

Abstract
To understand the adaptive value of reminiscence, a mediational model of reminiscence was tested in a sample of older adults with mild to moderate depressive symptoms. Using structural equation modeling, we investigated if psychological resources (mastery and meaning in life) mediate the relation between reminiscence (positive: identity construction and problem solving; and negative: bitterness revival and boredom reduction) and psychological distress (depressive symptoms and anxiety symptoms). A total of 202 older Dutch adults living in the community participated in this study. The present study consisted of baseline measurements of a randomized controlled trial that evaluated the effectiveness of a life-review therapy intervention on depression. Results showed that psychological resources fully mediated the relation between negative reminiscence and psychological distress. Specifically, negative reminiscing is related to decreased psychological distress through meaning in life and sense of mastery. The study contributes to current knowledge on the relation between reminiscence and mental health, both empirically and clinically. It helps to increase understanding of how reminiscence is related to psychological distress, especially in depressed older adults, and the relative importance of psychological resources, i.e., mastery and meaning in life. From a clinical perspective, these findings suggest the usefulness of focusing on strengthening psychological resources in therapeutic reminiscence-based strategies for older adults with depressive symptoms.
Keywords: Adaptation, Reminiscence, Mastery, Meaning in life, Depressive symptoms, Anxiety symptoms
Introduction
In general, older adults face several challenges associated with aging, like cognitive decline, a deteriorated physical health, and loss of psychological resources; processes which can lead to psychological distress. Hence, it is important to know which mechanisms are related to a successful coping with psychological distress in later life. In the last fifty years, several authors have acknowledged the adaptive value of reminiscence for the mental health of older adults (e.g., Butler 1963; Cappeliez and O’Rourke 2006; Korte et al. 2011; O’Rourke et al. 2010; Webster et al. 2010; Westerhof et al. 2010a; Wink and Schiff 2002; Wong 1995; Wong and Watt 1991). Reminiscence can be briefly defined as a volitional or non-volitional process that involves recalling one’s private or shared memories (Bluck and Levine 1998). The present study investigates how reminiscence can contribute to psychological resources and thus also to psychological distress in older adults with mild to moderate depressive symptomatology.
Research shows that particular ways of reminiscing are correlated with psychological distress. The types of reminiscence most consistently associated with mental health are identity construction, problem solving, bitterness revival, and boredom reduction (Westerhof et al. 2010a). Identity construction consists of using memories to identify who we are, whereas problem solving is about reflecting on past coping strategies to cope with present difficulties (Webster 1993). Bitterness revival can be defined as rehashing and ruminating about memories of difficult life circumstances, lost opportunities, and misfortunes, whereas boredom reduction involves using memories to fill a void of stimulation or interest (Webster 1993). Using structural equation modeling (SEM), it was shown that identity construction and problem solving comprise one factor, called self-positive reminiscence, whereas bitterness revival and boredom reduction comprise a second factor called self-negative reminiscence. Self-positive reminiscence is negatively related to psychological distress and self-negative reminiscence is positively related to distress (Cappeliez et al. 2005; Cappeliez and O’Rourke 2006; O’Rourke et al. 2010). These findings are supported by meta-analytic studies showing that interventions, focusing on reducing self-negative reminiscing and promoting self-positive reminiscing, lead to a decrease in psychological distress (Bohlmeijer et al. 2003, 2007; Cuijpers et al. 2006; Pinquart et al. 2007).
A next step in our effort to understand the adaptive value of reminiscence for psychological distress is to explore in greater detail how these different types of reminiscence are related to psychological distress. Recently, Cappeliez and Robitaille (2010) investigated the role played by assimilative and accommodative coping in mediating the relations of self-positive and self-negative functions of reminiscence with mental health. Using SEM, they showed that coping resources fully mediated these relations. We expanded their model in two ways. First, as these authors also suggested, our focus was to test a mediational model of reminiscence and mental health in a sample of older adults already presenting moderate psychological distress. This is especially important from a clinical perspective, because it can generate useful information on tailoring reminiscence-based interventions to characteristics of participants. Korte et al. (2011) indeed underscored the importance of differentiating reminiscence interventions by means of their intended purpose and target group. They found that reminiscence mediated the relationship between critical life events and psychological distress in a sample of older adults with subclinical psychological distress.
Second, and from a clinical perspective, we were interested in examining psychological resources which were previously used in studies on the effects of reminiscence-based interventions. It has been suggested that reminiscence may foster mental health by the accumulation of feelings of mastery and meaning in life (Wong 1995). The concept of mastery refers to the extent to which individuals believe they are in control of their important life experiences (Pearlin and Schooler 1978). Meaning in life can be defined as having a sense of direction and order, a reason for existence, a clear sense of personal identity, and a high degree of social consciousness (Reker 1997). Mastery and meaning are theoretically related resources; for example, manageability (mastery) and meaningfulness (meaning) comprise components of Antonovsky’s model of sense of coherence (Antonovsky 1993), whereas environmental mastery (mastery) and purpose in life (meaning) are two of the six components of Ryff’s model of psychological well-being (Ryff 1989). Several authors have found that mastery and meaning in life work together as protective psychological resources of mental health (e.g., Seligman 1998; Taylor 1989; Taylor et al. 2000).
