

Abstract
Background:
Flexural strength (FS) of denture base resins (DBRs) had been improved by reinforcing it with different glass fibers. However, a limited data are available on the effect of glass fiber reinforcement with conventional heat-cured resin after prolonged water storage.
Aims and Objectives
This study aimed to evaluate the reinforcing effect of novel S-glass and nylon fibers on the FS of acrylic DBRs. It also aimed to evaluate the effect of glass fiber reinforcement on the FS of acrylic DBRs after a prolonged storage in water.
Materials and Methods:
One hundred and sixty identical specimens were fabricated in specially designed molds according to the manufacturer's instructions. The three experimental groups were prepared consisting of conventional (unreinforced) acrylic resin, novel S-glass fiber-reinforced and nylon fiber-reinforced acrylic resin. The specimens were fabricated in a standardized fashion for each experimental group. Each group was further subdivided into two groups on the basis of storage conditions (dry and wet). FS was tested using a three-point universal testing machine at a crosshead speed of 5 mm/min. Glass fiber-reinforced group was further tested after prolonged storage in distilled water. Entered data were statistically analyzed with one-way ANOVA and least significant difference post hoc test.
Results:
In this study, statistically significant differences were noted in the FS of all the groups. S-glass fiber-reinforced group had highest FS compared to the other two groups (P < 0.001). Nylon fiber-reinforced group had lowest FS. All the groups stored in distilled water revealed a decrease in strength compared to those stored in dry atmosphere. Among wet specimens, those stored for 3 weeks had a significantly higher FS than those stored at one and 2 weeks (P < 0.01).
Conclusion:
Within the limitations of this investigation, the FS of heat-cured acrylic DBR was improved after reinforcement with glass fibers. It can be recommended to strengthen distal extension partial and complete denture bases. Nylon fibers may not be desirable for strengthening acrylic denture bases.
Keywords: Denture base material, fiber-reinforced resin, flexural strength, glass fibers
Introduction
Introduction of polymethyl methacrylate (PMMA) for use as denture base material dates back to the year 1937 when Dr. Walter Wright clinically evaluated PMMA and found that it fulfilled all the requirements of an ideal denture base material (DBM).[1] Ever since its introduction, PMMA continues to be used because of its favorable working characteristics, processing ease, accurate fit, stability in oral environment, good color stability, superior esthetics, and use with inexpensive equipment. However, despite these advantages, it has certain poor mechanical properties. Fractures may occur in use because of its unsatisfactory transverse strength, impact strength, or fatigue resistance.[2]
Most dentures fracture inside the mouth, primarily due to resin fatigue, with midline fractures being commonly encountered.[3,4] Outside the mouth, fracture occurs due to impact of falling. Various modifications have been suggested to overcome these shortcomings, which included plasticization,[5] copolymerization with rubber,[6] use of cross-linking agents such as polyethylene glycol dimethacrylate, and reinforcement with metal strengtheners.[7,8] Last two decades have seen a dramatic increase in the use of fiber-reinforced composites with different fibers such as glass, aramid, carbon, nylon, whiskers, and ultra-high-modulus polyethylene fibers being incorporated in the acrylic resin.
Several studies[9,10] have suggested the use of nylon as a DBM fabricated using the injection molding technique. Very few studies in the past have tested the effect of nylon as a reinforcement fiber on the flexural strength (FS) of acrylic resin.[10,11] Studies have been carried out using the novel glass fiber reinforcement system - Stick and Stick Net (Stick Tech Ltd., Turku, Finland) to find their effect on the FS of acrylic resin.[2] These glass fibers were found suitable and desirable for reinforcement of complete and partial dentures as they improved the FS of acrylic resin. However, the influence of prolonged water storage on the mechanical properties of acrylic resin reinforced with these novel glass fibers is still unknown.
