B). C, One year later.
DISCUSSION
The majority of BCCs are surgically excised with curative intent but advanced disease may be inoperable. Furthermore, surgery or radiotherapy may not be appropriate due to multiple recurrences or significant associated morbidity.
Orbital exenteration is a radical operation reserved for treating locally invasive or potentially life-threatening orbital disease that is not amenable to other options. Around 40–50% of exenterations performed by ophthalmologists are for eyelid or periocular skin tumors.12–15 Despite evidence that exenteration can achieve surgical cure,14,16,17 it is associated with significant morbidity and deformity.15,18–20
Most patients with BCC have dysregulated, abnormal Hedgehog signaling in isolated tumors and as part of the basal-cell naevus syndrome.21 The Hedgehog signaling pathway is a key regulator of cell growth and differentiation during fetal development. It is predominantly inactive in adults and suppressed by the constitutive inhibitory effects of the 12-transmembrane receptor Patched 1 (PTCH1) on Smoothened (SMO), a 7-transmembrane receptor. SMO promotes transcription of genes involved in cellular proliferation and angiogenesis.22
Most BCCs have either inactivating genetic alternations in PTCH1 or, less commonly, activating mutations in SMO.23–26 As a result of inactivating PTCH1 mutations or activating SMO mutations, SMO moves to the cell surface where it activates the GLI family of transcription factors. Activated GLI then moves to the nucleus and initiates the transcription of target genes inducing the formation of BCCs. Vismodegib offers an alternative treatment for advanced BCC by directly inhibiting SMO.
This is the largest case series to date of vismodegib for periocular and orbital BCC with a mean follow-up duration of 3 years (see table, Supplemental Digital Content 4, which displays a summary of case series of vismodegib for locally advanced periocular and orbital BCCs, http://links.lww.com/PRSGO/A493).27–29 Sonidegib is another hedgehog pathway inhibitor licensed for locally advanced BCC not amenable to surgery or radiotherapy.30
There are various questions not addressed by this study that require further investigation. First, the ideal treatment duration or role of interval dosing remains unclear. More advanced BCCs may require life-long treatment but the side effects can result in high rates of drug discontinuation, making intermittent treatment potentially a more acceptable approach. The ongoing STEVIE study8,9 assessing the safety of vismodegib in patients with advanced BCC may also help to guide strategies to improve drug tolerability. The MIKIE study (NCT01815840) found that intermittent dosing schedules are effective in patients with multiple BCCs, allowing them to benefit from long-term vismodegib treatment.31,32 A number of studies have characterized vismodegib side effects and useful treatment strategies.33,34
Second, resistance patterns of Hedgehog inhibitors have not yet been clearly defined. A recent study found that sequential arsenic trioxide and itraconazole treatment is a feasible option for metastatic BCC.35
Finally, there is a neoadjuvant role for vismodegib in making the inoperable operable and reducing the associated surgical morbidity. This role will likely become increasingly important with the emergence of drug resistance. In our series, the partial response of 55% in case 6 allowed subsequent surgical resection with clear margins and preservation of orbital contents. There have been several other case reports on the use of vismodegib in the neoadjuvant setting.36–38 Results from a study investigating the role of vismodegib in the neoadjuvant setting for high-risk operable BCCs suggest a minimum of 3 months of vismodegib can reduce the BCC surgical defect area.39,40 This is similar to our treatment response profile (Fig. 1). There are however concerns that histologically normal tissue interspersed with persistent BCC may confound tumor margin clearance.
With surgery, there is a reported incomplete BCC excision rate of up to 17%; both lesion location and grade of operating surgeon has a significant impact on this.41 Primary excision margins of periocular lesions may often be compromised to prevent causing functional impairment. When excision margins are involved, the recommendation is usually for reexcision, radiotherapy, or close outpatient follow-up. All these have a negative impact on patient experience and incur additional financial costs. Vismodegib treatment in the neoadjuvant setting may provide a cost-effective strategy to reduce the incomplete primary excision rates in high risk areas.
In conclusion, vismodegib appears to be effective for treating periocular and orbital BCCs with orbital salvage of patients who otherwise would have required exenteration. Some patients appear to have prolonged complete responses, even after treatment discontinuation. There is clearly a neoadjuvant role for vismodegib but further studies are required.
ACKNOWLEDGMENTS
The authors thank Faisal Ali for assistance with data collection.
PATIENT CONSENT
The patient provided written consent for the use of his image.
Footnotes
The STEVIE study was sponsored by F. Hoffman-La Roche. This article has not been originated or funded by F. Hoffman-La Roche or Roche Products Ltd. Roche Products Ltd. was not involved in the preparation, drafting, or editing of this article. Roche Products Limited has conducted a factual accuracy check on the final article, but any decisions to incorporate comments were made solely at the discretion of the authors.
Presented at the XV World Congress on Cancers of the Skin 2014, Edinburgh, United Kingdom; 50th European Society for Surgical Research Congress, 2015, Liverpool, United Kingdom; and 7th European Plastic Surgery Research Council Congress, 2015, Hamburg, Germany.
