

Abstract
Background
Psychosocial risks are now widely recognised as one of the biggest challenges for occupational safety and health (OSH) and a major public health concern. The aim of this paper is to investigate the Portuguese long version of the Copenhagen Psychosocial Questionnaire II (COPSOQ II), in order to analyse the psychometric properties of the instrument and to validate it.
Methods
The Portuguese COPSOQ II was issued to a total of 745 Portuguese employees from both private and public organisations across several economic sectors at a baseline and then 2 weeks later. Methodological quality appraisal was based on COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) recommendations. An analysis of the psychometric properties of the long version of COPSOQ II (internal consistency, intraclass correlation coefficient, floor and ceiling effects, response rate, missing values, mean and standard deviation, exploratory factor analysis) was performed to determine the validity and reliability of the instrument.
Results
The COPSOQ II had a response rate of 60.6% (test) and a follow-up response rate of 59.5% (retest). In general, a Cronbach’s alpha of the COPSOQ scales (test and retest) was above the conventional threshold of 0.70. The test-retest reliability estimated by the intraclass correlation coefficient (ICC) showed a higher reliability for most of the scales, above the conventional 0.7, except for eight scales. The proportion of the missing values was less than 1.3%, except for two scales. The average scores and standard deviations showed similar results to the original Danish study, except for eight scales. All of the scales had low floor and ceiling effects, with one exception. Overall, the exploratory factor analysis presented good results in 27 scales assuming a reflective measurement model. The hypothesized factor structure under a reflective model was not supported in 14 scales and for some but not all of these scales the explanation may be a formative measurement model.
Conclusion
The Portuguese long version of COPSOQ II is a reliable and valid instrument for assessing psychosocial risks in the workplace. Although the results are good for most of the scales, there are those that should be evaluated in greater depth in future studies. This instrument may contribute to the promotion of a healthy working environment and workforce, providing clear benefits for companies and employees.
Electronic supplementary material
The online version of this article (doi:10.1186/s12995-017-0170-9) contains supplementary material, which is available to authorized users.
Keywords: Psychosocial risks, Occupational health and safety, Risk assessment (89/391/EEC framework directive), Validation, Portugal
Background
In line with the Europe 2020 objective [1] and the European Union Strategic Framework for Health and Safety at Work 2014–2020 [2], ensuring a healthy and safe working environment contributes considerably to labour productivity and promotes economic growth, competitiveness and welfare [3]. Psychosocial risks are considered the most challenging risk factors across the European Union and a key challenge in modern occupational safety and health (OSH) management, as they are linked not only to health outcomes but also to performance-related outcomes such as absenteeism, ability to work and, in particular, job satisfaction [2, 4]. According to the Framework Directive (89/391/EEC) [5], employers have a legal responsibility to ensure the safety and health of workers in every aspect related to work, including psychosocial risks in the workplace [6].
Although the implementation of these provisions varies from one country to another, the Framework specifies that risks must be identified and assessed, and prevented and managed [7–9]. One of the most important aspects to consider is that risk assessment at work requires the use of valid and reliable methods in order to identify the risk factors in organisations [7, 9–11]. Occupational safety and health legislation therefore places a central focus of risk assessment on preventive approaches [12], which should be considered a priority for organisations [8, 13, 14].
Many measures (mainly questionnaire-based) related to working conditions have been developed, namely the Copenhagen Psychosocial Questionnaire [15, 16], Job Content Questionnaire [17, 18], Effort-Reward Imbalance Questionnaire [19, 20], Pressure Management Indicator [21], Stress Profile [22], Health and Safety Executive Indicator Tool [23], Work Environment Scale [24], General Nordic Questionnaire [25], Job Characteristics Inventory [26], Job Diagnostic Survey [27] and Stress Diagnostic Survey [28], among others, in order to support both employers and employees in the enhancement of OSH processes for prevention and management in organisations [29].
The Copenhagen Psychosocial Questionnaire (COPSOQ) is a comprehensive questionnaire that includes numerous dimensions based on an eclectic set of theories on psychosocial factors at work and on empirical research, rather than being linked to one particular theory [15, 16]. It covers a wide variety of dimensions, describing psychosocial working conditions, and is considered an instrument for research and psychosocial risk prevention in the workplace.
The COPSOQ is an instrument that was developed relatively recently. It was developed in 2000 by Tage S. Kristensen and Vilhelm Borg at the Danish National Research Centre for the Working Environment [15], and revised in 2010 (version II) [16]. In the second version of the Danish COPSOQ study, the psychometric qualities of the instrument were tested in a representative sample of 3517 working Danes between 20 and 59 years of age (52% women, response rate 60.4%). COPSOQ is now one of the most widely used instruments for assessing psychosocial risks in the workplace. It has gained prominent recognition in the scientific community in several countries and has been translated into more than 25 languages, which enables comparison between countries [30, 31]. An increasing number of validation studies have been performed in several countries such as Germany [32, 33], Spain [34], China [35], France [36], Sweden [37], Chile [38] and Iran [39], among others. According to a recent publication by the International Labour Organization [29], the COPSOQ was the first monitoring model to include population-based reference values to assess the need for action and to support the decision-making process concerning preventive measures at the workplace level. Founded in 2009, the COPSOQ International Network (http://www.copsoq-network.org) promotes scientific research and risk assessment using the COPSOQ and aims to facilitate communication between multiple groups. It is therefore linked to governments, universities and research institutions, enterprises and social agents from European and other countries all over the world [40].
The aim of this paper is to present the Portuguese long version of the Copenhagen Psychosocial Questionnaire II (COPSOQ II) and to analyse the psychometric properties of the instrument.
Methods
The validation study was conducted in two phases. In 2013, the original Danish long version of the Copenhagen Psychosocial Questionnaire II (COPSOQ II) was cross-culturally validated [41, 42] and its appraisal based on COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) recommendations [43–46]. The Portuguese version showed satisfactory reliability [47, 48]. Secondly, following implementation of the Portuguese version, data was collected between April 2013 and July 2015 and tested for further psychometric quality. Appraisal was based on COSMIN recommendations concerning the psychometric properties of instruments, which are widely accepted internationally. In this validation study, the following COSMIN domains were evaluated: reliability and factorial validity [43–46]. In addition, we compared our results with the original Danish COPSOQ II study.
Content and structure of the questionnaire
The Portuguese long version of COPSOQ II is a 128-item standardised self-report measure designed for psychosocial risk assessment and prevention. This version has kept the full content and structure of the original Danish long version, in that the 128-item questionnaire consisted of 41 scales reflecting 7 dimensions as outlined in Table 1.
Table 1.
Domains, scales and number of items in the Portuguese long version of COPSOQ II
| Domain | Scale | Number of Items |
|---|---|---|
| Demands at work | Quantitative demands | 4 |
| Work pace | 3 | |
| Cognitive demands | 4 | |
| Emotional demands | 4 | |
| Demands for hiding emotions | 3 | |
| Work organisation and job contents | Influence | 4 |
| Possibilities for development | 4 | |
| Variation | 2 | |
| Meaning of work | 3 | |
| Commitment to the workplace | 4 | |
| Interpersonal relations and leadership | Predictability | 2 |
| Recognition | 3 | |
| Role clarity | 3 | |
| Role conflicts | 4 | |
| Quality of leadership | 4 | |
| Social support from colleagues | 3 | |
| Social support from supervisors | 3 | |
| Social community at work | 3 | |
| Work-individual interface | Job insecurity | 4 |
| Job satisfaction | 4 | |
| Work-family conflict | 4 | |
| Family-work conflict | 3 | |
| Values in the workplace | Mutual trust between employees | 3 |
| Trust regarding management | 4 | |
| Justice | 4 | |
| Social inclusiveness | 4 | |
| Health and well-being | General health perception | 1 |
| Burnout | 4 | |
| Stress | 4 | |
| Sleeping troubles | 4 | |
| Depressive symptoms | 4 | |
| Somatic stress | 4 | |
| Cognitive stress | 4 | |
| Self-efficacy | 6 | |
| Offensive behaviour | Sexual harassment | 1 |
| Threats of violence | 1 | |
| Physical violence | 1 | |
| Bullying | 1 | |
| Unpleasant teasing | 1 | |
| Conflicts and quarrels | 1 | |
| Gossip and slander | 1 | |
| Total | Number of scales 41 | |
| Number of items | 128 |
Most item responses were scored on a five-point Likert scale with five options: always, often, sometimes, seldom, never/hardly ever or to a very large extent, to a large extent, somewhat, to a small extent, to a very small extent. The following items were reverse-scored: “Do you have enough time for your work tasks?”, “Do you have to do the same thing over and over again?”, “How often do you consider looking for work elsewhere?”, “Do employees withhold information from each other?”, “Do employees withhold information from the management?” and “Does the management withhold important information from employees?”.