Several studies with older adults demonstrate strong relationships of mastery and meaning in life with mental health. In a large, recent study with older adults, Forbes (2010) demonstrated that mastery was a strong predictor, stronger than sociodemographic factors, of both health status and perceived health. In the same vein, Steunenberg et al. (2007) showed that higher levels of mastery predicted recovery of depression in later life. Similar results were found by Gadella (2010), who demonstrated that higher levels of mastery were associated with lower levels of psychological distress in older adults. Other studies have also shown that high levels of mastery facilitate adaptation to psychological distress in the face of stressful events (Jang et al. 2002; Kempen et al. 1997, 1999; Roberts et al. 1994; Schieman and Turner 1998). Another line of research suggests that older adults with a strong sense of meaning in life report better mental health than those with less meaning in their lives (Nygren et al. 2005; Reker 1997). In a large meta-analysis, Pinquart (2002) showed that purpose in life (meaning) has a strong negative correlation with depression. Like mastery, meaning in life appears to fulfill a stress-buffering and counter-depressive role in older adults (Krause 2004, 2007).
Reminiscence may either impede or strengthen the psychological resources of mastery and meaning. When reminiscing for self-negative purposes, people ruminate on unpleasant events, reflecting a failure to integrate problematic past experiences with the more positive aspects of life and thereby obstructing the feeling that life is manageable and meaningful (Wong 1989, 1995). On the other hand, reminiscence for self-positive purposes makes use of past experiences that might serve a role in enhancing a sense of mastery and meaning, for example by recalling events of previous accomplishments or by remembering events that provide a sense of meaning and direction (Wong 1995). Empirical studies have shown that reminiscence interventions may indeed enhance mastery and meaning in life (Bohlmeijer et al. 2009, 2005; Pot et al. 2010; Westerhof and Bohlmeijer 2004). These resources may even mediate the effects of reminiscence interventions on depressive symptoms (Watt 1996; Westerhof et al. 2010b). We will therefore concentrate on these resources in our mediating model.
In line with the above studies, the present study tested a mediational model of reminiscence and mental health in a sample of older adults with mild to moderate depressive symptoms. We predicted that mastery and meaning in life are relevant psychological resources in the relation between reminiscence functions and psychological distress. A recent study shows that findings on the relation between reminiscence and psychological distress in the general older population may be generalized to older adults with depressive symptomatology (Korte et al. 2011). Therefore, using SEM, we tested a model that involved both direct links between self-positive (identity and problem solving) and self-negative (bitterness revival and boredom reduction) reminiscing, on the one hand, and psychological distress (depression and anxiety), on the other, together with indirect links mediated by psychological resources (mastery and meaning in life). More specifically, it was hypothesized that self-positive reminiscing would be positively linked to the personal resources of mastery and meaning leading to reduced psychological distress. Furthermore, it was hypothesized that self-negative reminiscing would be negatively related to these two resources, resulting in increased psychological distress.
Design and methods
Participants
A total of 202 older Dutch adults living in the community participated in this study (77 % female), with a mean age of 63 years (SD = 6.48, range 55–83). Participants’ level of formal education was equally represented among three categories (33.6 % <11 years, 33.7 % 11–14 years, and 32.7 % >14 years of schooling). A high number of participants were retired (30.7 %). Participants’ daily activities could best be described as doing volunteer work (18.3 %), having a paid job, doing the housekeeping, receiving a disability pension (each 15.8 %), or unemployed (3.5 %). On average, participants reported one to two chronic medical conditions (M = 1.5, SD = 1.4, range 0–6) and they experienced two to three critical life events in the last three years (M = 2.3, SD = 1.5, range 0–7). All of these older adults participated in a randomized controlled trial that evaluated the effectiveness of a life-review therapy intervention on depression (Korte et al. 2009, 2012). The present study consisted of baseline measurements of the participants in that study. All measurements were taken before the randomization process.
Recruitment
In cooperation with 14 Dutch mental healthcare institutions, an open recruitment strategy was used via advertisements in regional and national newspapers, posters, and information booklets available at healthcare institutions and surgeries of general practitioners, plus a radio interview and a commercial. The intervention was implemented by psychologists and other therapists in the participating mental healthcare institutions. In order to take part, people had to experience mild to moderate depressive symptoms and be aged 55 or over. To ensure that only older adults with mild to moderate symptoms of depression were included, people with a low score (0–4) on the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff 1977) were excluded. Furthermore, all older adults were examined with the Mini International Neuropsychiatric Interview (MINI; Sheehan et al. 1998). Diagnosis of a severe major depressive disorder through the MINI resulted in exclusion from the study. People were also excluded if they were currently receiving any form of treatment in a mental healthcare institution, or had recently started taking anti-depressant medication (within the previous 2 months). Eligible applicants were asked to sign an informed consent form. This study was approved by the METiGG, a medical-ethics committee for research in mental health care settings in the Netherlands. Furthermore, this study has been registered in the Netherlands Trial Register, the primary Dutch register for clinical trials (TC = 1,860). For a more elaborate description of the design of the study, we refer to Korte et al. (2009).
