

Abstract
Background
Radical prostatectomy is the most common treatment for localised prostate cancer in New Zealand. Active surveillance was introduced to prevent overtreatment and reduce costs while preserving the option of radical prostatectomy. This study aims to evaluate the cost-effectiveness of active surveillance compared to watchful waiting and radical prostatectomy.
Methods
Markov models were constructed to estimate the life-time cost-effectiveness of active surveillance compared to watchful waiting and radical prostatectomy for low risk localised prostate cancer patients aged 45–70 years, using national datasets in New Zealand and published studies including the SPCG-4 study. This study was from the perspective of the Ministry of Health in New Zealand.
Results
Radical prostatectomy is less costly than active surveillance in men aged 45–55 years with low risk localised prostate cancer, but more costly for men aged 60–70 years. Scenario analyses demonstrated significant uncertainty as to the most cost-effective option in all age groups because of the unavailability of good quality of life data for men under active surveillance. Uncertainties around the likelihood of having radical prostatectomy when managed with active surveillance also affect the cost-effectiveness of active surveillance against radical prostatectomy.
Conclusions
Active surveillance is less likely to be cost-effective compared to radical prostatectomy for younger men diagnosed with low risk localised prostate cancer. The cost-effectiveness of active surveillance compared to radical prostatectomy is critically dependent on the ‘trigger’ for radical prostatectomy and the quality of life in men on active surveillance. Research on the latter would be beneficial.
Electronic supplementary material
The online version of this article (doi:10.1186/s12885-017-3522-z) contains supplementary material, which is available to authorized users.
Keywords: Active surveillance, Cost-effectiveness, Low risk localised prostate cancer, Radical prostatectomy
Background
Radical prostatectomy is the most common treatment for patients diagnosed with localised prostate cancer in New Zealand, [1] though it may cause urinary, sexual and gastrointestinal problems [2]. Active surveillance is considered to be a viable alternative for patients with low risk localised prostate cancer, potentially preventing overtreatment and reducing costs while preserving the option of radical prostatectomy [3]. However, men under active surveillance may suffer from physical complications due to the regular investigations such as biopsies, and issues related to living with cancer, including anxiety and depression [4, 5]. The cumulative risk of a radical prostatectomy increases with time under surveillance.
Watchful waiting is mainly used in patients with a life expectancy less than 10 years, but it was included in two randomised clinical trials to compare with radical prostatectomy [6, 7]. The Scandinavian Prostate Cancer Group Study Number 4 (SPCG-4) showed that men treated with radical prostatectomy had fewer local progression cases, metastatic diseases and cancer-specific deaths than men under watchful waiting after 18 years of follow-up [6]. The Prostate Cancer Intervention versus Observation Trial (PIVOT) found no survival difference between the radical prostatectomy group and the observation group [7]. The inconsistent results between the SPCG-4 study and the PIVOT study might be associated with the different studied cohorts and follow-up time: 5% vs 76% of men identified by screening; 36% vs 43% had low risk cancer; the mean age of 65 years vs 67 years; 45% vs 5% had 15 years follow-up [6–9].
No randomised clinical trial with a follow-up over 10 years has been conducted comparing active surveillance and radical prostatectomy. Two published cost-effectiveness studies [10, 11] comparing active surveillance and radical prostatectomy were based on the PIVOT study [7] where most patients were identified by screening. Given the contradictive evidences of benefits and cost-effectiveness of prostate cancer screening [12–16], a new cost-effectiveness study of active surveillance is needed using data of patients identified clinically. The New Zealand Ministry of Health published guidelines on using active surveillance to manage men with low risk prostate cancer in July 2015 [3]. This study aims to evaluate the cost-effectiveness of active surveillance compared to watchful waiting and radical prostatectomy for men diagnosed with low risk localised prostate cancer in New Zealand.
Methods
Ethics
This study was approved by Northern Y (Ref. No. NTY/11/02/019) and Multi-Region Ethics Committees (Ref. No. MEC/11/EXP/044). No inform consent is required for this study.
Model construction
An economic model was constructed, consisting of three Markov models with microsimulation (radical prostatectomy (Additional file 1: Figure S1), active surveillance (Fig. 1) and watchful waiting (Additional file 1: Figure S2)). The cycle length was 1 year per cycle [17]. The model populations were men diagnosed with low risk localised prostate cancer by the D’Amico risk classification system (biopsy Gleason score ≤ 6, clinical stage T1c-T2a and Prostate-specific antigen (PSA) level ≤ 10 ng/mL) at the ages of 45, 50, 55, 60, 65 and 70 years. The simulations ended when the cohort reached the age of 100.
Fig. 1.