The scales were calculated as an average of the scores of the items included and transformed to a range of 0 to 100, with high values representing a high level of the concept being measured. The long version of COPSOQ II also includes questions aimed at the sociodemographic characterisation of the participant. The questionnaire takes 30 min to complete. To score the COPSOQ II scales, at least half of the items should be answered for calculating a particular scale [16]. The Portuguese questionnaire is freely available in the public domain as a PDF download from http://www.copsoq.pt/ [49].
Study sample
The study was conducted in 34 companies located in the north and centre of Portugal, between 1 April 2013 and 31 July 2015. It was approved by the Ethics Committee of the University of Porto. After being properly informed about the aim of the study, all of the participants signed the consent form prior to being issued with the questionnaire.
The sample included a total of 745 employees from both private and public organisations across several economic sectors (education, construction, wholesale and retail trade, financial and insurance, manufacturing, human health and social work, other sectors) at the baseline assessment (N = 745). A retest was conducted after two weeks (7–17 days) to assess reproducibility (N = 394). Figure 1 provides details of the participants according to the Classification of Economic Activities. For the current study, we included all workers aged 18 to 65 who were willing to participate in the study and who gave their informed consent.
Fig. 1.
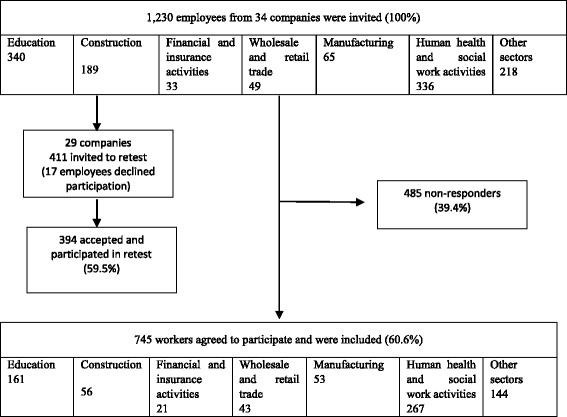
Flow chart showing participation according to the Classification of Economic Activities in the European Union NACE – Rev. 2
The response rate was 60.6%. For test-retest validation, the response rate was 59.5%. The sample size included in this study was based not only on COSMIN recommendations (excellent sample size: ≥ 100), [44] but also on the recommendations of Comrey and Lee [50] and McCullum et al. [51], who recommend more than 640 participants for factor analysis (in this case, based on the number of subjects per item/variable: 5 * 128 = 640), as well as in accordance with the recommendations of the Ethics Committee of the University of Porto.
The sample was classified by different sectors of economic activity according to the nomenclature of the Portuguese Classification of Economic Activities (CAE) Revision 3 (CAE – Rev. 3) [52], which is harmonised with the Classification of Economic Activities in the European Union (NACE – Rev. 2) [53] and the International Standard Classification of Activities, Revision 4 (ISIC – Rev. 4) of the United Nations [54]. The classification used data from Pordata, the Data Base of Contemporary Portugal [55] (Additional file 1).
Overall, the “education” and the “human health and social work activities” sectors of economic activities in our sample are considerably higher than in the general working population. The “construction” and “financial and insurance activities” displayed values very close to the population. Furthermore, the “Other sectors” that were considered (E, J, M, N, O, R, S, T, U), despite covering nine more sectors than expected, also displayed very close values. However, the “wholesale and retail trade” and “manufacturing” sectors of our study show representative values far below those for the population in general, suggesting that they should be confirmed by an appropriate sample in future. The characteristics of the study are shown in Tables 2 and 3. The majority of the participants were female (65.6%). The average age of the respondents was 39 (SD = 9.9), with a range of between 19 and 65. The distribution of organisations between public (n = 300) and private (n = 445) sectors was nearly balanced. Professional groups were classified according to the Portuguese Classification of Occupations [56] and are shown in Table 3. The 2010 Portuguese Classification of Occupations is the most recent international framework (according to the International Standard Classification of Occupations – ISCO 2008) [57].
Table 2.
Characteristics of the study population
| n | % | |
|---|---|---|
| Total participants | 745 | |
| Gender | ||
| Female | 489 | 65.6 |
| Male | 256 | 34.4 |
| Age distribution | ||
| 19–29 | 141 | 19.0 |
| 30–39 | 261 | 35.0 |
| 40–49 | 194 | 26.0 |
| 50–59 | 139 | 18.7 |
| 60–65 | 10 | 1.3 |
| Marital status | ||
| Single | 241 | 32.3 |
| Married | 376 | 50.5 |
| Cohabiting | 62 | 8.3 |
| Divorced | 54 | 7.2 |
| Widowed | 12 | 1.6 |
| Education | ||
| ≤ 9th year | 100 | 13.4 |
| 10th to 12th year | 177 | 23.8 |
| Bachelor | 20 | 2.7 |
| University degree | 318 | 42.7 |
| Postgraduate degree | 1 | 0.1 |
| Master’s degree | 102 | 13.7 |
| PhD | 27 | 3.6 |
| Economic activities | ||
| Manufacturing | 53 | 7.1 |
| Construction | 56 | 7.5 |
| Wholesale and retail trade | 43 | 5.8 |
| Financial and insurance activities | 21 | 2.8 |
| Education | 161 | 21.6 |
| Human health and social work activities | 267 | 35.8 |
| Other sectors | 144 | 19.3 |
| Sectors | ||
| Public | 300 | 40.3 |
| Private | 445 | 59.7 |
Table 3.
Distribution of professionals groups
| Occupation CNP a | n | % |
|---|---|---|
| Management of companies and public administration | 18 | 2.4 |
| Technical and scientific professionals and intellectuals | 341 | 45.8 |
| Technical and associate professionals | 113 | 15.2 |
| Administrative employees | 105 | 14.1 |
| Workers in catering services, personnel, security, etc. | 122 | 16.4 |
| Skilled agricultural and fishery | 0 | 0 |
| Tradespeople and skilled workers in manufacturing | 2 | 0.3 |
| Plant and machine operators, assemblers | 29 | 3.9 |
| Unskilled workers | 14 | 1.9 |
| Missing value | 1 | 0.1 |
| Total | 745 | 100 |
a Portuguese National Classification of Occupations
Study procedure
The procedure was initiated by presenting the study to organisations across several sectors of economic activity. The organisations that were contacted and were available to participate in the study formalised their interest with a signed consent. In every organisation, we tried to cover employees belonging to different hierarchical levels and in different functions in order to ensure that the sample was representative. Data collection activities were developed according to the way each institution worked and in accordance with the dates stipulated in the study.
Data collection included questionnaires available in paper format or as a digital survey. Of the 34 companies in total, digital survey data was collected in three. Before taking part in the digital survey, participants had to meet the following criteria: aged 18 to 65, with each participant having a computer permanently assigned to them for the performance of their duties and willing to participate in the study and to give their informed consent. The COPSOQ II paper format was used and completed in convenient rooms on the organisations’ own premises. The questionnaires were delivered directly to the participants who were supervised while they completed the questionnaire. In the case of the digital survey, the participants filled in an online consent form and completed the online questionnaire. The online questionnaire was made available in order to facilitate data collection, and employees received an email invitation encouraging them to fill out the form at a time and place of their choosing. Employees had 3 weeks to complete the survey and non-respondents received two email reminders during this time. For test-retest validation, similar data collection (paper format or online survey) was conducted after 2 weeks to assess reproducibility. All of the organisations have received a report with a summary of their results.
Psychometric and statistical analysis
Data analysis was performed and included descriptive statistics using mean and standard deviation (SD). The assessment of the psychometric validity of the Portuguese version of the COPSOQ II followed the COSMIN recommendations [43–46] as well as internationally recommended standards [58–61], and included:
-
(i)
the internal consistency of the 41 scales (test and retest) through Cronbach’s alpha;
-
(ii)
test-retest reliability within two weeks was estimated by the intraclass correlation coefficient (ICC) for quantitative variables;
-
(iii)
descriptive statistics comprising mean and standard deviation for all scales;
-
(iv)
floor and ceiling effects;
-
(v)
response rate (test) and follow-up response rate (retest);
-
(vi)
missing values; and
-
(vii)
exploratory factor analysis.
The items in COPSOQ II were analysed using explorative factor analyses within each of the seven major domains: Demands at work; Work organisation and job content; Interpersonal relations and leadership; Work-individual interface; Values at the workplace; Health and well-being and Offensive behaviour.
The assessments of internal consistency and test-retest reliability were performed according to available recommendations [58, 59]. Analysis of internal consistency was undertaken by assessing Cronbach’s alpha. As recommended by Nunnally and Bernstein [60], a Cronbach’s alpha of 0.70 is the threshold value for this assessment. The original Danish study [16] also considered the conventional threshold of 0.70.