Disclosure: Drs. Fife, Lear, and Durrani have received honoraria from Roche for speaker and advisory board meetings. Dr. Fife has also received honoraria from Pfizer, Novartis, and Bristol-Myers Squibb for speaker and advisory board meetings; support of trials at Cambridge Cancer Centre from Roche (STEVIE trial) and other companies (renal cancer). Dr. Wong and Dr. Price have no conflicts of interest or financial disclosures to declare. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Madan V, Lear JT, Szeimies RM. Non-melanoma skin cancer. Lancet. 2010;375:673–685.. [DOI] [PubMed] [Google Scholar]
- 2.Bath-Hextall F, Leonardi-Bee J, Smith C, et al. Trends in incidence of skin basal cell carcinoma. Additional evidence from a UK primary care database study. Int J Cancer. 2007;121:2105–2108.. [DOI] [PubMed] [Google Scholar]
- 3.Cook BE, Jr, Bartley GB. Epidemiologic characteristics and clinical course of patients with malignant eyelid tumors in an incidence cohort in Olmsted County, Minnesota. Ophthalmology. 1999;106:746–750.. [DOI] [PubMed] [Google Scholar]
- 4.Sexton M, Jones DB, Maloney ME. Histologic pattern analysis of basal cell carcinoma. Study of a series of 1039 consecutive neoplasms. J Am Acad Dermatol. 1990;23:1118–1126.. [DOI] [PubMed] [Google Scholar]
- 5.Howard GR, Nerad JA, Carter KD, et al. Clinical characteristics associated with orbital invasion of cutaneous basal cell and squamous cell tumors of the eyelid. Am J Ophthalmol. 1992;113:123–133.. [DOI] [PubMed] [Google Scholar]
- 6.Lear JT. Oral hedgehog-pathway inhibitors for basal-cell carcinoma. N Engl J Med. 2012;366:2225–2226.. [DOI] [PubMed] [Google Scholar]
- 7.Sekulic A, Migden MR, Oro AE, et al. Efficacy and safety of vismodegib in advanced basal-cell carcinoma. N Engl J Med. 2012;366:2171–2179.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hoffmann-La Roche F; STEVIE: a study of vismodegib in patients with locally advanced or metastatic basal cell carcinoma. Available at http://clinicaltrials.gov/show/NCT01367665. Accessed February 1, 2017.
- 9.Basset-Seguin N, Hauschild A, Grob JJ, et al. Vismodegib in patients with advanced basal cell carcinoma (STEVIE): a pre-planned interim analysis of an international, open-label trial. Lancet Oncol. 2015;16:729–736.. [DOI] [PubMed] [Google Scholar]
- 10.US Department of Health and Human Services. National Cancer Institute (2010). Common toxicity criteria for adverse events, version 4.0. Available at http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf. Accessed February 1, 2017.
- 11.Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–247.. [DOI] [PubMed] [Google Scholar]
- 12.Goldberg RA, Kim JW, Shorr N. Orbital exenteration: results of an individualized approach. Ophthal Plast Reconstr Surg. 2003;19:229–236.. [DOI] [PubMed] [Google Scholar]
- 13.Günalp I, Gündüz K, Dürük K. Orbital exenteration: a review of 429 cases. Int Ophthalmol. 1995;19:177–184.. [DOI] [PubMed] [Google Scholar]
- 14.Rathbun JE, Beard C, Quickert MH. Evaluation of 48 cases of orbital exenteration. Am J Ophthalmol. 1971;72:191–199.. [DOI] [PubMed] [Google Scholar]
- 15.Ben Simon GJ, Schwarcz RM, Douglas R, et al. Orbital exenteration: one size does not fit all. Am J Ophthalmol. 2005;139:11–17.. [DOI] [PubMed] [Google Scholar]
- 16.Bartley GB, Garrity JA, Waller RR, et al. Orbital exenteration at the Mayo Clinic. 1967-1986. Ophthalmology. 1989;96:468–473.. [DOI] [PubMed] [Google Scholar]
- 17.Levin PS, Dutton JJ. A 20-year series of orbital exenteration. Am J Ophthalmol. 1991;112:496–501.. [DOI] [PubMed] [Google Scholar]
- 18.Kuo CH, Gao K, Clifford A, et al. Orbital exenterations: an 18-year experience from a single head and neck unit. ANZ J Surg. 2011;81:326–330.. [DOI] [PubMed] [Google Scholar]
- 19.Rahman I, Maino A, Cook AE, et al. Mortality following exenteration for malignant tumours of the orbit. Br J Ophthalmol. 2005;89:1445–1448.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wong JC, Thampy R, Cook A. Life expectancy following orbital exenteration. Br J Ophthalmol. 2015;99:1–4.. [DOI] [PubMed] [Google Scholar]
- 21.Harris LG, Samant RS, Shevde LA. Hedgehog signaling: networking to nurture a promalignant tumor microenvironment. Mol Cancer Res. 2011;9:1165–1174.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Low JA, de Sauvage FJ. Clinical experience with Hedgehog pathway inhibitors. J Clin Oncol. 2010;28:5321–5326.. [DOI] [PubMed] [Google Scholar]