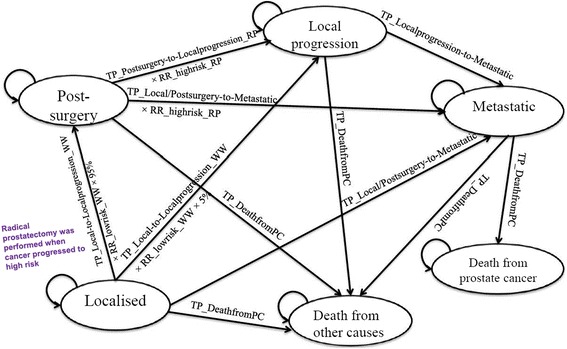
Influence diagram of the Markov model for active surveillance
The health states included ‘Localised’, ‘Post-surgery’, ‘Local progression’, ‘Metastatic’, ‘Death from prostate cancer’ and ‘Death from other causes’ (Fig. 1). In the SPCG-4 study, [6] some men diagnosed with localised prostate cancer in both treatment arms developed metastatic disease in the first year. Therefore, we assumed some metastatic cases were developed directly from ‘Localised’ or ‘Post-surgery’ states. In the active surveillance arm, patients would switch to watchful waiting once they reached 75 years old. When under 75 years old, 95% of them who developed high risk cancer were assumed to be captured and receive radical prostatectomy, and 5% of men were assumed to develop to local progression.
Transition probabilities
The transition probabilities to ‘Local progression’ from ‘Post-surgery’ in the radical prostatectomy arm (Additional file 1: Figure S3) and from ‘Localised’ in the watchful waiting arm were based on the SPCG-4 study published in 2008 [18]. The transition probabilities to metastatic disease were estimated from the results of the SPCG-4 study published in 2008 and in 2014 [6, 18]. The probability of death from metastatic prostate cancer was estimated based on 276 patients [19–21]. The summarised annual transition probabilities are shown in Table 1.
Table 1.
Annual transition probabilities in the economic model
| Transition probability | Description | Transition probabilities (Mean) | SE | Source | ||
|---|---|---|---|---|---|---|
| TP_Local-to-Localprogression_WW | From Localised to Local progression in the watchful waiting arm | 0.0565 | 0.0098 | [18, 30] | ||
| TP_ Postsurgery-to-Localprogression_RP | From Post-surgery to Local progression in the radical prostatectomy arm | 0.0152+0.0012T (T: time (years) from radical prostatectomy) Additional file 1: Figure S3 | Constant: 0.0026; | [18, 30] | ||
| Slope: 0.0004 Variance-covariance matrix: | ||||||
| Slope | Constant | |||||
| Slope | 1.80E-07 | -9.89E-07 | ||||
| Constant | -9.89E-07 | 6.88E-06 | ||||
| TP_Local/Postsurgery-to-Metastatic | From Localised or from Post-surgery to metastases | 0.0075 | 0.0010 | [6, 30] | ||
| TP_Localprogression-to-Metastatic | From Local progression to metastases | 0.0800 | 0.0050 | [6, 30] | ||
| TP_DeathfromPC | From Metastases to death from prostate cancer | 0.3221 | 0.0115 | [19, 21] | ||
| TP_Deathfromothercauses | Death from other causes | New Zealand Period Life Tables: 2010–12 | - | [31] | ||
The probabilities of progression were estimated from a cohort of men with localised prostate cancer. The relative risks of these transition probabilities for low risk, intermediate risk and high risk cancer (Table 2) compared to the localised cancer cohort were estimated based on the proportions of each risk level cancers in the SPCG-4 cohorts [6, 18] and the relative risks of biochemical recurrence for each risk level cancers [22]. They were estimated by dividing the possibilities of biochemical recurrence for low, intermediate and high risk cancer with the overall possibilities in the two arms in the SPCG-4 study, respectively. The calculation was repeated 100,000 times and Gamma distribution fit the result distribution. The annual likelihood of having radical prostatectomy in the active surveillance arm was assumed to be equal to the transition probability from low risk localised prostate cancer to ‘Local progression’ in the watchful waiting group, and that was 1.6%: TP_Local-to-Localprogression_WW (Table 1) × RR_lowrisk_WW (Table 2).
Table 2.
Relative risks of cancer progression for low, intermediate and high risk cancer compared to all localised prostate cancer patients in the SPCG-4 study
| Relative risk | Risk group | Mean | SE | Distribution |
|---|---|---|---|---|
| In the radical prostatectomy arm | ||||
| RR_lowrisk_WW | Low risk | 0.2947 | 0.0100 | Gamma |
| RR_intermrisk_WW | Intermediate risk | 1.0397 | 0.0347 | Gamma |
| RR_highrisk_WW | High risk | 1.9600 | 0.0655 | Gamma |
| In the watchful waiting arm | ||||
| RR_lowrisk_RP | Low risk | 0.3006 | 0.0107 | Gamma |
| RR_intermrisk_RP | Intermediate risk | 1.0606 | 0.0374 | Gamma |
| RR_highrisk_RP | High risk | 1.9993 | 0.0703 | Gamma |
RR relative risk, RP radical prostatectomy, AS active surveillance, WW watchful waiting RR_lowrisk_WW: relative risk of cancer progression for low risk patients compared to localised prostate cancer patients in the watchful waiting arm
Quality of life
The quality of life data in this model are presented in Table 3. The only quality of life data that specifically addressed active surveillance was from Stewart et al. study [23] (mean value: 0.83). Half men included in that study did not have prostate cancer when the study was conducted. This quality of life value was only used in the scenario analysis (please refer to scenario analyses).
Table 3.