Ramos et al.[12] evaluated the effect of a plasma-treated polyethylene fiber on the fracture strength of PMMA and observed a drastic increase in the fracture strength of the treated group as compared to the untreated group. In addition to the increased fracture strength, the treated group also demonstrated resistance to crack propagation. Stipho[13] investigated the different effects of quantitative percentages (0%, 1%, 2%, 5%, 10%, 15%) of glass fiber intensity on the transverse strength, maximum deformation, and the modulus of elasticity of acrylic resin and noted that 1% glass fiber treatment enhanced the transverse strength of the tested specimen. The interaction of glass fiber concentration on fracture strength and deformation was significant (P < 0.0001). Cucci et al.[14] compared the water sorption, solubility, and the transverse bond strength of 2 autopolymerizing acrylic resins and 1 heat-polymerizing acrylic resin. No difference was noted in the solubility of all materials. Autopolymerizing acrylic resin demonstrated significantly lower transverse bond strength to denture base acrylic resin and failed adhesively. Vallittu[15] conducted a study to describe and test a novel system to use polymer-preimpregnated reinforcing fibers with commonly used multiphase acrylic resins. Continuous unidirectional and woven preimpregnated glass fiber reinforcements (Stick and Stick Net) were used to reinforce heat-polymerizing and autopolymerizing denture base polymers. A temporary fixed partial denture polymer was also reinforced with Stick reinforcement material. As a result Stick Net reinforcement increased the strain at fracture, whereas Stick reinforcement decreased the strain values. Standard error of the mean examination revealed well-impregnated glass fibers with polymer matrix. Quantity of glass fibers varied from 6% to 28 vol%, the lowest being with Stick Net reinforcement and the highest with Stick reinforcement. John et al.[10] conducted an in vitro study to compare the FS of a heat-polymerized acrylic resin after reinforcement with glass, aramid, and nylon fibers. They observed a better FS in the reinforced group than the conventional one. Specimens reinforced with glass fibers showed the highest FS, followed by aramid and nylon. Narva et al.[16] compared static three-point FS of denture base polymer that had been reinforced with different fiber reinforcements such as nonimpregnated polyethylene fibers, light-polymerized monomer impregnated glass fibers, porous polymer preimpregnated glass fibers, and light-polymerized monomer-polymer impregnated glass fibers. The results showed that the brand and the location of the fiber reinforcements significantly influenced the FS. However, the location of the fiber reinforcements did not influence the flexural modulus. Barbosa et al.[17] compared the FS between a conventional heat-polymerized, a microwave-polymerized, and an autopolymerizing acrylic resin. The results showed highest FS in microwave-polymerized groups and lowest in heat-polymerized group. Diaz-Arnold et al.[18] evaluated static and dynamic flexure properties of a variety of acrylic resins utilized in the fabrication of prostheses and found that lucitone possessed higher static and postcycling FS compared to other heat-cured and light-cured acrylic resins. Mutneja et al.[19] conducted an in vitro study to evaluate the FS of heat-cured acrylic resin after incorporating different percentages of silver-zinc zeolite (0%, 0.5%, 1%, 2%). As a result the study showed a statistically significant decrease in FS with the addition of 0.5%, 1% and 2% of silver-zinc zeolite to heat-cured acrylic resin. Fonseca et al.[20] evaluated the effect of fiber addition in flexural properties of 30 weight % silica-filled Bis-GMA resin or unfilled Bis-GMA. The results showed that the FS of fiber addition in Bis-GMA resin increases flexural properties, and the interaction between resin and fibers seems better in the absence of inorganic fillers increasing flexural properties. Ajaj-Alkordy Alsaadi[21] conducted a study to compare the elastic modulus and the FS between two heat-cured acrylic resins and found that the high-impact acrylic resin demonstrated lower elastic modulus and higher FS compared to the traditional acrylic resin.
The present in vitro study aimed to evaluate and compare the effect of novel glass fiber and nylon fiber reinforcement system on the FS of heat-polymerizing acrylic resin under dry and wet conditions. It also aimed to evaluate the effect of this novel glass fiber reinforcement system on the FS of heat-polymerizing resin after a prolonged water storage interval.
Materials and Methods
A total of 160 specimens were fabricated for the study. These were further divided into three groups (Group A, B, and C), out of which Group A and C were comprised 40 specimens each. Group A (control) comprised unreinforced (conventional) acrylic resin specimens and Group C comprised acrylic resin specimens reinforced with nylon fibers. Specimens in each group were further subdivided into two groups (20 specimens each), based on dry (D at room temperature) and wet storage conditions (W in distilled water at 37°C ± 1°C for 7 days), and Group B comprised acrylic resin specimens reinforced with S-glass fibers which consisted of 20 specimens for dry and 20 for wet condition each (for 7 days, 14 days, and 21 days). The groups were then designated as Group A-D and A-W7, Group B-D and B-W7 + B-W14 + B-W21, and Group C-D and C-W7.
Two rectangular stainless steel dies of standard dimensions (65 mm × 10 mm × 3 mm) were fabricated according to the revised ADA specification number 12 for denture base polymers.[22] These dies were invested in a metal flask with dental stone to prepare a mold using the conventional flasking technique. Heat-polymerizing acrylic resin (Trevalon, Dentsply International) was mixed according to the manufacturer's instructions and packed during the dough stage into the plaster mold space and pressed with a force of 300 N in a hydraulic press (Press, Dentalfarm Torino-Italy). To minimize air inclusions, a roller was used over the material while in the doughy stage after placement in the mold. The upper and lower halves of the flask were closed and the recommended polymerization cycles were followed. The flask was kept in the water bath at 23°C ± 2°C water, and then, the temperature was increased to 100°C ± 0.5°C for 45 min. The mold was cooled in air to 23°C ± 1°C, after which the test specimens were removed from the mold.[15] Two test specimens were polymerized in the mold simultaneously. A total of 40 specimens were selected for this control group.