- 23.Hahn H, Wicking C, Zaphiropoulous PG, et al. Mutations of the human homolog of Drosophila patched in the nevoid basal cell carcinoma syndrome. Cell. 1996;85:841–851.. [DOI] [PubMed] [Google Scholar]
- 24.Gailani MR, Ståhle-Bäckdahl M, Leffell DJ, et al. The role of the human homologue of Drosophila patched in sporadic basal cell carcinomas. Nat Genet. 1996;14:78–81.. [DOI] [PubMed] [Google Scholar]
- 25.Undén AB, Zaphiropoulos PG, Bruce K, et al. Human patched (PTCH) mRNA is overexpressed consistently in tumor cells of both familial and sporadic basal cell carcinoma. Cancer Res. 1997;57:2336–2340.. [PubMed] [Google Scholar]
- 26.Xie J, Murone M, Luoh SM, et al. Activating smoothened mutations in sporadic basal-cell carcinoma. Nature. 1998;391:90–92.. [DOI] [PubMed] [Google Scholar]
- 27.Gill HS, Moscato EE, Chang AL, et al. Vismodegib for periocular and orbital basal cell carcinoma. JAMA Ophthalmol. 2013;131:1591–1594.. [DOI] [PubMed] [Google Scholar]
- 28.Demirci H, Worden F, Nelson CC, et al. Efficacy of Vismodegib (Erivedge) for basal cell carcinoma involving the orbit and periocular area. Ophthal Plast Reconstr Surg. 2015;31:463–466.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ozgur OK, Yin V, Chou E, et al. Hedgehog pathway inhibition for locally advanced periocular basal cell carcinoma and basal cell nevus syndrome. Am J Ophthalmol. 2015;160:220–227.e2.. [DOI] [PubMed] [Google Scholar]
- 30.Migden MR, Guminski A, Gutzmer R, et al. Treatment with two different doses of sonidegib in patients with locally advanced or metastatic basal cell carcinoma (BOLT): a multicentre, randomised, double-blind phase 2 trial. Lancet Oncol. 2015;16:716–728.. [DOI] [PubMed] [Google Scholar]
- 31.Rogers G, Kunstfeld R, Schadendorf D, et al. ; Mikie: a randomized, double-blinded, regimen-controlled, phase 2 study to assess the efficacy and safety of two different vismodegib (VISMO) regimens in patients (pts) with multiple basal cell carcinomas (BCCs). Available at http://meetinglibrary.asco.org/content/134946-144. Accessed February 1, 2017.
- 32.Dréno B, Kunstfeld R, Hauschild A, et al. Two intermittent vismodegib dosing regimens in patients with multiple basal-cell carcinomas (MIKIE): a randomised, regimen-controlled, double-blind, phase 2 trial. Lancet Oncol. 2017;18:404–412.. [DOI] [PubMed] [Google Scholar]
- 33.Fife K, Herd R, Lalondrelle S, et al. Managing adverse events associated with vismodegib in the treatment of basal cell carcinoma. Future Oncol. 2017;13:175–184.. [DOI] [PubMed] [Google Scholar]
- 34.Lacouture ME, Dréno B, Ascierto PA, et al. Characterization and management of Hedgehog pathway inhibitor-related adverse events in patients with advanced basal cell carcinoma. Oncologist. 2016;21:1218–1229.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ally MS, Ransohoff K, Sarin K, et al. Effects of combined treatment with arsenic trioxide and itraconazole in patients with refractory metastatic basal cell carcinoma. JAMA Dermatol. 2016;152:452–456.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Chang AL, Atwood SX, Tartar DM, et al. Surgical excision after neoadjuvant therapy with vismodegib for a locally advanced basal cell carcinoma and resistant basal carcinomas in Gorlin syndrome. JAMA Dermatol. 2013;149:639–641.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Aldabagh B, Yu J, Perkocha LA, et al. Histologic changes in basal cell carcinoma after treatment with vismodegib. Dermatol Surg. 2013;39:1703–1705.. [DOI] [PubMed] [Google Scholar]
- 38.Kahana A, Worden FP, Elner VM. Vismodegib as eye-sparing adjuvant treatment for orbital basal cell carcinoma. JAMA Ophthalmol. 2013;131:1364–1366.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Ally MS, Aasi SZ. The role of vismodegib in the management of advanced basal cell skin cancers: a review. Curr Dermatol Rep. 2014;3:98–102.. [Google Scholar]
- 40.Kwon GP, Ally MS, Bailey-Healy I, et al. Update to an open-label clinical trial of vismodegib as neoadjuvant before surgery for high-risk basal cell carcinoma (BCC). J Am Acad Dermatol. 2016;75:213–215.. [DOI] [PubMed] [Google Scholar]
- 41.Wong KY, Gilleard O, Price RD. Are non-melanoma skin cancer incomplete excision rates different between grades of plastic surgeons? J Plast Reconstr Aesthet Surg. 2013;66:e146–e148.. [DOI] [PubMed] [Google Scholar]