EQ-5D based quality of life results for patients at different health states
| Health states | Treatment | Utility | Disutility | SE | Sources |
|---|---|---|---|---|---|
| Post-surgery | Radical prostatectomy | 0.900 | 0.100 | 0.015 | [24] |
| Localised prostate cancer | Watchful waiting | 0.890 | 0.110 | 0.013 | [24] |
| Active surveillance | 0.890 | 0.110 | 0.013 | [24] | |
| Local progression | - | 0.820 | 0.180 | 0.015 | [24] |
| Metastatic prostate cancer: Not last year in life | - | 0.688 | 0.312 | 0.019 | [32, 33] |
| Metastatic prostate cancer: final year of life | - | 0.551 | 0.449 | 0.060 | [34] |
The quality of life data for active surveillance used in our model was based on a study conducted by Korfage et al. [24]. A quality of life value of 0.89 for men before radical prostatectomy was used as the quality of life for men under active surveillance and a quality of life value of 0.90 after radical prostatectomy was used as the quality of life for men after radical prostatectomy in this model. Our Midland Prostate Cancer Study [21] estimated a similar quality of life value (mean value: 0.88) in 42 men who were diagnosed with localised prostate cancer and had radical prostatectomy.
A utility score of 0.820 for patients who received external beam radiotherapy was used for the utility of patients with local progression, because patients diagnosed with locally advanced prostate cancer are mainly treated with radiotherapy and hormone therapy.
Costs
This study was from the perspective of the Ministry of Health in New Zealand, and only direct medical costs were considered. The estimated costs excluded goods and services tax (GST) and were valued in 2012/13 New Zealand dollars (NZ$). A 3.5% discount rate was applied to future costs and utilities.
The treatment costs (Table 4) were based on men enrolled in the Midland Prostate Cancer Project and the Metastatic Prostate Cancer Project [20, 21]. Patients with local progression are treated with radiotherapy and hormone therapy which is similar to the treatment pattern for metastatic prostate cancer. The costs were estimated from the National Non-Admitted Patient Collection (NNPAC), National Minimum Dataset (NMDS) and the Pharmaceutical Information Database (PHARMS). These datasets can be linked through patients’ National Health Index (NHI) numbers that is a unique identifier that is assigned to people who use health and disability support services in New Zealand. NNPAC collects national records for outpatient and emergency department events, NMDS contains clinical data for inpatients and day patients, and PHARMS includes all prescribed and dispensed records for subsidised pharmaceuticals.
Table 4.
Costs of treatment for prostate cancer
| Treatment | Treatment year | Age (Years) | Mean | SE | Patients |
|---|---|---|---|---|---|
| Localised prostate cancer | |||||
| Watchful waiting | First year | All | $323 | $193 | 27 |
| Subsequent years | All | $0 | $0 | - | |
| Active surveillance | First year | All | $980 | $676 | 25 |
| Subsequent years | <75 | $812 | $651 | 18 | |
| ≥75 | $0 | $0 | - | ||
| Radical prostatectomy | First year | All | $13,527 | $422 | 52 |
| Subsequent years | All | $0 | $0 | - | |
| Locally advanced and metastatic cancer | |||||
| First year | <80 | $8,899 | $711 | 145 | |
| Subsequent years | <80 | $6,573 | $789 | 104 | |
| Not last year in life | 80+ | $3,887 | $426 | 40 | |
| Last year in life | 80+ | $3,438 | $502 | 75 | |
Cost-effectiveness analysis
The model construction and data analysis were performed using TreeAge Pro 2015. The model used an outer loop (n = 1000) to capture variation in parameter values, with an inner loop microsimulation considering outcomes for a simulated population (n = 10,000). The costs and utilities for each simulated man were calculated after each Markov cycle by summing the costs and utilities attached to the related health states and transitions in that cycle. The life-time costs and QALYs (quality-adjusted life years) per simulated man in each treatment arm were estimated by averaging the total costs and utilities of all cycles and applying a half cycle correction to all costs (except the costs of ‘Post-surgery’ in the first year after radical prostatectomy) and utilities.
Uncertainty was assessed in all parameters using appropriate distributions. The probability of progression from ‘Post-surgery’ to ‘Local progression’ is based on two parameters, so the Cholesky Decomposition is used. In all other cases, beta distributions were formed for the other transition probabilities. Gamma distributions were similarly formed to model all disutilities (i.e. the difference between 1 and the relevant utility) and for all cost distributions.
Incremental analysis was performed in terms of incremental cost-effectiveness ratio (ICER) by dividing the incremental life-time costs with the incremental life-time utilities. Cost-effectiveness acceptability curves (CEAC) and frontier plots were also constructed to indicate the likelihood of each treatment being cost-effective under a range of willingness-to-pay values (the amount of money willing to pay for a QALY gained) [25].
Scenario analyses
Five scenario analyses were conducted. The first scenario analysis used an annual conversion rate of 5% from active surveillance to radical prostatectomy. The 5% conversion rate was used in the cost model built by Corcoran et al. [26]. Hayes et al. used 0.83 (mean value) as the quality of life after active surveillance and 0.80 (mean value) as the quality of life after treatment without complications in their economic model [10, 27]. These quality of life values were used in the second scenario analysis. The third scenario analysis used an alternative set of cost parameters (Additional file 1: Table S1), which were based on the Waikato District Health Board price list. The fourth scenario analysis used the quality of life data in scenario two and the cost parameters in scenario three. The fifth scenario analysis used all the data in the first three scenarios.