For the interpretation of the magnitude of the intraclass correlation coefficient (ICC), an ICC greater than 0.70 was considered adequate [62, 63].
A descriptive statistics (mean and standard deviation) analysis was performed for sociodemographic data and for all 41 scales.
Similar to the original Danish COPSOQ II study, floor and ceiling effects, defined as the proportion of respondents selecting the lowest (floor) and highest (ceiling) response options for all items in a scale, were determined for all scales.
The missing values considered if respondents had answered less than half of the questions in a particular scale, and was analysed for all 41 scales.
Exploratory factor analysis was conducted following a recommendation by the Ethics Committee of the University of Porto. Factorial validity was assessed by definition and evaluation of the factor structure of the instrument using methods of exploratory factor analysis [59, 64, 65]. Models of exploratory factor analysis were defined using principal components analysis for factor extraction [59, 64, 65]. The extraction of the main factors was performed using varimax rotation with Kaiser normalisation. Selection of the number of factors to retain took into account Kaiser’s criterion (eigenvalues greater than one); graphical analysis of the scree plot; a criterion based on the total variance explained (at least greater than 50%); and the Kaiser-Meyer-Olkin (KMO). In the factor analysis, the missing items were handled by using the list-wise deletion method [66]. For all hypothesis tests, a significance level of α = 5% was used. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) v20.0® software program.
Results
A total of 745 employees from 34 companies completed the questionnaire. The average age of the participants was 39 (SD = 9.6). The majority (65.6%) of respondents were female. The participants worked an average of 42.9 h/week (SD = 7.2) and had been in their current jobs for 9.4 years (SD = 9.5) on average. The rate of participation in the test (N = 745) was 60.6%, and in the retest (N = 394) it was 59.5%. The scale characteristics for the dimensions in COPSOQ II are shown in Table 4.
Table 4.
Comparison of the reliability and summary descriptive statistics between the Portuguese (n = 745) and the original COPSOQ II Danish (n = 3517) study sample
| Domain | Scale | Danish | Portuguese | Danish | Portuguese | Danish | Portuguese | Danish | Portuguese | Portuguese | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cronbach’s α n = 3517 |
Cronbach’s α Test n = 745 |
Cronbach’s α Retest n = 394 |
Mean | SD | Mean | SD | % Floor |
% Ceiling |
% Floor |
% Ceiling |
Missing (%) |
Missing N (%) |
Test-retest reliability ICC (95% CI) |
||
| Demands at work | Quantitative demands | 0.82 | 0.69 | 0.67 | 40.2 | 20.5 | 36.3 | 18.2 | 2.9 | 0.3 | 3.6 | 0.3 | 2.2 | 2 (0.3) | 0.818 (0.770–0.859) |
| Work pace | 0.84 | 0.74 | 0.72 | 59.5 | 19.1 | 63.1 | 19.2 | 0.5 | 3.4 | 0.8 | 4.6 | 2.2 | 2 (0.3) | 0.845 (0.804–0.880) | |
| Cognitive demands | 0.74 | 0.63 | 0.71 | 63.9 | 18.7 | 57.0 | 18.4 | 0.3 | 1.1 | 1.1 | 0.9 | 2.2 | 3 (0.4) | 0.778 (0.721–0.828) | |
| Emotional demands | 0.87 | 0.73 | 0.76 | 40.7 | 24.3 | 54.9 | 20.8 | 5.7 | 0.4 | 1.5 | 0.4 | 2.2 | 2 (0.3) | 0.783 (0.727–0.831) | |
| Demands for hiding emotions | 0.57 | 0.60 | 0.62 | 50.6 | 20.8 | 39.7 | 23.3 | 1.5 | 0.9 | 7.0 | 0.8 | 2.3 | 4 (0.5) | 0.719 (0.644–0.784) | |
| Work organisation and job contents | Influence | 0.73 | 0.53 | 0.68 | 49.8 | 21.2 | 47.2 | 19.0 | 1.6 | 0.5 | 1.2 | 0.5 | 2.2 | 3 (0.4) | 0.629 (0.531–0.712) |
| Possibilities for development | 0.77 | 0.71 | 0.73 | 65.9 | 17.6 | 68.7 | 17.0 | 0.4 | 2.3 | 0.3 | 4.4 | 2.6 | 2 (0.3) | 0.810 (0.761–0.852) | |
| Variation | 0.50 | 0.23 | 0.26 | 60.4 | 21.4 | 50.4 | 19.8 | 2.0 | 4.2 | 2.7 | 1.1 | 2.2 | 3 (0.4) | 0.474 (0.324–0.598) | |
| Meaning of work | 0.74 | 0.70 | 0.70 | 73.8 | 15.8 | 75.9 | 17.7 | 0.1 | 7.3 | 0.1 | 15.6 | 2.8 | 2 (0.3) | 0.779 (0.745–0.844) | |
| Commitment to the workplace | 0.76 | 0.61 | 0.71 | 60.9 | 20.4 | 69.5 | 16.4 | 0.7 | 2.2 | 0.1 | 4.7 | 2.2 | 2 (0.3) | 0.521 (0.307–0.628) | |
| Interpersonal relations and leadership | Predictability | 0.74 | 0.50 | 0.62 | 57.7 | 20.9 | 58.6 | 19.5 | 1.5 | 4.2 | 1.2 | 3.0 | 2.3 | 2 (0.3) | 0.736 (0.660–0.799) |
| Recognition | 0.83 | 0.67 | 0.76 | 66.2 | 19.9 | 66.9 | 19.2 | 0.9 | 5.8 | 0.4 | 4.4 | 2.8 | 2 (0.3) | 0.807 (0.755–0.851) | |
| Role clarity | 0.78 | 0.72 | 0.73 | 73.5 | 16.4 | 60.2 | 14.7 | 0.0 | 7.5 | 0.3 | 0.9 | 2.7 | 2 (0.3) | 0.777 (0.717–0.828) | |
| Role conflicts | 0.67 | 0.70 | 0.67 | 42.0 | 16.6 | 44.2 | 19.0 | 1.3 | 0.2 | 1.8 | 0.5 | 2.6 | 3 (0.4) | 0.785 (0.729–0.833) | |
| Quality of leadership | 0.89 | 0.90 | 0.88 | 55.3 | 21.1 | 64.6 | 21.5 | 1.2 | 1.9 | 0.3 | 10.7 | 2.0 | 167a (22.4) | 0.926 (0.903–0.945) | |
| Social support from colleagues | 0.70 | 0.65 | 0.74 | 57.3 | 19.7 | 59.6 | 21.9 | 1.1 | 1.9 | 0.3 | 12.8 | 2.0 | 5 (0.7) | 0.748 (0.748–0.808) | |
| Social support from supervisors | 0.79 | 0.84 | 0.82 | 61.6 | 22.4 | 68.4 | 19.2 | 0.9 | 4.4 | 0.8 | 3.1 | 2.7 | 165b (22.1) | 0.834 (0.780–0.878) | |
| Social community at work | 0.85 | 0.81 | 0.77 | 78.7 | 18.9 | 59.3 | 20.3 | 0.2 | 24.4 | 1.9 | 2.6 | 2.6 | 3 (0.4) | 0.832 (0.787–0.870) | |
| Work-individual interface | Job insecurity | 0.77 | 0.77 | 0.79 | 23.7 | 20.8 | 43.9 | 26.1 | 19.0 | 0.5 | 6.9 | 2.0 | 2.3 | 2 (0.3) | 0.835 (0.793–0.872) |
| Job satisfaction | 0.82 | 0.72 | 0.80 | 65.3 | 18.2 | 62.5 | 16.0 | 0.7 | 5.1 | 0.3 | 3.0 | 2.8 | 3 (0.4) | 0.864 (0.826–0.897) | |
| Work-family conflict | 0.80 | 0.84 | 0.85 | 33.5 | 24.3 | 40.0 | 26.7 | 9.7 | 1.2 | 9.3 | 4.0 | 2.9 | 3 (0.4) | 0.905 (0.880–0.927) | |
| Family-work conflict | 0.79 | 0.76 | 0.88 | 7.6 | 15.3 | 10.7 | 16.9 | 74.6 | 0.2 | 65.4 | 0.4 | 2.9 | 2 (0.4) | 0.792 (0.751–0.842) | |
| Values at the workplace | Mutual trust between employees | 0.77 | 0.66 | 0.65 | 68.6 | 16.9 | 69.0 | 16.6 | 0.0 | 5.6 | 0.1 | 4.7 | 3.2 | 10 (1.3) | 0.752 (0.685–0.809) |