Measurements
Reminiscence functions
Reminiscence functions were measured with the Dutch version of the reminiscence functions scale (RFS), a questionnaire that assesses reminiscence functions over the course of a person’s life (Webster 1993). The scale comprises eight subscales reflecting possible functions of reminiscence. We only included four of the RFS subscales that have been most consistently related to mental health in previous research (Cappeliez et al. 2005; Cappeliez and O’Rourke 2006; Cully et al. 2001; Westerhof et al. 2010a), namely identity (6 items), problem solving (6 items), bitterness revival (5 items), and boredom reduction (6 items). Prompted by “When I reminisce, it is…” various reasons or motivations to reminisce were proposed to the participants. Possible answers ranged from 1 to 6 (never, rarely, seldom, occasionally, often, or very often). Examples were: “When I reminisce, it is…to see how my past fits in with my journey through life” (identity), “…to help me plan for the future” (problem solving), “…to keep painful memories alive” (bitterness revival), or “…to pass the time during idle or restless hours” (boredom reduction). Scores were each averaged per subscale representing a particular reminiscence function, a higher score signifying a more frequent reliance on that reminiscence function. The RFS has shown satisfactory psychometric properties in different samples of adults of various ages, including older adults (Webster 1993; Robitaille et al. 2010). The four subscales showed good internal consistency in the present sample (identity: α = .85, problem solving: α = .79, bitterness revival: α = .83, boredom reduction: α = .86).
Mastery
To assess the degree of mastery over one’s life, the Dutch version of the Mastery Scale was used (Pearlin and Schooler 1978). This scale consists of seven items intended to assess beliefs in perceived control over one’s life in general or beliefs regarding one’s ability to control an event. We used the abbreviated version of five items which are each phrased in a negative way. Possible responses were given on a 5-point scale ranging from 1 “strongly disagree” to 5 “strongly agree”. Summary scores ranged from 5 to 25. Higher scores on the scale thus indicate higher levels of mastery. The Mastery Scale has good psychometric properties (Pearlin and Schooler 1978). In the present study, the scale showed a good internal consistency (α = .79).
Meaning in life
Meaning in life was measured using the Dutch version of the meaning in life questionnaire (MLQ), a 10-item measure (Steger et al. 2006). The scale comprises two subscales: the presence of meaning and the search for meaning in life. The presence of meaning refers to comprehension of life experiences and a sense of overarching purpose, whereas search for meaning refers to the intensity and activity with seeking to establish and/or increase thereof. For the purpose of this study, we only included the 5-item presence of meaning scale, as this yielded more consistent relations with mental health than the search for meaning scale (Steger et al. 2006). Participants answered on a 5-point scale from 1 “absolutely untrue” to 5 “absolutely true” to what they thought made their life feel important to them. Examples were: “I understand my life’s meaning” and “I have discovered a satisfying life purpose”. The MLQ has good psychometric properties (Steger et al. 2006). The subscale presence of meaning showed a good internal consistency in the present study (α = .80).
Depressive symptoms
Participants’ depressive symptoms were measured using the Dutch version of the Center for Epidemiologic Studies Depression Scale (CES-D), a 20-item, self-report scale developed to measure depressive symptoms in the community. Participants indicated how often they had experienced each symptom during the previous week. Response categories, ranging from 0 to 3, are “rarely or never,” “some of the time,” “occasionally,” or “mostly or always.” Summation results in a CES-D score range from 0 to 60. A score of 16 or higher is considered indicative of clinically relevant depressive disorders. (Radloff 1977). The psychometric properties of the scale were found to be good (Radloff 1977), and particularly in a similar sample of older Dutch people with depressive symptoms (Haringsma et al. 2004). In this study, the scale showed good internal consistency (α = .84).
Anxiety symptoms
Participants’ anxiety symptoms were assessed using the anxiety scale of the Hospital Anxiety and Depression Scale (HADS-A), a 7-item, self-report screening scale on which respondents are asked to indicate whether they had experienced feelings of restlessness, tenseness, or panic during the past four weeks (Zigmond and Snaith 1983). Items range from 0 “rarely or never” to 3 “always or most of the time.” The Dutch translation has shown good psychometric properties in six different groups of Dutch subjects (Spinhoven et al. 1997). The scale showed satisfactory internal consistency in this study (α = .78).
Data analysis
Analyses were performed with Missing Value Analysis in PASW 18 to impute all missing data on the continuous measures with the expectation–maximization (EM) method. Missing values based on maximum likelihood estimates were imputed using observed data in an iterative process (Dempster et al. 1977). The total percentage of missing data was 2.48 %. All variables were inspected for skewness and kurtosis. Next, descriptive analyses were carried out to analyze the means, standard deviations, and bivariate correlations of all study variables. An exploratory factor analysis was carried out to provide the first evidence for the measurement model.
Using SEM with AMOS 16.0, a mediational model of reminiscence and psychological distress was tested. Self-positive reminiscence functions (identity and problem solving), self-negative reminiscence functions (bitterness revival and boredom reduction), psychological resources (mastery and meaning in life), and psychological distress (depression and anxiety) were modeled as latent variables composed of measured variables. To test the significance of the mediated effect, we compared the fit of two predictor–mediator–outcome models: one with a direct and an indirect path from the predictor to the outcome and one with only the indirect path (Frazier et al. 2004). A mediational model is supported if the first model does not provide a better fit to the data than the second model. We calculated the difference between the χ2 values and the degrees of freedom of both models to assess whether they differ significantly. If there is no significant difference, this implies that the model without the direct path explains the data equally well and is preferred to the fuller model that includes the direct path.