Results
Cost-effectiveness analysis
Across all five age groups, men in the watchful waiting arm had the lowest life-time costs but also the poorest health outcomes in terms of both life years and QALYs (Table 5). Expected life years were similar between the active surveillance and radical prostatectomy arms, while the number of QALYs was slightly lower for active surveillance. The life-time costs of active surveillance were higher than the costs of radical prostatectomy for men diagnosed aged 45–50, but were lower than the costs of radical prostatectomy for men diagnosed at higher ages.
Table 5.
Cost per QALY gained for men with low risk localised prostate cancer
| Age (years) | Life-time outcome | Watchful waiting | Active surveillance | Radical prostatectomy | Incremental analysis |
|---|---|---|---|---|---|
| 45 | Cost (NZ$) | $15,884 | $23,396 | $22,316 | RP vs WW: $6,432 per QALY; |
| Effectiveness (QALYs) | 15.43 | 16.34 | 16.43 | AS was dominated by RP | |
| 50 | Cost (NZ$) | $14,192 | $21,115 | $20,991 | RP vs WW: $7,906 per QALY; |
| Effectiveness (QALYs) | 14.49 | 15.24 | 15.35 | AS was dominated by RP | |
| 55 | Cost (NZ$) | $12,258 | $18,484 | $19,612 | RP vs WW: $10,358 per QALY; AS was extended dominated by WW and RP (AS vs WW: $10,377 per QALY; RP vs AS: $10,255 per QALY) |
| Effectiveness (QALYs) | 13.37 | 13.97 | 14.08 | ||
| 60 | Cost (NZ$) | $10,113 | $15,461 | $18,254 | AS vs WW: $12,155 per QALY; |
| Effectiveness (QALYs) | 12.08 | 12.52 | 12.65 | RP vs AS: $21,485 per QALY | |
| 65 | Cost (NZ$) | $7,843 | $11,998 | $16,972 | AS vs WW: $14,839 per QALY; |
| Effectiveness (QALYs) | 10.62 | 10.90 | 11.05 | RP vs AS: $33,160 per QALY | |
| 70 | Cost (NZ$) | $5,560 | $7,976 | $15,821 | AS vs WW: $17,257 per QALY; |
| Effectiveness (QALYs) | 9.03 | 9.17 | 9.35 | RP vs AS: $43,583 per QALY |
RP radical prostatectomy, AS active surveillance, WW watchful waiting
For younger men (aged 45, 50 or 55 years), radical prostatectomy appeared cost-effective compared to watchful waiting with ICERs of NZ$6432 to NZ$10,358 per QALY gained. Active surveillance was dominated (less effective and more costly) by radical prostatectomy for men aged 40–50 and was extended dominated by watchful waiting and radical prostatectomy for men aged 55.
For men aged 60, active surveillance was cost-effective between willingness-to-pay values of around NZ$12,155–21,485 per QALY. At an indicative figure of NZ$30,000 per QALY, radical prostatectomy appeared cost-effective. However, for men aged 65 and 70, the ranges over which active surveillance was cost-effective included this indicative NZ$30,000 per QALY value (NZ$14,839–33,160 per QALY and NZ$17,257–43,583 per QALY). At much lower willingness-to-pay values (e.g. NZ$10,000 per QALY), radical prostatectomy appeared cost-effective for the youngest patients (aged 45 and 50).
The CEACs (Additional file 1: Figures S4 to S9) also provided useful information as to which option is cost-effective at different values of willingness-to-pay. These figures also highlighted that there remained significant uncertainty as to the choice of the most cost-effective option. In all the models up to 60 years of age, there remained at least 30% likelihood that active surveillance was the most cost-effective option at a figure of NZ$30,000 per QALY. Whilst the possibility of radical prostatectomy being cost-effective increased as higher the willingness-to-pay values rise, this option was no more than 65% likely to be cost-effective in any model even at an unrealistic willingness-to-pay of NZ$100,000 per QALY.
Scenario analyses
The results of five scenario analyses are presented in Table 6. When using the 5% conversion rate (scenario one), the life-time cost of active surveillance increased by 20–36% (aged 70), and the costs of active surveillance were higher than the costs of radical prostatectomy for men aged 45–60 (Additional file 1: Table S2). When using the new quality of life values, the number of QALYs in the active surveillance arm was higher than that in the radical prostatectomy arm in all age groups, and radical prostatectomy was either dominated by active surveillance or extended dominated by active surveillance and watchful waiting. When using new quality of life values, costing values and the 5% conversion rate (scenario five), the ICER of active surveillance compared to watchful waiting increased to NZ$44,090–101,360 per QALY gained. The new costing values (scenario three and four) did not have substantial impact on the results.
Table 6.