| Trust regarding management | 0.80 | 0.60 | 0.65 | 67.0 | 17.7 | 62.8 | 18.2 | 0.2 | 3.9 | 0.7 | 3.7 | 2.5 | 7 (0.9) | 0.785 (0.729–0.834) | |
| Justice | 0.83 | 0.81 | 0.83 | 59.2 | 17.7 | 61.8 | 18.3 | 0.4 | 1.6 | 0.4 | 3.0 | 2.6 | 7 (0.9) | 0.878 (0.846–0.906) | |
| Social inclusiveness | 0.63 | 0.65 | 0.64 | 67.5 | 16.3 | 59.0 | 20.7 | 0.1 | 3.8 | 0.7 | 2.2 | 2.8 | 8 (1.1) | 0.685 (0.601–0.758) | |
| Health and well-being | General health perception | - | - | - | 66.0 | 20.9 | 58.3 | 22.8 | 0.8 | 14.8 | 1.3 | 9.8 | 1.2 | 0 (0) | 0.820 (0.753–0.869) |
| Burnout | 0.83 | 0.91 | 0.94 | 34.1 | 18.2 | 32.9 | 22.5 | 1.7 | 0.2 | 10.9 | 0.3 | 0.6 | 1 (0.1) | 0.938 (0.922–0.952) | |
| Stress | 0.81 | 0.83 | 0.87 | 26.7 | 17.7 | 43.9 | 22.3 | 5.2 | 0.1 | 4.0 | 1.5 | 0.6 | 1 (0.1) | 0.904 (0.879–0.925) | |
| Sleeping troubles | 0.86 | 0.88 | 0.93 | 21.3 | 19.0 | 38.7 | 21.6 | 17.4 | 0.0 | 5.4 | 0.3 | 0.6 | 2 (0.3) | 0.930 (0.912–0.946) | |
| Depressive symptoms | 0.76 | 0.77 | 0.82 | 21.0 | 16.5 | 32.9 | 22.5 | 10.3 | 0.0 | 10.9 | 0.3 | 0.7 | 1 (0.1) | 0.862 (0.826–0.893) | |
| Somatic stress | 0.68 | 0.70 | 0.78 | 17.8 | 16.0 | 26.9 | 18.9 | 16.6 | 0.0 | 12.2 | 0.3 | 0.6 | 1 (0.1) | 0.843 (0.802–0.878) | |
| Cognitive stress | 0.83 | 0.84 | 0.88 | 17.8 | 15.7 | 31.8 | 18.8 | 18.6 | 0.0 | 5.9 | 0.1 | 0.7 | 1 (0.1) | 0.915 (0.893–0.934) | |
| Self-efficacy | 0.80 | 0.80 | 0.89 | 67.5 | 16.0 | 66.1 | 17.9 | 0.0 | 1.8 | 0.1 | 2.3 | 1.3 | 1 (0.1) | 0.890 (0.862–0.914) | |
| Offensive behaviour | Sexual harassment | - | - | - | 2.9% | - | 0.6% | - | 97.0 | 0.1 | 98.1 | 0.1 | 3.3 | 7 (0.9) | 0.655 (0.526–0.749) |
| Threats of violence | - | - | - | 7.8% | - | 1.5% | - | 92.2 | 0.3 | 95.1 | 0.1 | 3.2 | 8 (1.1) | 0.909 (0.875–0.934) | |
| Physical violence | - | - | - | 3.9% | - | 0.2% | - | 96.1 | 0.0 | 99.2 | 0.8 | 3.3 | 8 (1.1) | 0.888 (0.871–0.903) | |
| Bullying | - | - | - | 8.3% | - | 1.0% | - | 91.7 | 0.5 | 96.7 | 0.1 | 2.5 | 8 (1.1) | 0.562 (0.399–0.681) | |
| Unpleasant teasing | - | - | - | 8.3% | - | 5.2% | - | 91.7 | 0.3 | 82.5 | 0.3 | 3.2 | 7 (0.9) | 0.813 (0.743–0.864) | |
| Conflicts and quarrels | - | - | - | 51.2% | - | 5.8% | - | 48.8 | 1.3 | 79.9 | 0.4 | 2.5 | 7 (0.9) | 0.683 (0.564–0.769) | |
| Gossip and slander | - | - | - | 38.9% | - | 5.3% | - | 61.1 | 3.5 | 83.6 | 0.8 | 2.6 | 7 (0.9) | 0.658 (0.531–0.751) | |
a Most cases are “not applicable” rather than there being “no answers” from participants. The data results of the “non-answers” and not applicable are the following for the two scales: Quality of leadership [no answers n = 10; not applicable n = 157] and Social support from supervisors [no answers n = 9; not applicable n = 156]
For 29 of the 41 scales, Cronbach’s alpha was generally above the conventional threshold of 0.70, nine scales ranged between 0.60 and 0.70, and three scales had a reliability of less than 0.60 (Influence at work, Variation and Predictability). Test-retest reliability was assessed by examining the correlation of the scale score in the baseline long version of the COPSOQ II questionnaire with the COPSOQ II questionnaire scale score completed 2 weeks after the baseline assessment. According to the adopted criteria for the interpretation of the magnitude of the ICC (> 0.70), this analysis indicated an acceptable reliability for 33 out of 41 scales. For the eight scales where we had ICC values of less than 0.70, five of them had very close values and three were indicative of poor reliability.
The average scores and standard deviations showed similar results to the original Danish study [16]. However, the average scores showed moderate differences in eight scales [Demand for hiding emotions (Portugal = 39.7, Denmark = 50.6), Social support from supervisors (Portugal = 68.4, Denmark = 61.6), Social community at work (Portugal = 59.3, Denmark = 78.7), Stress (Portugal = 43.9, Denmark = 26.7), Sleeping troubles (Portugal = 38.7, Denmark = 21.3), Depressive symptoms (Portugal = 32.9, Denmark = 21.0), Somatic stress (Portugal = 26.9, Denmark = 17.8) and Cognitive stress (Portugal = 31.8, Denmark = 17.8)] and very significant differences in three scales [Job insecurity (Portugal = 43.9, Denmark = 23.7), Conflicts and quarrels (Portugal = 5.8%, Denmark = 51.2) and Gossip and slander (Portugal = 5.3%, Denmark = 38.9)]. These verified differences are positive and negative, depending on each case.
Most of the scales had low floor and ceiling effects, except Family–work conflict, which had a high floor effect (65.4%).
For 39 of the 41 scales in the long questionnaire, the percentage of missing values was less than 1.3% (0.1–1.3%). Two scales had high values [Quality of leadership (22.4%) and Social support from supervisors (22.1%)] although most cases are not applicable rather than there being no answers from participants.
An exploratory factor analysis was conducted considering the seven dimensions of the long version of the COPSOQ II, and the results are summarized in Tables 5, 6, 7, 8, 9, 10, 11.
Table 5.
Exploratory factor analysis of items in the Demands at work dimension (n = 700) of COPSOQ II (long version): loadings for each factor and each item in the scale after varimax rotation and factor extraction using principal components
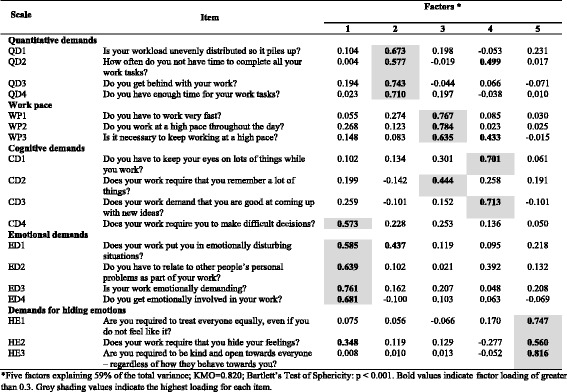
*Five factors explaining 59% of the total variance; KMO = 0.820; Bartlett’s Test of Sphericity: p < 0.001. Bold values indicate factor loading of greater than 0.3. Grey shading values indicate the highest loading for each item
Table 6.
Exploratory factor analysis of items in the Work organisation and job contents dimension (n = 699) of COPSOQ II (long version): loadings for each factor and each item in the scale after a varimax rotation and factor extraction using principal components
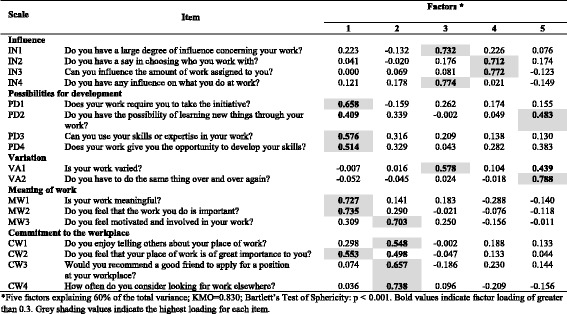
*Five factors explaining 60% of the total variance; KMO = 0.830; Bartlett’s Test of Sphericity: p < 0.001. Bold values indicate factor loading of greater than 0.3. Grey shading values indicate the highest loading for each item
Table 7.