The fit of the model was judged by the χ2 test, the comparative fit index (CFI), the root mean square error of approximation (RMSEA), and the goodness of fit index (GFI). The CFI evaluates the fit of the estimated model relative to the fit of the independent model (where no relationships are estimated between variables), whereas the RMSEA is a popular measure that also considers the complexity of the model (i.e., the degrees of freedom). Finally, the GFI is a measure of the proportion of variance and covariance that the proposed model is able to explain (similar to R 2 in regression; Byrne 2001). CFI and GFI values >0.95 are indicative of an acceptable fit. RMSEA values <0.05 represent a good fit, while values <0.08 represent a reasonable fit (Hu and Bentler 1999).
Results
The skewness and kurtosis of all study variables varied between −1.09 and 0.614, and −0.603 and 1.68 respectively, values which are well within the acceptable range to proceed with SEM (West et al. 1995). Descriptive results and bivariate correlations between all observed study variables are presented in Table 1. On average, participants scored 20.5 (SD = 8.57) on the CES-D, indicating that the older adults in this study reported mild to moderate depressive symptoms. In total, 68.8 % of the participants met the cut-off for clinically relevant depressive symptoms. It can be seen that not all variables were significantly related. First, bitterness revival and boredom reduction reminiscence were both positively related to depression, but unrelated to anxiety, whereas identity and problem solving reminiscence were both unrelated to depression and anxiety. Second, bitterness revival and boredom reduction reminiscence were negatively related to mastery, but unrelated to meaning in life, whereas identity and problem solving reminiscence were unrelated to both mastery and meaning in life. Third, mastery and meaning in life were negatively related to depression and anxiety. The exploratory factor analysis revealed four factors: self-positive reminiscence (identity construction and problem solving), self-negative reminiscence (bitterness revival and boredom reduction), psychological resources (mastery and meaning in life), and psychological distress (depression and anxiety).
Table 1.
Descriptive statistics and bivariate correlation of all observed variables (N = 204)
| Variables | Mean (SD) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|---|
| Identity | 23.6 (5.44) | – | |||||||
| Problem solving | 23.0 (5.07) | 0.78** | – | ||||||
| Bitterness revival | 14.4 (5.39) | 0.31** | 0.33** | – | |||||
| Boredom reduction | 13.4 (5.99) | 0.36** | 0.29** | 0.58** | – | ||||
| Mastery | 14.8 (3.38) | −0.10 | −0.05 | −0.30** | −0.21** | – | |||
| Meaning in life | 15.1 (3.44) | 0.02 | 0.11 | −0.10 | −0.03 | 0.34** | – | ||
| Depressive symptoms | 20.5 (8.57) | 0.05 | 0.02 | 0.14* | 0.16* | −0.37** | −0.36** | – | |
| Anxiety symptoms | 8.35 (3.51) | −0.00 | 0.01 | 0.05 | 0.01 | −0.25** | −0.19** | 0.52** | – |
* p < 0.05, ** p < 0.01
Correlations between all latent variables are shown in Table 2. At the latent level, corrected for measurement error, self-negative reminiscence was positively related to psychological distress and negatively to psychological resources. Furthermore, the variable psychological resources was negatively related to psychological distress. There are no significant relations of self-positive reminiscence with psychological resources and psychological distress.
Table 2.
Correlations between latent variables
| Correlations | p value | |
|---|---|---|
| Self-positive and self-negative reminiscence | .474 | .000 |
| Self-positive reminiscence and psychological resources | −.036 | .729 |
| Self-negative reminiscence and psychological resources | −.411 | .003 |
| Psychological distress and psychological resources | −.654 | .050 |
| Self-positive reminiscence and psychological distress | .042 | .610 |
| Self-negative reminiscence and psychological distress | .197 | .029 |
Mediation was supported, as the model including a direct path between reminiscence and psychological distress did not provide a better fit to the data than the model with only the indirect path (Δχ2 = 0.893, df = 2; p > .05). Besides, the previous low, but significant latent correlation (r = .20) between negative reminiscence and psychological distress becomes insignificant. Therefore, we report fit indices for the preferred second model. A non-significant χ2 was obtained (χ2 = 22.7, df = 16, p = 0.121), indicating a good overall model fit. Furthermore, the goodness-of-fit of the model was confirmed using the values of the CFI (0.99), RMSEA (0.05), and GFI (0.97).
Figure 1 shows the standardized regression weights for each path tested in the model. Identity and problem solving, and bitterness revival and boredom reduction contribute equally to the measurement of the self-positive and self-negative latent constructs, respectively. As for the latent construct psychological resources, mastery contributes somewhat more than meaning in life. Depression contributed most to the measurement of the latent construct psychological distress. There is no direct relation between self-positive reminiscence and psychological resources. However, there is a significant relation between self-negative reminiscence and psychological resources. Moreover, psychological resources fully mediate the relation between self-negative reminiscence and psychological distress. The indirect effect of self-negative reminiscence on psychological distress is .36 (standardized estimate).
Fig. 1.