Scenario analysis for men with low risk localised prostate cancer
| Age at diagnosis (Years) | ICER (Cost per QALY gained) | Dominance | |||
|---|---|---|---|---|---|
| AS vs WW | RP vs WW | AS vs RP | RP vs AS | ||
| Scenario one: using the 5% conversion rate | |||||
| 45 | - | $6,441 | - | - | AS was dominated by RP |
| 50 | - | $7,908 | - | - | AS was dominated by RP |
| 55 | - | $10,361 | - | - | AS was dominated by RP |
| 60 | - | $14,021 | - | - | AS was dominated by RP |
| 65 | - | $21,226 | - | - | AS was extended dominated by WW and RP |
| 70 | $31,135 | - | - | $33,140 | - |
| Scenario two: using new quality of life inputs | |||||
| 45 | $11,060 | - | - | - | RP was extended dominated by WW and AS |
| 50 | $12,602 | - | - | - | RP was extended dominated by WW and AS |
| 55 | $14,814 | - | - | - | RP was dominated by AS |
| 60 | $17,807 | - | - | - | RP was dominated by AS and by WW |
| 65 | $21,916 | - | - | - | RP was dominated by AS and by WW |
| 70 | $26,833 | - | - | - | RP was dominated by AS and by WW |
| Scenario three: using new costing inputs | |||||
| 45 | - | $5,324 | - | - | AS was dominated by RP |
| 50 | - | $6,613 | - | - | AS was dominated by RP |
| 55 | - | $8,793 | - | - | AS was dominated by RP |
| 60 | - | $12,332 | - | - | AS was extended dominated by WW and RP |
| 65 | $15,732 | - | - | $24,000 | - |
| 70 | $19,364 | - | - | $35,761 | - |
| Scenario four: using new quality of life inputs and costing inputs | |||||
| 45 | $11,254 | - | - | - | RP was extended dominated by WW and AS |
| 50 | $12,882 | - | - | - | RP was extended dominated by WW and AS |
| 55 | $15,248 | - | - | - | RP was extended dominated by WW and AS |
| 60 | $18,520 | - | - | - | RP was dominated by AS and by WW |
| 65 | $23,184 | - | - | - | RP was dominated by AS and by WW |
| 70 | $30,122 | - | - | - | RP was dominated by AS and by WW |
| Scenario five: using new quality of life values, costing values and the 5% conversion rate | |||||
| 45 | $22,904 | - | - | - | RP was extended dominated by WW and AS |
| 50 | $27,385 | - | - | - | RP was extended dominated by WW and AS |
| 55 | $33,790 | - | - | - | RP was extended dominated by WW and AS |
| 60 | $44,090 | - | - | - | RP was dominated by WW |
| 65 | $59,769 | - | - | - | RP was dominated by WW and by AS |
| 70 | $101,360 | - | - | - | RP was dominated by WW and by AS |
RP radical prostatectomy, AS active surveillance, WW watchful waiting
Discussion
Men in the watchful waiting arm had the lowest life-time costs but also the poorest health outcomes in terms of both life years and QALYs. The model in this study yielded similar numbers of life-years between the active surveillance arm and the radical prostatectomy arm, which was consistent with the evidence that active surveillance and radical prostatectomy have similar effects on the survival of men with low risk localised prostate cancer [3, 28].
The life-time costs of active surveillance were lower than the costs of radical prostatectomy for older men, but were higher for younger men. This likely reflects the fact that the longer a person under active surveillance, the greater the risk of ultimately progressing to surgery and the higher costs. In older men the chance of having surgery is smaller, and active surveillance is a more appropriate tool for them. The cost-effectiveness of active surveillance was dependent on the quality of life for men with localised prostate cancer under different treatment options, and the annual probability of having radical prostatectomy in the active surveillance arm.
The triggers of active treatment in the active surveillance arm remain uncertain and different institutions have their own protocols for both biopsy follow-up and defining need to change from active surveillance to radical prostatectomy [29]. Whether or not these reflected existing protocols, a systematic review including data from seven large active surveillance studies reported that up to one-third of men under active surveillance received definitive treatment after a median follow-up of 2.5 years [28]. It was reported that 27–100% men were treated because of histologic reclassification and 13–48% due to PSA doubling time being less than 3 years, while 7–13% of men were treated without evidence of progression [28].
The model in this study assumed active treatment is triggered only when histological progression of the localised prostate cancer is detected, and an annual conversion rate of 1.6% from active surveillance to radical prostatectomy was used. With an annual conversion rate of 1.6%, life-time costs of active surveillance were lower than the costs of radical prostatectomy for men aged 55–70. This conversion rate is ideal rather than realistic under current practice models.
The cost savings for active surveillance existed because radical prostatectomy either does not occur or is likely to occur a significant time into the future. With higher annual conversion rates, prostatectomies become more likely to occur and to occur sooner. The current surveillance costs incurred can outweigh what is saved by pushing the cost of potential prostatectomies into the future, and in this case the life-time costs of active surveillance can outweigh those of a radical prostatectomy. When using the 5% conversion rate, the life-time costs of active surveillance were higher than the costs of radical prostatectomy for men aged 45–60. A study conducted by Hayes et al. [10] showed that the life-time costs of active surveillance were higher than the costs of radical prostatectomy in men aged 65, using a 9% annual rate of conversion. In reality, the annual probability of converting from active surveillance to active treatment might be over 10% [28].
Quality of life data for men under active surveillance and that for men who received radical prostatectomy appeared critical for the cost-effectiveness of active surveillance compared to radical prostatectomy. Unfortunately, there are no good quality of life data for men under active surveillance. Our Midland Prostate Cancer Study [21] had quality of life data on 42 men with radical prostatectomy (average quality of life:0.88, which is close to the value used in the model) but only 3 men with active surveillance. If the quality of life for men under active surveillance is better than that in the radical prostatectomy arm and men in the active surveillance arm would have radical prostatectomy only when high risk cancer was detected, active surveillance might be cost-effective for men at all age groups. Otherwise it might be only cost-effective for older patients.