Exploratory factor analysis of items in the Interpersonal relations and leadership dimension (n = 516) of COPSOQ II (long version): loadings for each factor and each item in the scale after a varimax rotation and factor extraction using principal components
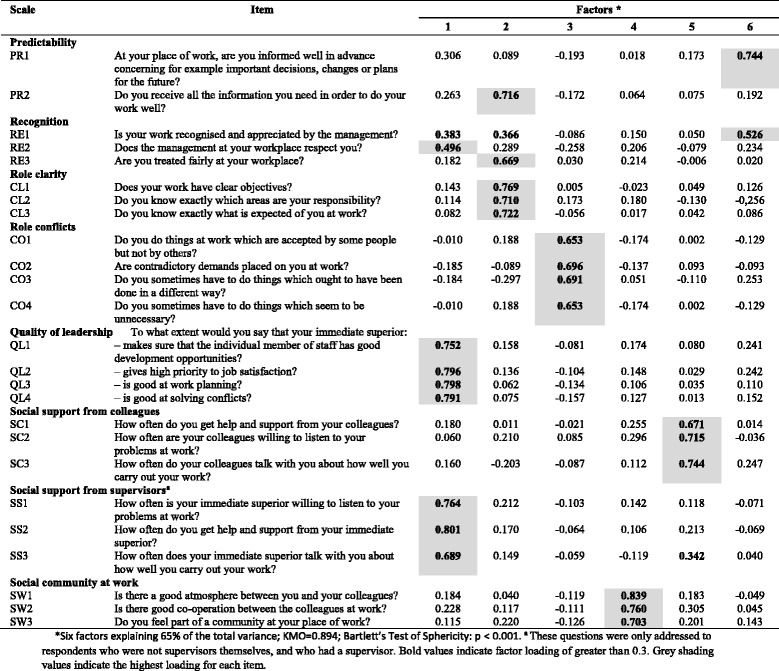
*Six factors explaining 65% of the total variance; KMO = 0.894; Bartlett’s Test of Sphericity: p < 0.001. a These questions were only addressed to respondents who were not supervisors themselves, and who had a supervisor. Bold values indicate factor loading of greater than 0.3. Grey shading values indicate the highest loading for each item
Table 8.
Exploratory factor analysis of items in the Work-individual interface dimension (n = 704) of COPSOQ II (long version): loadings for each factor and each item in the scale after a varimax rotation and factor extraction using principal components
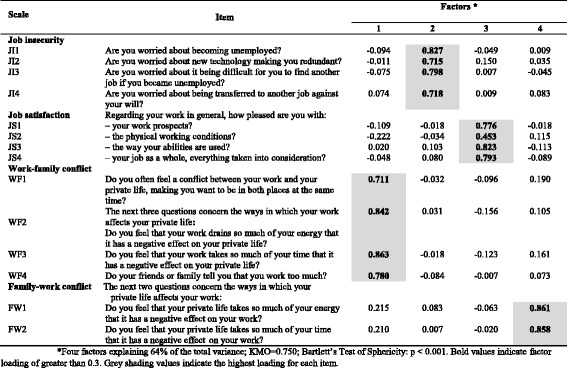
*Four factors explaining 64% of the total variance; KMO = 0.750; Bartlett’s Test of Sphericity: p < 0.001. Bold values indicate factor loading of greater than 0.3. Grey shading values indicate the highest loading for each item
Table 9.
Exploratory factor analysis of items in the Values at the workplace dimension (n = 683) of COPSOQ II (long version): loadings for each factor and each item in the scale after a varimax rotation and factor extraction using principal components
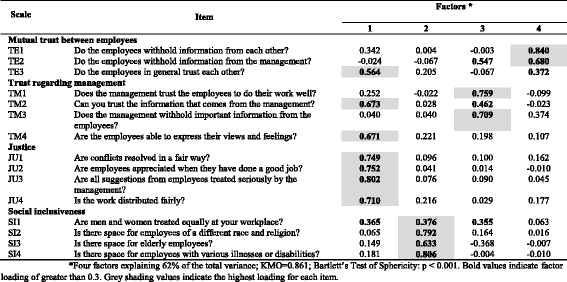
*Four factors explaining 62% of the total variance; KMO = 0.861; Bartlett’s Test of Sphericity: p < 0.001. Bold values indicate factor loading of greater than 0.3. Grey shading values indicate the highest loading for each item
Table 10.
Exploratory factor analysis of items in the Health and well-being dimension (n = 694) of COPSOQ II (long version): loadings for each factor and each item in the scale after a varimax rotation and factor extraction using principal components
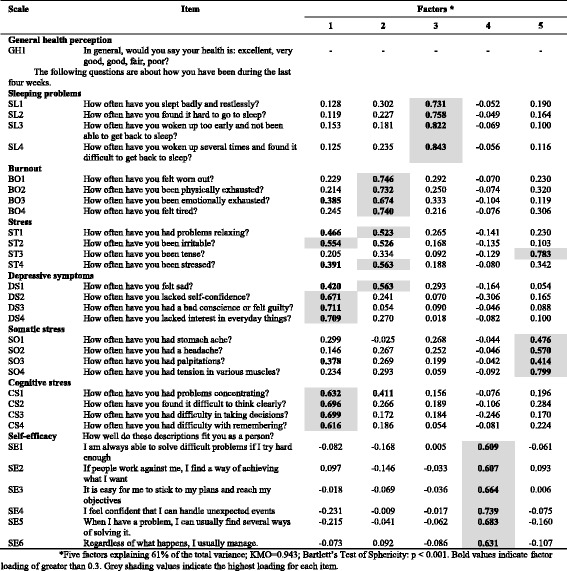
*Five factors explaining 61% of the total variance; KMO = 0.943; Bartlett’s Test of Sphericity: p < 0.001. Bold values indicate factor loading of greater than 0.3. Grey shading values indicate the highest loading for each item
Table 11.
Exploratory factor analysis of items in the Offensive behaviour dimension (n = 729) of COPSOQ II (long version): loadings for each factor and each item in the scale after a varimax rotation and factor extraction using principal components
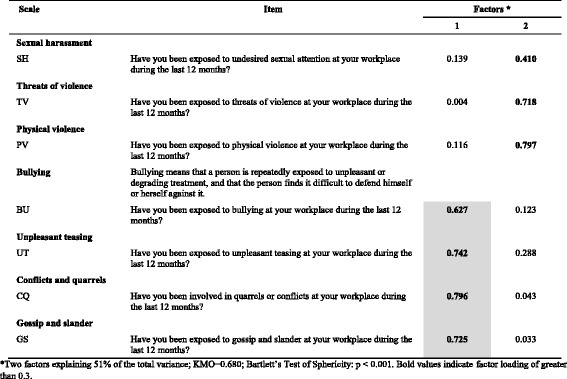
*Two factors explaining 51% of the total variance; KMO = 0.680; Bartlett’s Test of Sphericity: p < 0.001. Bold values indicate factor loading of greater than 0.3
In the Demands at work dimension, the results support the scales (Quantitative demands, Work pace, Emotional demands and Demands for hiding emotions). However, items in the scale of Cognitive demands have the highest loadings on three different factors, indicating that the construct validity of this scale is not supported (Table 5).
In the Work organisation and Job Contents dimension, the results support the Commitment to the workplace scale. Items in the Influence scale are split into two factors (one factor concerning influence in general and concerning what you do, and one factor concerning influence on who you work with and the amount of work). In the scale concerning Possibilities for development, one item loads on factor 5 rather than factor 1. In the Variation scale, one item loads on factor 5 while the other item loads highest on factor 3, together with two items concerning Influence. In the Meaning of work scale, one item loads highest on factor 2, together with the items on Commitment to the workplace (Table 6).
In the Interpersonal relations and leadership dimension (Table 7), the results support the Role clarity, Role conflict, Social support from colleagues and Social community at work scales. Two scales (Quality of leadership and Social support from supervisors) load on the same factor. Two other scales (Predictability and Recognition) load on several factors.
In the Work-individual interface dimension, the results support the hypothesised scale structure (Table 8).
In the Values at the workplace dimension, the results support the hypothesised scale structure for two scales (Justice and Social inclusiveness), while the other two scales are split between several factors (Table 9).
In the Health and well-being dimension, the results support the hypothesised scale structure for five scales (Sleeping problems, Burnout, Somatic stress, Cognitive stress and Self-efficacy). The stress scale is split into several factors. In the Depressive symptoms scale, DS1 loads strongest on factor 2 (Table 10).
In the Offensive behaviour dimension (Table 11), the results support the Bullying, Unpleasant teasing, Conflict and quarrels and Gossip and slander scales. The other three scales load on factor 2 rather than factor 1.