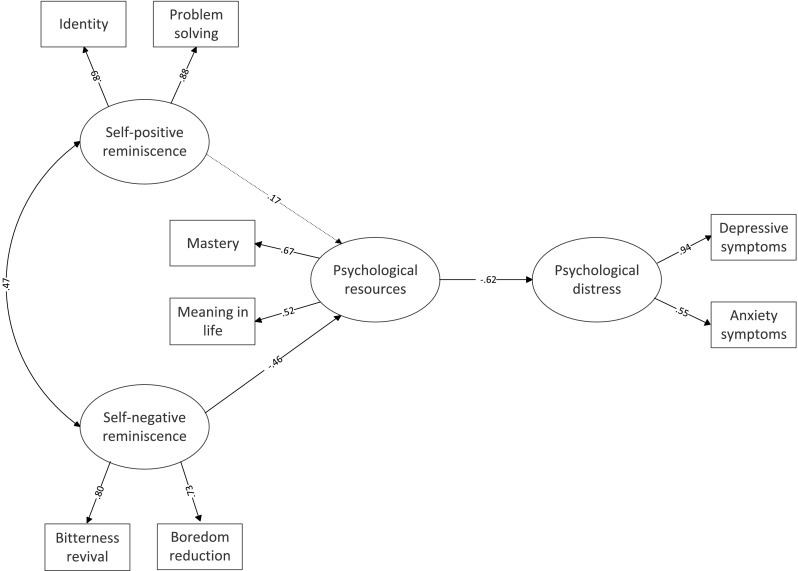
SEM model of reminiscence and psychological distress and psychological resources as a mediator. Note The model includes standardized estimates. The dotted line represents a non-significant path
Discussion
The purpose of this study was to test the mediating effects of psychological resources (mastery and meaning in life) in the relation of self-positive reminiscence (identity and problem solving) and self-negative reminiscence (bitterness revival and boredom reduction) with psychological distress (depression and anxiety) among older adults reporting mild to moderate psychological distress. Our hypothesis of an indirect effect of both self-negative and self-positive reminiscence functions on psychological distress, through psychological resources, is partly supported by the results. To be precise, self-negative functions of reminiscence are related to lower psychological distress through psychological resources. However, this hypothesized mediating link of psychological resources was not found in the case of the self-positive functions of reminiscence. These results mean that more frequent reminiscences for bitterness revival and boredom reduction are accompanied by lower levels of the psychological resources: meaning in life and sense of mastery. In turn, the negative relation between these psychological resources and psychological distress indicate that lower levels of psychological resources are associated with increased psychological distress.
Our results are largely in line with a recent study carried out by Cappeliez and Robitaille (2010). As in our study, they also found a negative relation between self-negative reminiscence and coping (i.e., assimilative coping and accommodative coping). However, in contrast to our findings, they also identified a significant mediation of the link between self-positive reminiscence and well-being by coping. The model can only be partially expanded to people with mild to moderate distress and to the psychological resources investigated in our study. The sample of Cappeliez and Robitaille’s (2010) study was composed of a general sample of older adults, whereas our study targeted specifically older adults with mild to moderate depressive symptomatology. One might wonder why engaging in self-positive reminiscence functions does not lead to decreased psychological distress in older adults who are depressed. Studies on autobiographical memory have shown that depressed individuals have difficulties in recalling specific positive memories (Williams et al. 2007). When engaging in self-positive reminiscence, they might in fact stick to over-general memories. This might not be helpful for the purposes of consolidating identity or finding a solution to a current problem. The self-reported use of positive reminiscence on the RFS might therefore not be related to depression. Serrano et al. (2004) showed that providing practice in producing specific positive memories is indeed effective in reducing psychological distress among depressed older adults.
The present study underlines that psychological resources, more specifically mastery and meaning in life, are important in explaining the link between self-negative reminiscence and psychological distress. Other studies indeed acknowledged the adaptive function of meaning in life (Krause 2004, 2007) and mastery (Zarit et al. 1999) in depressive symptoms among older adults. Using one general construct for mastery and meaning in life, as we did in our study, might suggest that these are overlapping resources which can be influenced by one type of reminiscence intervention. Although the literature describes these resources separately, reminiscence-based interventions often try to influence these processes at once. For example, formulating new, realistic goals may improve meaning in life when these goals are related to the personal past and to important life values, but they may also influence mastery when people experience that they are able to actually reach those goals.
These findings have direct clinical implications. To decrease psychological distress in later life, it might be useful, perhaps even necessary, to focus on strategies that strengthen mastery and meaning in life. This is supported by the finding that reminiscence functions aimed at reducing self-negative functions are effectively enhancing mastery and meaning in life in older adults (Bohlmeijer et al. 2005, 2009, 2008; Pot et al. 2010; Westerhof et al. 2010b). This point is further supported by the demonstration by Westerhof et al. (2010b) that improved meaning in life mediates the effects of a reminiscence-based intervention on depressive symptoms.
Some limitations of this study should be acknowledged. First, this study used cross-sectional data to test a mediational model. Although testing mediation with SEM, a single-step approach, has advantages over more traditional mediation models, it is still not a method that can truly establish the existence of causal relations between variables. Rather they provide an evaluation of the fit between a hypothesized causal model and data as collected. A reverse causality might still be possible, for example an increase in psychological distress might cause fewer psychological resources, which would lead to self-negative forms of reminiscence. In order to be conclusive about causality, experimental studies or controlled intervention studies are needed. Second, for practical reasons, we have included only four reminiscence functions. It may be worthwhile to investigate how other, more social reminiscence functions are related to psychological distress. A related limitation is that we have included only two psychological resources as potential mediators in the relation between reminiscence and psychological distress. In future studies, it might be interesting to investigate other potentially mediating psychological resources, for example self-efficacy or self-esteem, which might also be related to self-positive reminiscing. Third, the majority of the older adults in our study were female and relatively “young,” which implies a limitation for the generalization of the findings. Therefore, in future studies it would be interesting to broaden the study sample by including adults from more senior segments of the population and also men. This would allow for testing possible differences between men and women and young–old and old–old adults. Finally, the sample comprised participants who had volunteered to participate in a clinical trial on the effectiveness of a reminiscence-based intervention. It may be that they have higher expectations about the effectiveness of reminiscing and even more experience with reminiscence as a helpful coping strategy compared to people who did not choose to participate. So they might have interpreted the RFS differently, which might have affected the findings. Possibly, this has led to a reduction in the variance, which makes it more difficult to find significant associations between reminiscence and mental health.