One of the strengths of this study is that it synthesized data from internationally recognised studies and local costing and outcome data to provide relevant economic information for decision making in New Zealand. This model was based on data of patients mainly identified clinically instead of by screening, which is different from other cost-effectiveness studies. Variations in different age groups were taken into account, which was an advantage compared to other published studies [10, 11, 26]. The entry criteria for active surveillance in the New Zealand guidelines [3] included a life expectancy of greater than 10 years, but patient’s age was not mentioned. The results of this study might have some impact on these guidelines.
This study has some limitations, including the uncertainties on quality of life for men under active surveillance. The quality of life for men at different ages was assumed to be the same if they had identical treatment. In reality, the quality of life may vary by age even under the same treatment. GP costs were not considered in this study. On average the number of PSA tests per prostate cancer patient per year ordered by GPs was only one, which implied that GPs do not play an important role in the on-going management of prostate cancer patients. The model inputs included the costs of short-term complications (included in the first year costs) caused by radical prostatectomy but not the costs of long-term complications. The long-term complications are mainly managed by GPs, and most of the costs are borne by patients and thus were not considered from the perspective of the Ministry of Health. In the active surveillance arm, radical prostatectomy was assumed to be used when cancer progression was detected. Not taking radiation treatment as definitive treatment into account is a limitation of this study.
Conclusion
Active surveillance is less likely to be cost-effective compared to radical prostatectomy for younger men diagnosed with low risk localised prostate cancer. The cost-effectiveness of active surveillance compared to radical prostatectomy is critically dependent on the ‘trigger’ for radical prostatectomy and the quality of life in men on active surveillance.
Early or unnecessary trigger of active treatment reduces the cost-effectiveness of active surveillance. If the quality of life for men under observational management was better than that for men having radical prostatectomy, active surveillance was cost-effective compared to radical prostatectomy, but was not cost-effective compared to watchful waiting for older men with a high annual probability of having radical prostatectomy in the active surveillance arm. More research on these specific points may allow a greater certainty when identifying the optimal management for men with low risk prostate cancer.
Acknowledgements
Not applicable.
Funding
This study was supported by Health Research Council of New Zealand (HRC Partnership Programme grant number 11/082, entitled ‘The costs and complications of screening for prostate cancer’). Chunhuan Lao has been provided with a doctoral scholarship by the New Zealand Ministry of Health.
The funding body was not involved in the design of the study and collection, analysis, interpretation of data, or writing the manuscript.
Availability of data and materials
The data that support the findings of this study are available from the New Zealand Ministry of Health but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the New Zealand Ministry of Health.
Abbreviations
- CEAC
Cost-effectiveness acceptability curves
- GST
Goods and services tax
- ICER
Incremental cost-effectiveness ratio
- NHI
National health index
- NMDS
National minimum dataset
- NNPAC
National non-admitted patient collection
- NZ$
New Zealand dollars
- PHARMS
Pharmaceutical information database
- PIVOT
Prostate cancer intervention versus observation trial
- PSA
Prostate-specific antigen
- QALY
Quality-adjusted life year
- SPCG-4
Scandinavian prostate cancer group study number 4
Additional file
Supporting tables and figures for the cost-effectiveness of active surveillance. (DOCX 889 kb)
Authors’ contributions
CL, RL, RE and PR contributed to the study conception, design and data analyses. CB was involved in data collection and research design. MH and PG provided clinical advice on model construction. All authors were involved in result interpretation, drafting and revising the manuscript. All authors have read and approved the final version of this manuscript.
Ethics approval and consent to participate
Access to the national datasets was approved by the Northern Y (Ref. No. NTY/11/02/019) and Multi-Region Ethics Committees (Ref. No. MEC/11/EXP/044). No consent to participate is needed according to the Rule 10 and Rule 11 of the New Zealand Health Information Privacy Code, 1994.
Consent for publication
Not applicable.
Competing interests
None of the authors have any competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Footnotes
Electronic supplementary material
The online version of this article (doi:10.1186/s12885-017-3522-z) contains supplementary material, which is available to authorized users.
Contributor Information
Chunhuan Lao, Phone: +64 (0)7 837 9485, Email: chunhuan.lao@waikato.ac.nz.
Richard Edlin, Email: r.edlin@auckland.ac.nz.
Paul Rouse, Email: p.rouse@auckland.ac.nz.
Charis Brown, Email: charis@waikato.ac.nz.
Michael Holmes, Email: Michael.Holmes@waikatodhb.health.nz.
Peter Gilling, Email: Peter.Gilling@bopdhb.govt.nz.
Ross Lawrenson, Email: Ross.Lawrenson@waikatodhb.health.nz.