To prepare S-fiber-reinforced acrylic resin specimens, S reinforcements (Stick (S) Stick Tech Ltd., Turku, Finland] were cut into the length of 60 mm and width of 8 mm. These fibers were wetted with a mixture of polymer powder and monomer liquid after mixing the heat-polymerizing acrylic resin. The wetted reinforcements were packed into polyethylene bags for 10 min to form dough-like reinforcements. After attaining a dough-like consistency, the reinforcements were placed into the mold and pressed with a force of 300 N, as followed for the control specimens.[15] The polymerization cycle followed was the same as that for the control specimens. A total of 80 specimens were selected for this S-fiber-reinforced group.
The nylon fibers (Gujlon-Kim, Gujarat, India) were cut into 10 mm long pieces, and these cut fibers were soaked in monomer for 10 min for better bonding with the heat-polymerizing acrylic resin.[23] After this, these fibers were removed from the monomer and the excess liquid was allowed to dry. The acrylic resin and nylon fibers (2% by weight[23]) were mixed thoroughly to disperse the fibers. The nylon fibers were randomly oriented in the specimen. On reaching dough stage, the mixture was kneaded and packed into the prepared mold. The specimens were polymerized and recovered in the same manner as that of control and S-fiber-reinforced specimens. After deflasking, if the specimens revealed exposed fibers at the peripheral border, trimming was carried out with diamond burs to avoid delamination of the reinforcement. A total of 40 specimens were selected for this nylon fiber-reinforced group.
After deflasking, all specimens were retrieved and were finished with a tungsten carbide bur at 45,000 rpm and polished using conventional laboratory polishing method: coarse pumice, water and lathe bristle brush for 90 s at a rate of 2800 rpm (Unident India Pvt. Ltd.,), and soft leather polishing wheel for 90 s at a rate of 6500 rpm (Unident India Pvt. Ltd.,). The finished and polished S-fiber-reinforced specimens (20 specimens each) were stored for wet conditions in distilled water in water bath (VWR, International Radnor, Pennsylvania) at 37°C ± 1°C for 7, 14, and 21 days of interval. Furthermore, 20 specimens each of control and nylon fiber-reinforced specimens were stored in a similar manner. Width and thickness of each specimen was measured with a digital vernier caliper (Caloratory Product, Ambala Cantt., Haryana, India) and the excess was trimmed. A three-point bending test was conducted for FS using an Instron universal testing machine (Lloyd LR 100K) at a crosshead speed of 5 mm/min. The specimens were placed on jigs that were 50.0 mm apart and then a load was applied by a centrally located road until fracture of specimen occurred. The maximum load at this fracture of specimen was recorded and converted into FS using the following formula: FS σ =3 × F × L/2 × b × d2 (where, F is the maximum load applied, L is span between two supports, b is width of the specimen, and d is the thickness of the specimen).[2]
Results
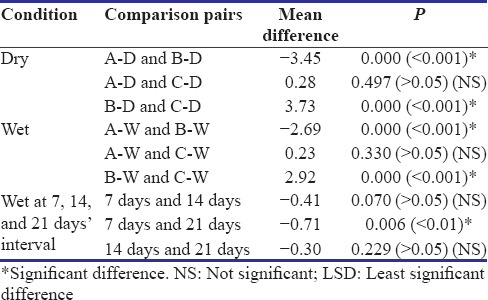
The mean FS of the control, s-glass fiber, and nylon fiber-reinforced groups under dry and wet conditions is summarized in Table 1. The mean FS of unreinforced group under dry conditions was 8.77 ± 1.33 kgf/mm2, which increased to 12.22 ± 1.16 kgf/mm2 on reinforcement within S-glass fibers. The group reinforced with nylon fibers showed a decrease in FS to 8.49 ± 1.30 kgf/mm2. The comparison of mean FS values among three groups of dry specimens using one-way ANOVA showed a significant difference (P < 0.001) [Table 2]. Least significant difference (LSD) post hoc test showed a significant higher FS values in Group B than other groups when tested under dry conditions. No significant difference was observed between Group A and C. The specimens of all the three groups, when stored in water for 7 days, showed a decrease in their mean FS. The wet specimens of control, glass fiber-reinforced, and nylon fiber-reinforced group had a mean FS value of 8.43 ± 1.01 kgf/mm2, 11.12 ± 0.56 kgf/mm2, and 8.20 ± 0.54 kgf/mm2, respectively [Graph 1]. S-glass fiber reinforcements showed an increased FS of denture base resin (DBR) in dry and wet atmosphere. However, nylon fiber reinforcements revealed their weakness in strengthening DBR under both the conditions. One-way ANOVA showed significant difference between the groups of wet specimens (P < 0.001). LSD post hoc test revealed a significantly higher FS values in wet specimens of Group B compared to Group A and C. No significant difference was noted between Group A and C. The mean FS values of Group B under wet conditions at 7, 14, and 21 days’ interval were 11.12 ± 0.56 kgf/mm2, 11.53 ± 0.64 kgf/mm2, and 11.83 ± 0.80 kgf/mm2, respectively [Graph 2]. Repeated measures one-way ANOVA showed significant difference between FS of wet specimens of Group B at different time intervals. LSD post hoc test showed a significantly higher FS at 21 days’ interval than 7 days’ interval. No significant difference was observed between 7 and 14 days’ interval and 14 and 21 days’ interval.