The results of the exploratory factor analysis showed that, from the 41 total scales, 27 support the hypothesised scale structure while the factor results differ from the scale structure for 14 scales (Cognitive demands, Influence, Possibilities for development, Variation, Meaning of work, Predictability, Recognition, Mutual trust between employees, Trust between management, Stress, Depressive symptoms, Sexual harassment, Threats of violence and Physical violence).
Discussion
This paper described the Portuguese validation of the long version of COPSOQ II using rigorous methodology based on both psychometric and conceptual criteria.
In general, a Cronbach’s alpha of the COPSOQ scales (test and retest) indicated acceptable reliability (0.7). Furthermore, the fact that Cronbach’s alpha is influenced by the number of items in the scale explains the findings of lower values of alphas.
The test-retest reliability results indicate that most of the scales showed good temporal stability and reliability in the considered time interval. However, there were eight scales that showed ICC values below 0.7 (Influence, Variation, Commitment to the workplace, Social inclusiveness, Sexual harassment, Bullying, Conflicts and quarrels and Gossip and slander). Out of these eight four belonged to the offensive behaviour dimension, three to belonged to the Work organisation and job contents and the remaining one to the Values at workplace dimension.
The three scales concerning the Variation, Commitment to the workplace and Bullying showed poor ICC values. The reason for the poor test-retest reliability should be evaluated in future studies.
The test-retest design showed a good reliability for most of the scales, namely where Cronbach’s alpha was low, as reported in a previous study by Thorsen and Bjorner [67]. These authors examined the reliability of the COPSOQ work environment questionnaire and have concluded that the test-retest design and intraclass correlation appears to be more appropriate than Cronbach’s alpha for assessing the reliability of COPSOQ’s psychosocial work environment scales.
Thorsen and Bjorner [67] specified assumptions for 26 COPSOQ scales, eight of each were assumed to exhibit a reflective model (internal consistency) and 18 were assumed to exhibit a formative model.
The exploratory factor analysis findings assumed that from the 41 total scales, 27 are based on a reflective model of effect indicators, in which all of the items are a manifestation of the same underlying construct [46, 68, 69]. The remaining 14 scales did not show a clear factor in the exploratory factor analysis. Out of these, three (Meaning of work, Stress and Depressive symptoms) cannot be assumed to exhibit the formative model, since they had previously been assumed to exhibit a reflective measurement model, as reported by Thorsen and Bjorner [67]. Future studies should evaluate these three scales in greater depth.
The remaining 11 scales assumed to exhibit a formative model in which items are combined due to their hypothesised common effect rather than their common cause. High inter-item correlation is not a necessary criterion of construct validity and these do not need to be correlated [46, 67, 70, 71].
Following this line of thinking, as Thorsen and Bjorner [67] also state, Cronbach’s alpha might not be a good measure of reliability for these scales because it might underestimate true reliability. In this circumstance, the internal consistency is not considered relevant for items that form a formative model [46, 70–74].
In accordance with these findings, the authors Bjorner and Pejtersen [75] argue that the traditional psychometric techniques (e.g. factor analysis and reliability through Cronbach’s alpha) may not be appropriate for some COPSOQ II scales for which the items are combined based on a hypothesised common effect rather than a hypothesised common cause.
As quoted in their work [75] “Bollen pointed out that not all questionnaires scales can be conceived as consisting of effect indicator items, being that some items must be seen as causes of the latent construct rather than effects” [70, 71].
These insights can help to explain the apparently “inconsistent” findings that were reported in some of the results of the exploratory factor analysis.
The average scores and standard deviations showed similar results to the original Danish study, except for 11 scales, which may be explained by the context of unstable labour markets and the significant increase in employees’ feeling of job insecurity (e.g. fear of being hampered in the performance of their function or in their career development and even of losing their job) and the resulting negative impact on employees’ health and well-being. As for the floor and ceiling effect, we observed similar results to the original Danish study. The Family-work conflict scale showed a high floor effect (65.4%) and a very low mean value (10.7). In accordance with the original authors, this result also indicates that private life is not interfering with work in general.
As for the missing items, in 39 out of the total of 41 scales, the missing items are less than 1.3%. A higher proportion of missing values observed in two scales (Quality of leadership and Social support from supervisors) should be interpreted cautiously due to the fact that most cases are “not applicable” questions rather than “no answers” from the participants.
The Portuguese COPSOQ II had a moderate response rate of 60.6% for the baseline test (n = 745) and a good follow-up rate of 59.5% for the retest (N = 394).
Several strengths of this study need to be mentioned. Firstly, the inclusion of international statistical standards enables reliable and comparable national, European and international statistics. In line with this, validation of the long version of COPSOQ II, maintaining its full content and structure, also enables statistics comparable to those of other countries.
Secondly, the adoption of COSMIN methodology, internationally widely accepted recommendations for the assessment of psychometric characteristics, is aimed at ensuring the quality of results. Thirdly, the inclusion of various sectors of economic activity, taking into consideration workers at different hierarchical levels and in different functions in each company, ensured greater confidence in the results.
There were some limitations to the study. Firstly, the study sample in the Wholesale and retail trade and Manufacturing sectors of economic activity should be improved. Secondly, the online survey data collection had lower response rates than the paper-based ones. Thirdly, the current economic crisis could have an impact on the answers that people give to some of the questions.
Conclusion
Most scales in the Portuguese long version of the COPSOQ II were found to be valid and reliable for the evaluation and study of the implications of psychosocial work factors for the health and well-being of workers. Three scales need further evaluation since the hypothesized factor structure was not supported (Meaning of work, Stress, and Depressive symptoms) while three other scales should be further evaluated due to low reliability in test-retest analyses (Variation, Commitment to the workplace, and Bullying).
The Framework Directive (89/391/EEC) confers a central place in risk assessment to preventive approaches and highlights the use of valid and reliable methods in order to identify all types of risk factors in organisations, with psychosocial risk management being the employers’ responsibility. This line of approach establishes the importance of integrated prevention, taking an increasing number of risk factors into consideration and including all aspects of psychosocial risks (e.g. demands at work, work-individual interface, work organisation and job contents, offensive behaviour, etc.). This tool is intended to be a resource for researchers and professionals in Portuguese organisations for the prevention and promotion of health and well-being in the labour context and also to promote the development of a national culture of prevention, in particular as regards psychosocial risk factors.
In future research, gradual use of the COPSOQ in various economic activities will lead to a broader database, thereby allowing researchers and professionals to adjust validation analyses (in particular the scales that indicated less satisfactory results), establish comparisons between companies and advance in the development of Portuguese standards.
Acknowledgments
We would like to thank all the employees who agreed to participate in the study.
Funding
This study received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Availability of data and materials
The data are available by contacting the author: Susel Rosário: e-mail: skrosario@gmail.com
Abbreviations
- BGW
Institute for statutory accident insurance and prevention in the health and welfare services
- CAE – Rev. 3
Portuguese classification of economic activities – revision 3
- CIDES
Department of health information and decision sciences
- CINTESIS
Centre for research in health technologies and information systems and information and decision sciences department
- COPSOQ II
Copenhagen Psychosocial Questionnaire II
- COSMIN
COnsensus-based standards for the selection of health measurement instruments
- CUF
Companhia União Fabril
- Cvcare
Center of excellence for epidemiology and health service research for healthcare professionals
- EUROSTAT
Statistical office of the european communities
- FFAW GmbH
Freiburg research centre for occupational sciences
- GPR
Principles of prevention and rehabilitation department
- ICC
Intraclass correlation coefficient
- ISCO
International standard classification of occupations
- ISIC – Rev. 4
International standard classification of activities – revision 4
- IVDP
Institute for health services research in dermatology and nursing
- KMO
Kaiser-Meyer-Olkin
- LAETA
Associated laboratory for energy, transport and aeronautics
- NACE – Rev. 2
Classification of economic activities in the european union – revision 2
- NOPain
National observatory of pain
- OECD
Organisation for Economic Co-operation and Development
- OSH
Occupational Safety and Health
- PORDATA
The data base of contemporary Portugal
- SD
Standard deviation
- SPSS
Statistical package for the social sciences
Additional file
Portuguese Classification of Economic Activities (CAE) – Revision 3 (CAE – Rev. 3) according to Pordata (2013). (DOCX 16 kb)
Authors’ contributions
SR, LFA, JAF, AN, MN and JTC have made substantial contributions to this study. All of the authors approved and critically reviewed the final version of the manuscript.
Ethics approval and consent to participate
The study was approved by Ethics Committee of the University of Porto (Parecer N° 16/CEUP/2013). All participants gave their informed written consent.
Consent for publication
No details on individuals are reported within the manuscript.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Footnotes
Electronic supplementary material
The online version of this article (doi:10.1186/s12995-017-0170-9) contains supplementary material, which is available to authorized users.