References
- 1.Obertová Z, Lawrenson R, Scott N, Holmes M, Brown C, Lao C, et al. Treatment modalities for Māori and New Zealand European men with localised prostate cancer. Int J Clin Oncol. 2015;20(4):814–820. doi: 10.1007/s10147-014-0781-4. [DOI] [PubMed] [Google Scholar]
- 2.Madalinska JB, Essink-Bot ML, De Koning HJ, Kirkels WJ, Van der Maas PJ, Schröder FH. Health-related quality-of-life effects of radical prostatectomy and primary radiotherapy for screen-detected or clinically diagnosed localized prostate cancer. J Clin Oncol. 2001;19(6):1619–1628. doi: 10.1200/JCO.2001.19.6.1619. [DOI] [PubMed] [Google Scholar]
- 3.Prostate Cancer Working Group and Ministry of Health . Guidance on Using Active Surveillance to Manage Men with Low-risk Prostate Cancer. Wellington: Ministry of Health; 2015. [Google Scholar]
- 4.Korfage IJ, Essink-Bot ML, Janssens ACJW, Schröder FH, De Koning HJ. Anxiety and depression after prostate cancer diagnosis and treatment: 5-Year follow-up. Br J Cancer. 2006;94(8):1093–1098. doi: 10.1038/sj.bjc.6603057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ganeswaran D, Sweeney C, Yousif F, Lang S, Goodman C, Nabi G. Population-based linkage of health records to detect urological complications and hospitalisation following transrectal ultrasound-guided biopsies in men suspected of prostate cancer. World J Urol. 2014;32(2):309–315. doi: 10.1007/s00345-012-0893-2. [DOI] [PubMed] [Google Scholar]
- 6.Bill-Axelson A, Holmberg L, Garmo H, Rider JR, Taari K, Busch C, et al. Radical prostatectomy or watchful waiting in early prostate cancer. N Engl J Med. 2014;370(10):932–942. doi: 10.1056/NEJMoa1311593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wilt TJ, Brawer MK, Jones KM, Barry MJ, Aronson WJ, Fox S, et al. Radical prostatectomy versus observation for localized prostate cancer. N Engl J Med. 2012;367(3):203–213. doi: 10.1056/NEJMoa1113162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bill-Axelson A, Holmberg L, Ruutu M, Häggman M, Andersson SO, Bratell S, et al. Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med. 2005;352(19):1977–1984. doi: 10.1056/NEJMoa043739. [DOI] [PubMed] [Google Scholar]
- 9.Wilt TJ, Brawer MK, Barry MJ, Jones KM, Kwon Y, Gingrich JR, et al. The Prostate cancer Intervention Versus Observation Trial:VA/NCI/AHRQ Cooperative Studies Program #407 (PIVOT): Design and baseline results of a randomized controlled trial comparing radical prostatectomy to watchful waiting for men with clinically localized prostate cancer. Contemp Clin Trials. 2009;30(1):81–87. doi: 10.1016/j.cct.2008.08.002. [DOI] [PubMed] [Google Scholar]
- 10.Hayes JH, Ollendorf DA, Pearson SD, Barry MJ, Kantoff PW, Lee PA, et al. Observation versus initial treatment for men with localized, low-risk prostate cancer: A cost-effectiveness analysis. Ann Intern Med. 2013;158(12):853–860. doi: 10.7326/0003-4819-158-12-201306180-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Koerber F, Waidelich R, Stollenwerk B, Rogowski W. The cost-utility of open prostatectomy compared with active surveillance in early localised prostate cancer. BMC Health Serv Res. 2014;14:163. doi: 10.1186/1472-6963-14-163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Schröder FH, Hugosson J, Roobol MJ, Tammela TLJ, Ciatto S, Nelen V, et al. Prostate-cancer mortality at 11 years of follow-up. N Engl J Med. 2012;366(11):981–990. doi: 10.1056/NEJMoa1113135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hugosson J, Carlsson S, Aus G, Bergdahl S, Khatami A, Lodding P, et al. Mortality results from the Göteborg randomised population-based prostate-cancer screening trial. Lancet Oncol. 2010;11(8):725–732. doi: 10.1016/S1470-2045(10)70146-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Andriole GL, Crawford ED, Grubb RL, Buys SS, Chia D, Church TR, et al. Prostate cancer screening in the randomized prostate, lung, colorectal, and ovarian cancer screening trial: Mortality results after 13 years of follow-up. J Natl Cancer Inst. 2012;104(2):125–132. doi: 10.1093/jnci/djr500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ilic D, O'Connor D, Green S, Wilt TJ. Screening for prostate cancer: An updated Cochrane systematic review. BJU Int. 2011;107(6):882–891. doi: 10.1111/j.1464-410X.2010.10032.x. [DOI] [PubMed] [Google Scholar]
- 16.Lao C, Brown C, Rouse P, Edlin R, Lawrenson R. Economic evaluation of prostate cancer screening: A systematic review. Future Oncol. 2015;11(3):467–477. doi: 10.2217/fon.14.273. [DOI] [PubMed] [Google Scholar]
- 17.Johansson JE, Andrén O, Andersson SO, Dickman PW, Holmberg L, Magnuson A, et al. Natural history of early, localized prostate cancer. JAMA. 2004;291(22):2713–2719. doi: 10.1001/jama.291.22.2713. [DOI] [PubMed] [Google Scholar]
- 18.Bill-Axelson A, Holmberg L, Filén F, Ruutu M, Garmo H, Busch C, et al. Radical prostatectomy versus watchful waiting in localized prostate cancer: The Scandinavian prostate cancer group-4 randomized trial. J Natl Cancer Inst. 2008;100(16):1144–1154. doi: 10.1093/jnci/djn255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lawrenson R, Lao C, Obertová Z, Brown C, Holmes M, Tyrie L, et al. Management and Characteristics of Patients with Metastatic Prostate Cancer in a Cohort of New Zealand Men. Oncology (Switzerland). 2014:157–63. [DOI] [PubMed]
- 20.Lawrenson R, Brown C, Obertova Z, Lao C, Scott N. Final report for the management of metastatic prostate cancer study. New Zealand: Auckland; 2015. https://www.fmhs.auckland.ac.nz/assets/fmhs/som/wcs/docs/2015%20Management%20of%20Men%20with%20Prostate%20Cancer%20-%20FINAL%20REPORT.pdf.