Despite these limitations, the present study contributes to the present knowledge of the relation between reminiscence and mental health, both empirically and clinically. Our study affords a better understanding of how reminiscence is related to psychological distress, especially in depressed older adults. In this respect, we have shown how important psychological resources, i.e., mastery and meaning, are. From a clinical perspective, our findings suggest that it might be useful in therapeutic reminiscence-based strategies for older adults with depressive symptoms and to focus on strengthening these psychological resources.
References
- Antonovsky A. The structure and properties of the sense of coherence scale. Soc Sci Med. 1993;36(6):725–733. doi: 10.1016/0277-9536(93)90033-Z. [DOI] [PubMed] [Google Scholar]
- Bluck S, Levine LJ. Reminiscence as autobiographical memory: a catalyst for reminiscence theory development. Ageing Soc. 1998;18(2):185–208. doi: 10.1017/S0144686X98006862. [DOI] [Google Scholar]
- Bohlmeijer ET, Smit F, Cuijpers P. Effects of reminiscence and life review on late-life depression: a meta-analysis. Int J Geriatr Psychiatry. 2003;18(12):1088–1094. doi: 10.1002/gps.1018. [DOI] [PubMed] [Google Scholar]
- Bohlmeijer ET, Valenkamp M, Westerhof G, Smit F, Cuijpers P. Creative reminiscence as an early intervention for depression: results of a pilot project. Aging Ment Health. 2005;9(4):302–304. doi: 10.1080/13607860500089567. [DOI] [PubMed] [Google Scholar]
- Bohlmeijer ET, Roemer M, Cuijpers P, Smit F. The effects of life-review on psychological well-being in older adults: a meta-analysis. Aging Ment Health. 2007;11(3):291–300. doi: 10.1080/13607860600963547. [DOI] [PubMed] [Google Scholar]
- Bohlmeijer ET, Westerhof GJ, Emmerik-de Jong M. The effects of integrative reminiscence on meaning in life: results of a quasi-experimental study. Aging Ment Health. 2008;12(5):639–646. doi: 10.1080/13607860802343209. [DOI] [PubMed] [Google Scholar]
- Bohlmeijer ET, Kramer J, Smit F, Onrust S, Van Marwijk H. The effects of integrative reminiscence on depressive symptomatology and mastery of older adults. Community Ment Health J. 2009;45(6):476–484. doi: 10.1007/s10597-009-9246-z. [DOI] [PubMed] [Google Scholar]
- Butler RN. The life-review: an interpretation of reminiscence in the aged. Psychiatry. 1963;26(1):65–76. doi: 10.1080/00332747.1963.11023339. [DOI] [PubMed] [Google Scholar]
- Byrne BM. Structural equation modeling with AMOS. Mahwah: Erlbaum; 2001. [Google Scholar]
- Cappeliez P, O’Rourke N. Empirical validation of a model of reminiscence and health in later life. J Gerontol B. 2006;61(4):237–244. doi: 10.1093/geronb/61.4.P237. [DOI] [PubMed] [Google Scholar]
- Cappeliez P, Robitaille A. Coping mediates the relationships between reminiscence and psychological well-being among older adults. Aging Ment Health. 2010;14(7):807–818. doi: 10.1080/13607861003713307. [DOI] [PubMed] [Google Scholar]
- Cappeliez P, O’Rourke N, Chaudhury H. Functions of reminiscence and mental health in later life. Aging Ment Health. 2005;9(4):295–301. doi: 10.1080/13607860500131427. [DOI] [PubMed] [Google Scholar]
- Cuijpers P, Van Straten A, Smit F. Psychological treatment of late-life depression: a meta-analysis of randomized controlled trials. Int J Geriatr Psychiatry. 2006;21:1139–1149. doi: 10.1002/gps.1620. [DOI] [PubMed] [Google Scholar]
- Cully JA, LaVoie D, Gfeller JD. Reminiscence, personality, and psychological functioning in older adults. Gerontologist. 2001;41:89–95. doi: 10.1093/geront/41.1.89. [DOI] [PubMed] [Google Scholar]
- Dempster AP, Laird NM, Rubin DB. Maximum Likelihood from incomplete data via the EM algorithm. J R Stat Soc. 1977;39(1):1–38. [Google Scholar]
- Forbes DA. Enhancing mastery and sense of coherence: important determinants of health in older adults. Geriatr Nurs. 2010;22(1):29–32. doi: 10.1067/mgn.2001.113532. [DOI] [PubMed] [Google Scholar]
- Frazier P, Tix A, Barron K. Testing moderator and mediator effects in counseling psychology research. J Couns Psychol. 2004;51(1):115–134. doi: 10.1037/0022-0167.51.1.115. [DOI] [Google Scholar]
- Gadella TM. The role of mastery and social support in the association between life stressors and psychological distress in older Canadians. J Gerontol Soc Work. 2010;53:512–530. doi: 10.1080/01634372.2010.490691. [DOI] [PubMed] [Google Scholar]
- Haringsma R, Engels GI, Beekman ATF, Spinhoven P. The criterion validity of the Center for Epidemiological Studies Depression Scale (CES-D) in a sample of self-referred elders with depressive symptomatology. Int J Geriatr Psychiatry. 2004;19:558–563. doi: 10.1002/gps.1130. [DOI] [PubMed] [Google Scholar]