References
- 1.European Commission. Europe 2020: A European Strategy for Smart, Sustainable and Inclusive Growth. Communication from the Commission COM(2010) 2020 Final. Brussels: European Commission; 2010. doi:10.1016/j.resconrec.2010.03.010.
- 2.European Commission . Communication from the commission to the European Parliament, the council, the European economic and social committee and the Committee of the Regions on an EU strategic framework on health and safety at work 2014–2020. Brussels: European Commission; 2014. [Google Scholar]
- 3.European Foundation for the Improvement of Living and Working Conditions (Eurofound) European Agency for Safety and Health at Work (EU-OSHA) Psychosocial risks in Europe: prevalence and strategies for prevention. Luxembourg: Publications Office of the European Union; 2014. [Google Scholar]
- 4.EU-OSHA . Estimating the cost of accidents and ill-health at work – a review of methodologies. Luxembourg: Publications Office of the European Union; 2014. [Google Scholar]
- 5.European Commission . Official journal of the European Communities, L183, 29/06/1989. 1989. Council directive 89/391/EEC - OSH “framework directive.”. [Google Scholar]
- 6.European Commission . Employment, social affairs and inclusion. 2014. Interpretative document of the implementation of council directive 89/391/EEC in relation to mental health in the workplace. [Google Scholar]
- 7.European Commission . Guidance on risk assessment at work. Luxembourg: Publications Office of the European Union; 1996. [Google Scholar]
- 8.International Labour Office . ILO guidelines on occupational safety and health management systems. Geneva: International Labour Office; 2001. [Google Scholar]
- 9.Stravoula L, Cox T. The European framework for psychosocial risk management: PRIMA-EF. Nottingham: World Health Organization; 2008. [DOI] [PubMed] [Google Scholar]
- 10.Nübling M, Vomstein M, Haugh A, Nübling T, Adiwidjaja A. European-wide survey on teachers work related stress - assessment, comparison and evaluation of the impact of psychosocial hazards on teachers at their workplace. Brussels: European Trade Union Committee for Education; 2011. [Google Scholar]
- 11.Rosário S, Fonseca J, Nienhaus A, Torres da Costa J. Standardized assessment of psychosocial factors and their influence on medically confirmed health outcomes in workers: a systematic review. J Occup Med Toxicol. 2016;11:19. doi: 10.1186/s12995-016-0106-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.EU-OSHA . The second European survey of enterprises on new and emerging risks (ESENER-2) Luxembourg: Publications Office of the European Union; 2015. [Google Scholar]
- 13.International Labour Office . SOLVE integrating health promotion into workplace OSH policies: Trainer’s guide. Geneva: International Labour Office; 2012. [Google Scholar]
- 14.International Labour Office . World day for safety and health at work, 28 April 2010. Geneva: International Labour Office; 2010. Emerging risks and new patterns of prevention in a changing world of work. [Google Scholar]
- 15.Kristensen TS, Hannerz H, Høgh A, Borg V. The Copenhagen psychosocial questionnaire—a tool for the assessment and improvement of the psychosocial work environment. Scand J Work Environ Health. 2005;31(6):438–449. doi: 10.5271/sjweh.948. [DOI] [PubMed] [Google Scholar]
- 16.Pejtersen JH, Kristensen TS, Borg V, Bjorner JB. The second version of the Copenhagen psychosocial questionnaire. Scand J Public Health. 2010;38(3 Suppl):8–24. doi: 10.1177/1403494809349858. [DOI] [PubMed] [Google Scholar]
- 17.Karasek RA. Job demands, job decisions latitude and mental strain: implications for job redisign. Adm Sci Q. 1979;24:285–307. doi: 10.2307/2392498. [DOI] [Google Scholar]
- 18.Johnson JV, Hall EM. Job strain, work place social support, and cardiovascular disease: a cross-sectional study of a random sample of the Swedish working population. Am J Public Health. 1988;78(10):1336–1342. doi: 10.2105/AJPH.78.10.1336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Siegrist J. Adverse health effects of high-effort / low-reward conditions. J Occup Health Psychol. 1996;1(1):27–41. doi: 10.1037/1076-8998.1.1.27. [DOI] [PubMed] [Google Scholar]
- 20.Siegrist J, Starke D, Chandola T, et al. The measurement of effort-reward imbalance at work: European comparisons. Soc Sci Med. 2004;58(8):1483–1499. doi: 10.1016/S0277-9536(03)00351-4. [DOI] [PubMed] [Google Scholar]
- 21.Williams S, Cooper CL. Measuring occupational stress: development of the pressure management indicator. J Occup Health Psychol. 1998;3(4):306–321. doi: 10.1037/1076-8998.3.4.306. [DOI] [PubMed] [Google Scholar]
- 22.Setterlind S, Larsson G. The stress profile: a psychosocial approach to measuring stress. Stress Med. 1995;11(2):85–92. doi: 10.1002/smi.2460110116. [DOI] [Google Scholar]
- 23.Cousins R, Mackay C, Clarke S, Kelly C, Kelly P, McCaig R. Management standards and work-related stress in the UK: practical development. Work Stress. 2004;18:113–136. doi: 10.1080/02678370410001734322. [DOI] [Google Scholar]
- 24.Moos R. The work environment scale manual. 3. Palo Alto: Consulting Psychologists Press; 1994. [Google Scholar]
- 25.Elo A-L, Skogstad A, Dallner M, Gamberale F, Hottinen V, Knardahl S. User’s Guide for the QPSNordic: General Nordic Questionnaire for Psychological and Social Factors at Work. (2000:603 T, ed.). Copenhagen: Nordic Council of Ministers; 2000.
- 26.Sims H, Szilagyi A, Keller R. The measurement of job characteristics. Acad Manag J. 1976;19(2):195–212. doi: 10.2307/255772. [DOI] [PubMed] [Google Scholar]
- 27.Hackman JR, Oldham GR. Development of the job diagnostic survey. J Appl Psychol. 1975;60(2):159–170. doi: 10.1037/h0076546. [DOI] [Google Scholar]
- 28.Ivancevich M, Matteson T. Stress and work. Glenview, IL: Scott, Foresman and Company; 1980. [Google Scholar]
- 29.International Labour Office . World day for safety and health at work 28 April 2016. Geneva: International Labour Office; 2016. Workplace stress: a collective challenge. [Google Scholar]
- 30.Kristensen TS. A questionnaire is more than a questionnaire. Scand J Public Health. 2010;38(3 Suppl):149–155. doi: 10.1177/1403494809354437. [DOI] [PubMed] [Google Scholar]
- 31.Nübling M, Burr H, Moncada S, Kristensen TS. COPSOQ international network: Co-operation for research and assessment of psychosocial factors at work. Public Health Forum. 2014;22(1). doi:10.1016/j.phf.2013.12.019.
- 32.Nübling M, Stößel U, Hasselhorn H-M, Michaelis M, Hofmann F. Measuring psychological stress and strain at work - Evaluation of the COPSOQ Questionnaire in Germany. Psychosoc Med. 2006;3:Doc05. http://www.ncbi.nlm.nih.gov/pubmed/19742072%5Cn, http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC2736502. [PMC free article] [PubMed]
- 33.Nübling M, Stößel U, Hasselhorn H, Michaelis M, Hofmann F. Methoden Zur Erfassung Psychischer Belastungen - Erprobung Eines Messinstrumentes (COPSOQ) 2005. [Google Scholar]
- 34.Moncada S, Utzet M, Molinero E, et al. The copenhagen psychosocial questionnaire II (COPSOQ II) in Spain-a tool for psychosocial risk assessment at the workplace. Am J Ind Med. 2014;57(1):97–107. doi: 10.1002/ajim.22238. [DOI] [PubMed] [Google Scholar]
- 35.Shang L, Ping L, Lin-bo F, Hua-kang G, Jian L. Psychometric properties of the Chinese version of Copenhagen psychosocial questionnaire. J Env Occup Med. 2008;25(6):572–576. [Google Scholar]
- 36.Dupret E, Bocéréan C, Teherani M, Feltrin M, Pejtersen JH. Psychosocial risk assessment: French validation of the Copenhagen psychosocial questionnaire (COPSOQ) Scand J Public Health. 2012;40(5):482–490. doi: 10.1177/1403494812453888. [DOI] [PubMed] [Google Scholar]
- 37.Berthelsen H, Hakanen J, Kristensen TS, Lönnblad A, Westerlund H. A qualitative study on the content validity of the social capital scales in the Copenhagen psychosocial questionnaire (COPSOQ II) Scand J Work Organ Psychol. 2016;1(1 (5)):1–13. [Google Scholar]
- 38.Alvarado R, Pérez-Franco J, Saavedra N, et al. Validación de un cuestionario para evaluar riesgos psicosociales en el ambiente laboral en Chile. Rev Med Chil. 2012;140:1154–1163. doi: 10.4067/S0034-98872012000900008. [DOI] [PubMed] [Google Scholar]
- 39.Pournik O, Ghalichi L, TehraniYazdi A, Tabatabaee SM, Ghaffari M, Vingard E. Measuring psychosocial exposures: Validation of the Persian of the copenhagen psychosocial questionnaire (COPSOQ). Med J Islam Repub Iran. 2015;29(1). [PMC free article] [PubMed]
- 40.COPSOQ International Network. COPSOQ International Network for scientific research and risk assessment with the Copenhagen Psychosocial Questionnaire (COPSOQ). http://www.copsoq-network.org/.