- 21.Lawrenson R, Brown C, Obertova Z, Lao C, Conaglen H. The Midlands Prostate Cancer Study: Understanding the pathways of care for men with localised prostate cancer. Auckland, New Zealand; 2014. https://www.fmhs.auckland.ac.nz/assets/fmhs/som/wcs/docs/FINALREPORTLawrenson11-052.pdf.
- 22.Cooperberg MR, Ramakrishna NR, Duff SB, Hughes KE, Sadownik S, Smith JA, et al. Primary treatments for clinically localised prostate cancer: A comprehensive lifetime cost-utility analysis. BJU Int. 2013;111(3):437–450. doi: 10.1111/j.1464-410X.2012.11597.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Stewart ST, Lenert L, Bhatnagar V, Kaplan RM. Utilities for prostate cancer health states in men aged 60 and older. Med Care. 2005;43(4):347–355. doi: 10.1097/01.mlr.0000156862.33341.45. [DOI] [PubMed] [Google Scholar]
- 24.Korfage IJ, Essink-Bot ML, Borsboom GJJM, Madalinska JB, Kirkels WJ, Habbema JDF, et al. Five-year follow-up of health-related quality of life after primary treatment of localized prostate cancer. Int J Cancer. 2005;116(2):291–6. [DOI] [PubMed]
- 25.Barton GR, Briggs AH, Fenwick EAL. Optimal cost-effectiveness decisions: The role of the cost-effectiveness acceptability curve (CEAC), the cost-effectiveness acceptability frontier (CEAF), and the expected value of perfection information (EVPI) Value Health. 2008;11(5):886–897. doi: 10.1111/j.1524-4733.2008.00358.x. [DOI] [PubMed] [Google Scholar]
- 26.Corcoran AT, Peele PB, Benoit RM. Cost comparison between watchful waiting with active surveillance and active treatment of clinically localized prostate cancer. Urology. 2010;76(3):703–707. doi: 10.1016/j.urology.2009.12.071. [DOI] [PubMed] [Google Scholar]
- 27.Hayes JH, Ollendorf DA, Pearson SD, Barry MJ, Kantoff PW, Stewart ST, Bhatnagar V, Sweeney CJ, Stahl JE, McMahon PM. Active surveillance compared with initial treatment for men with low-risk prostate cancer: A decision analysis. JAMA. 2010;304(21):2373–2380. doi: 10.1001/jama.2010.1720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Dall'Era MA, Albertsen PC, Bangma C, Carroll PR, Carter HB, Cooperberg MR, et al. Active surveillance for prostate cancer: A systematic review of the literature. Eur Urol. 2012;62(6):976–983. doi: 10.1016/j.eururo.2012.05.072. [DOI] [PubMed] [Google Scholar]
- 29.Han CS, Parihar JS, Kim IY. Active surveillance in men with low-risk prostate cancer: current and future challenges. Am J Clin Exp Urol. 2013;1(1):72–82. [PMC free article] [PubMed] [Google Scholar]
- 30.Lao C. Economic evaluation of screening and treatment for prostate cancer in the Midland Cancer Network region in New Zealand. Auckland, New Zealand: The University of Auckland; 2016. [Google Scholar]
- 31.Statistics New Zealand. New Zealand Period Life Tables: 2010–12. Wellington, New Zealand; 2013.
- 32.Wu EQ, Mulani P, Farrell MH, Sleep D. Mapping FACT-P and EORTC QLQ-C30 to patient health status measured by EQ-5D in metastatic hormone-refractory prostate cancer patients. Value Health. 2007;10(5):408–414. doi: 10.1111/j.1524-4733.2007.00195.x. [DOI] [PubMed] [Google Scholar]
- 33.Skaltsa K, Longworth L, Ivanescu C, Phung D, Holmstrom S. Mapping the FACT-P to the preference-based EQ-5D questionnaire in metastatic castration-resistant prostate cancer. Value Health. 2014;17(2):238–244. doi: 10.1016/j.jval.2013.12.005. [DOI] [PubMed] [Google Scholar]
- 34.Färkkilä N, Torvinen S, Roine RP, Sintonen H, Hänninen J, Taari K, et al. Health-related quality of life among breast, prostate, and colorectal cancer patients with end-stage disease. Qual Life Res. 2014;23(4):1387–1394. doi: 10.1007/s11136-013-0562-y. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the New Zealand Ministry of Health but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the New Zealand Ministry of Health.