- Hu LT, Bentler PM. Cut-off criteria for fit indices in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6:1–55. doi: 10.1080/10705519909540118. [DOI] [Google Scholar]
- Jang Y, Haley WE, Small BJ, Mortimer JA. The role of mastery and social resources in the associations between disability and depression in later life. Gerontologist. 2002;6:807–813. doi: 10.1093/geront/42.6.807. [DOI] [PubMed] [Google Scholar]
- Kempen GIJM, Jelicic M, Ormel J. Personality, chronic medical morbidity, and health-related quality of life among older persons. Health Psychol. 1997;16:539–549. doi: 10.1037/0278-6133.16.6.539. [DOI] [PubMed] [Google Scholar]
- Kempen GIJM, Van Heuvelen MJ, Van Sonderen E, Van den Brink RH, Kooijman AC, Ormel J. The relationship of functional limitations to disability and the moderating effects of psychological attributes in community-dwelling older adults. Soc Sci Med. 1999;48(9):1161–1172. doi: 10.1016/S0277-9536(98)00427-4. [DOI] [PubMed] [Google Scholar]
- Korte J, Bohlmeijer ET, Smit F. Prevention of depression and anxiety in later life: design of a randomized controlled trial for the clinical and economic evaluation of a life-review intervention. BMC Public Health. 2009;9:250. doi: 10.1186/1471-2458-9-250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Korte J, Bohlmeijer ET, Westerhof GJ, Pot AM. Reminiscence and adaptation to critical life events in older adults with mild to moderate depressive symptoms. Aging Ment Health. 2011;15(5):638–646. doi: 10.1080/13607863.2010.551338. [DOI] [PubMed] [Google Scholar]
- Korte J, Bohlmeijer ET, Westerhof GJ, Cappeliez P, Smit F. Life-review therapy for older adults with moderate depressive symptomatology: a pragmatic randomized controlled trial. Psychol Med. 2012;42:1163–1173. doi: 10.1017/S0033291711002042. [DOI] [PubMed] [Google Scholar]
- Krause N. Stressors arising in highly valued roles and the physical health status of older adults. J Gerontol. 2004;59B:S287–S291. doi: 10.1093/geronb/59.5.s287. [DOI] [PubMed] [Google Scholar]
- Krause N. Evaluating the stress-buffering function of meaning in life among older people. J Aging Health. 2007;19:792–812. doi: 10.1177/0898264307304390. [DOI] [PubMed] [Google Scholar]
- Nygren B, Alex L, Jonsen E, Gustafson Y, Norberg A, Lundman B. Resilience, sense of coherence, purpose in life and self-transcendence in relation to perceived physical and mental health among the oldest old. Aging Ment Health. 2005;9(4):354–362. doi: 10.1080/1360500114415. [DOI] [PubMed] [Google Scholar]
- O’Rourke N, Cappeliez P, Claxton A. Functions of reminiscence and the psychological well-being of young–old and older adults over time. Aging Ment Health. 2010;15(2):272–281. doi: 10.1080/13607861003713281. [DOI] [PubMed] [Google Scholar]
- Pearlin LI, Schooler C. The structure of coping. J Health Soc Behav. 1978;19:2–21. doi: 10.2307/2136319. [DOI] [PubMed] [Google Scholar]
- Pinquart M. Creating and maintaining purpose in life in old age: a meta-analysis. Ageing Int. 2002;27(2):90–114. doi: 10.1007/s12126-002-1004-2. [DOI] [Google Scholar]
- Pinquart M, Duberstein PR, Lyness JM. Effects of psychotherapy and other behavioural interventions on clinically depressed older adults: a meta-analysis. Aging Ment Health. 2007;11:645–657. doi: 10.1080/13607860701529635. [DOI] [PubMed] [Google Scholar]
- Pot AM, Bohlmeijer ET, Onrust S, Melenhorst AS, Veerbeek M, De Vries W. The impact of life review on depression in older adults: a randomized controlled trial. Int Psychogeriatr. 2010;22(4):572–581. doi: 10.1017/S104161020999175X. [DOI] [PubMed] [Google Scholar]
- Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1:385–401. doi: 10.1177/014662167700100306. [DOI] [Google Scholar]
- Reker GT. Personal meaning, optimism, and choice: existential predictors of depression in community and institutional elderly. Gerontologist. 1997;37:709–716. doi: 10.1093/geront/37.6.709. [DOI] [PubMed] [Google Scholar]
- Roberts BL, Dunkle R, Haug M. Physical, psychological, and social resources as moderators of the relationship of stress to mental health in the very old. J Gerontol Soc Work. 1994;49:535–543. doi: 10.1093/geronj/49.1.s35. [DOI] [PubMed] [Google Scholar]
- Robitaille A, Cappeliez P, Coulombe D, Webster JD. Factorial structure and psychometric properties of the reminiscence functions scale. Aging Ment Health. 2010;14(2):184–192. doi: 10.1080/13607860903167820. [DOI] [PubMed] [Google Scholar]
- Ryff CD. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J Pers Soc Psychol. 1989;57:1069–1081. doi: 10.1037/0022-3514.57.6.1069. [DOI] [Google Scholar]