- 41.Rosário S, Fonseca J, Torres Da Costa J. SHO2014. Guimarães: Simpósio Internacional de Segurança e Higiene Ocupacional; 2014. Validação e Adaptação Linguística e Cultural da Versão Longa do Questionário Psicossocial de Copenhaga II (COPSOQ II) em Português; pp. 350–352. [Google Scholar]
- 42.Rosário S, Fonseca J, Torres Da Costa J. Occupational safety and hygiene II - selected extended and revised contributions from the international symposium occupational safety and hygiene, SHO 2014. 2014. Cultural and linguistic adaptation and validation of the long version of Copenhagen psychosocial questionnaire II (COPSOQ II) in portuguese; pp. 441–445. [Google Scholar]
- 43.Mokking L, Terwee C, Patrick D, et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual Life Res. 2010;19:539–549. doi: 10.1007/s11136-010-9606-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Terwee CB, Mokkink LB, Knol DL, Ostelo RWJG, Bouter LM, De Vet HC. Rating the methodological quality in systematic reviews of studies on measurement properties: a scoring system for the COSMIN checklist. Qual Life Res. 2012;21(4):651–657. doi: 10.1007/s11136-011-9960-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Mokkink LB, Terwee CB, Patrick DL, et al. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J Clin Epidemiol. 2010;63(7):737–745. doi: 10.1016/j.jclinepi.2010.02.006. [DOI] [PubMed] [Google Scholar]
- 46.Mokkink L, Terwee B, Patrick L, et al. Cosmin checklist manual. Amsterdam: Center, VU University Medical Biostatistics, Department of Epidemiology Research, EMGO Institute for Health and Care; 2012. [Google Scholar]
- 47.Berthelsen H, Lönnblad A, Hakanen J, et al. Cognitive interviewing used in the development and validation of Copenhagen psychosocial questionnaire in Sweden. In: Isidorsson T, Håkansson K, Oudhuis M, Schiller B, et al., editors. Conference paper presented at the 7th Nordic working life conference, Göteborg, Sweden - stream 26: methodological challenges for working life and labour market studies. Göteborg: The 7th Nordic Working Life Conference; 2014. [Google Scholar]
- 48.Berthelsen H, Hakanen J, Kristensen T, Lönnblad A, Westerlund H. A qualitative study on the content validity of the social scales in the Copenhagen in the Copenhagen psychosocial questionnaire (COPSOQ II) Scand J Work Organ Psychol. 2016;1((1) 5):1–13. [Google Scholar]
- 49.Copenhagen Psychosocial Questionnaire in Portugal. Scientific research and risk assessment with the Copenhagen Psychosocial Questionnaire (COPSOQ) in Portugal. www.copsoq.pt.
- 50.Comrey AL, Lee HB. A First Course in Factor Analysis (2nd Ed.). New York: Lawrence Erlbaum Associates; 1992. doi:10.1037/0011756.
- 51.MacCallum RC, Widaman KF, Zhang S, Hong S. Sample size in factor analysis. Psychol Methods. 1999;4(1):84–99. doi: 10.1037/1082-989X.4.1.84. [DOI] [Google Scholar]
- 52.Decreto-Lei n.o 381/2007, 14 de Novembro, 1a série – N.o 219. Estabelece a Classificação Portuguesa de Atividades Económicas (CAE), Revisão 3 (CAE – Rev. 3). 2007:pp 8440–8464. https://dre.pt/application/file/a/629058.
- 53.European Commission . Eurostat methodologies and working papers: NACE rev.2 statistical classification of economic activities in the European Community. Luxembourg: Office for Official Publications of the European Communities; 2008. [Google Scholar]
- 54.Nations U. International Standard Industrial Classfication of All Economic Activities Rev.4.; 2008. doi:10.1007/s13398-014-0173-7.2.
- 55.Fundação Francisco Manuel dos Santos. Pordata (Base de Dados Portugal Contemporânea). Empresas: Total E Por Sector de Atividade Económica. Lisboa: Fundação Francisco Manuel dos Santos; 2013. http://www.pordata.pt/.
- 56.Instituto Nacional de Estatística. Classificação Portuguesa Das Profissões 2010. Lisboa: Instituto Nacional de Estatística I.P; 2011. https://www.ine.pt.
- 57.United Nations. International Standard Classification of Occupations - ISCO 2008. Vol I. Geneva: United Nations; 2012. http://www.ilo.org/public/english/bureau/stat/isco/.
- 58.McDowell I. Measuring Health — a Guide To Rating Scales and Questionnaires. 3rd ed. Oxford: Oxford University Press; 2006. doi:10.1179/108331900786166731.
- 59.Streiner D, Norman G. Health measurement scales – a practical guide to their development and use. 2. New York: Oxford University Press; 1995. [Google Scholar]
- 60.Nunnally J, Bernstein I. Psychometric theory. 3. New York: McGraw-Hill; 1994. [Google Scholar]
- 61.Fayers P, Machin D. Quality of life: the assessment, analysis and interpretation of patient report outcomes. 2. Chichester: John Wiley & Sons Ltd; 2007. [Google Scholar]
- 62.Roe Y, Haldorsen B, Svege I, Bergland A. Development and reliability of a clinician-rated instrument to evaluate function in individuals with shoulder pain: a preliminary study. Physiother Res Int. 2013;18(4):230–238. doi: 10.1002/pri.1555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Terwee C, Mokkink L, Steultjens M, Dekker J. Performance-based methods for measuring the physical function of patients with osteoarthritis of the hip or knee: a systematic review of measurement properties. Rheumatology (Oxford) 2006;45(7):890–902. doi: 10.1093/rheumatology/kei267. [DOI] [PubMed] [Google Scholar]
- 64.Cohen J. Statistical power analysis for the Behavioral sciences. 2. Hillsdale: Lawrence Erlbaum Associates Publishers; 1988. [Google Scholar]
- 65.Thompson B. Exploratory and Confirmatory Factor Analysis: Understanding Concepts and Applications. Washington, DC; 2004. doi:10.1037/10694-000.
- 66.Kang H. The prevention and handling of the missing data. Korean J Anesth. 2013;64(5):402–406. doi: 10.4097/kjae.2013.64.5.402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Thorsen S, Bjorner J. Reliability of the Copenhagen Psychosocial Questionnaire. Scand J Public Health. 2010;38(3):25–32. [DOI] [PubMed]
- 68.Cortina JM. What is coefficient alpha? An examination of theory and applications. J Appl Psychol. 1993;78(1):98–104. doi:10.1037/0021-9010.78.1.98.
- 69.Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16(3):297–334. doi:10.1007/BF02310555.
- 70.Bollen KA. Multiple indicators: Internal consistency or no necessary relationship? Qual Quant. 1984;18(4):377–385. doi:10.1007/BF00227593.
- 71.Bollen K, Lennox R. Conventional Wisdom on Measurement: Psychol Bull. 1991;110(2):305–14. doi:10.1037/0033-2909.110.2.305.
- 72.Fayers M, Hand J. Factor analysis, causal indicators and quality of life. Qual Life Res. 1997;6(2):139–150. doi: 10.1023/A:1026490117121. [DOI] [PubMed] [Google Scholar]
- 73.Fayers M, Hand J. Causal variables, indicator variables and measurement scales:an example from quality of life. J R Stat Soc. 2002;165:233–261. doi: 10.1111/1467-985X.02020. [DOI] [Google Scholar]
- 74.Streiner D. Being inconsistent about consistency:when coefficient alpha does and doesn’t matter. J Pers Assess. 2003;80:217–222. doi: 10.1207/S15327752JPA8003_01. [DOI] [PubMed] [Google Scholar]
- 75.Bjorner J, Pejtersen J. Evaluating construct validity of the second version of the Copenhagen psychosocial questionnaire through analysis of differential item functioning and differential item effect. Scand J Public Health. 2010;38(3):90–105. doi: 10.1177/1403494809352533. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data are available by contacting the author: Susel Rosário: e-mail: skrosario@gmail.com