- Schieman S, Turner HA. Age, disability and the sense of mastery. J Health Soc Behav. 1998;39:169–187. doi: 10.2307/2676310. [DOI] [PubMed] [Google Scholar]
- Seligman MEP. Learned optimism: how to change your mind and your life. New York: Pocket Books; 1998. [Google Scholar]
- Serrano JP, Latorre JM, Gatz M, Montanes J. Life review therapy using autobiographical retrieval practice for older adults with depressive symptomatology. Psychol Aging. 2004;19:272–277. doi: 10.1037/0882-7974.19.2.272. [DOI] [PubMed] [Google Scholar]
- Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E. The mini-international neuropsychiatric interview (M.I.N.I): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiat. 1998;59:22–33. [PubMed] [Google Scholar]
- Spinhoven PH, Ormel J, Sloekers PPA, Kempen GIJM, Speckens AEM, Van Hemert AM. A validation study of the hospital anxiety and depression scale (HADS) in different groups of Dutch subjects. Psychol Med. 1997;27:363–370. doi: 10.1017/S0033291796004382. [DOI] [PubMed] [Google Scholar]
- Steger M, Frazier P, Oishi S, Kaler M. The meaning in life questionnaire, assessing the presence of and search for meaning in life. J Couns Psychol. 2006;53:80–93. doi: 10.1037/0022-0167.53.1.80. [DOI] [Google Scholar]
- Steunenberg B, Beekman AT, Deeg DJ, Bremmer MA, Kerkhof AJ. Mastery and neuroticism predict recovery of depression in later life. Am J Geriatr Psychiatry. 2007;15(3):234–242. doi: 10.1097/01.JGP.0000236595.98623.62. [DOI] [PubMed] [Google Scholar]
- Taylor SE. Positive illusions: creative self-deception and the healthy mind. New York: Basic Books; 1989. [Google Scholar]
- Taylor SE, Kemeny ME, Reed GM, Bower JE, Gruenewald TL. Psychological resources, positive illusions, and health. Am Psychol. 2000;55(1):99–109. doi: 10.1037/0003-066X.55.1.99. [DOI] [PubMed] [Google Scholar]
- Watt LM (1996) Integrative and instrumental reminiscence therapies for the treatment of depression in older adults. Unpublished Doctoral Dissertation, University of Ottawa
- Webster JD. Construction and validation of the reminiscence functions scale. J Gerontol B. 1993;48:256–262. doi: 10.1093/geronj/48.5.p256. [DOI] [PubMed] [Google Scholar]
- Webster JD, Bohlmeijer ET, Westerhof GJ. Mapping the future of reminiscence: a conceptual guide for research and practice. Res Aging. 2010;32(4):527–564. doi: 10.1177/0164027510364122. [DOI] [Google Scholar]
- West SG, Finch JF, Curran PJ. Structural equation models with non-normal variables. Thousand Oaks: SAGE; 1995. [Google Scholar]
- Westerhof GJ, Bohlmeijer ET. In search of meaning: a reminiscence program for older adults. Educ Gerontol. 2004;30:751–766. doi: 10.1080/03601270490498016. [DOI] [Google Scholar]
- Westerhof GJ, Bohlmeijer ET, Webster JD. Reminiscence and mental health: a review of recent progress in theory, research, and intervention. Ageing Soc. 2010;30:697–721. doi: 10.1017/S0144686X09990328. [DOI] [Google Scholar]
- Westerhof GJ, Bohlmeijer ET, Van Beljouw IMJ, Pot AM. Improvement in personal meaning mediates the effects of a life review intervention on depressive symptoms in a randomized controlled trial. Gerontologist. 2010;50(4):541–549. doi: 10.1093/geront/gnp168. [DOI] [PubMed] [Google Scholar]
- Williams JM, Barnhofer T, Crane C, Herman D, Raes F, Watkins E, Dalgleish T. Autobiographical memory specificity and emotional disorder. Psychol Bull. 2007;133:122–148. doi: 10.1037/0033-2909.133.1.122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wink P, Schiff B. To review or not to review? The role of personality and life events in life review and adaptation to older age. In: Webster JD, Haight BK, editors. Critical advances in reminiscence work: from theory to application. New York: Springer; 2002. pp. 44–60. [Google Scholar]
- Wong PT. Personal meaning and successful aging. Can Psychol. 1989;30(3):516–525. doi: 10.1037/h0079829. [DOI] [Google Scholar]
- Wong PT. The processes of adaptive reminiscence. In: Haight BK, Webster JD, editors. The art and science of reminiscing: theory, research, methods, and applications. Washington, DC: Taylor and Francis; 1995. pp. 23–35. [Google Scholar]
- Wong PT, Watt LM. What types of reminiscence are associated with successful aging? Psychol Aging. 1991;6(2):272–279. doi: 10.1037/0882-7974.6.2.272. [DOI] [PubMed] [Google Scholar]
- Zarit SH, Femia EE, Gatz M, Johansson B. Prevalence, incidence and correlates of depression in the oldest old: the OCTO study. Aging Ment Health. 1999;3(2):119–128. doi: 10.1080/13607869956271. [DOI] [Google Scholar]
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–370. doi: 10.1111/j.1600-0447.1983.tb09716.x. [DOI] [PubMed] [Google Scholar]