Table 1.
Comparison of flexural strength of dry, wet, and wet specimens at different time interval in different groups using one-way ANOVA
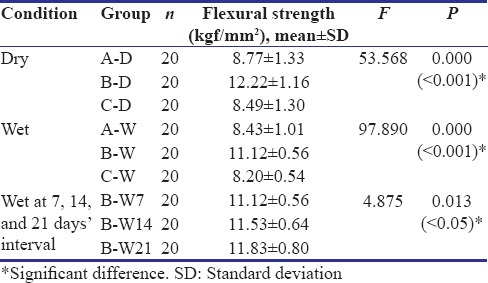
Table 2.
Pairwise comparison of groups for flexural strength of dry, wet, and wet specimens of Group B at different time interval using least significant difference post hoc test
Graph 1.
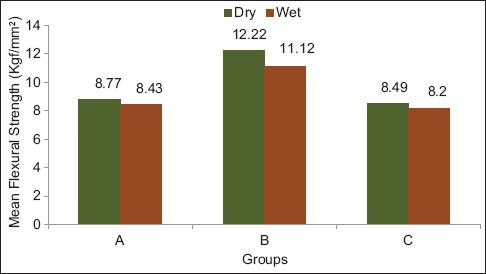
Mean values of flexural strength of dry and wet specimens in different groups
Graph 2.
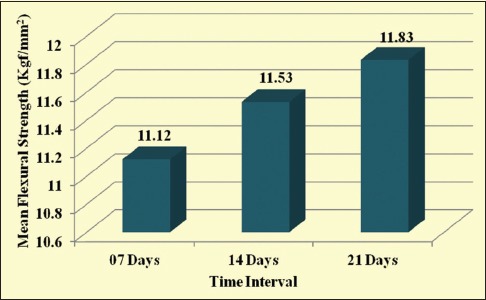
Mean values of flexural strength of wet specimens of Group B at different time interval
Discussion
Despite its popularity, PMMA material is far from ideal in fulfilling the mechanical requirements.[24,25] The fracture of acrylic resins denture, especially midline fracture, is a common clinical finding in prosthodontic practice,[8,26,27,28] which mainly results due to flexural fatigue. Fracture of acrylic resin denture occurs both outside and inside the mouth. Outside the mouth, failure occurs through impact if the denture is dropped by the patient. Inside the mouth, occlusal forces may also cause fracture.[24] Among the different causes of denture fracture, poor fit, lack of balanced occlusion, material fatigue, and dropping of the denture were identified as the most possible causes.[29]
To overcome this problem and to improve the mechanical properties of dental polymers, various types of fibers, carbon, aramid, glass, and metal wire reinforcement have been tested. The traditional method to increase denture strength involves the use of high strength resins or applying strengtheners to the DBRs. There is evidence that the transverse strength of resins can be slightly enhanced by the use of metal strengtheners. However, the influence of metal strengtheners on the fatigue resistance of dental appliances is minor. Earlier attempts to use metal wires and metal plate strengtheners are typified by the work of Ruffino,[7] Vallittu and Lassila,[8] and Jennings and Wuebbenhorst.[30] To solve the problem related with these metal strengtheners, various types of fiber reinforcements have been investigated for use with dental polymers.[31] The development of fiber composite materials in the industry has inspired a new approach to improve the performance of dental polymers. DBR made from PMMA resin has been reinforced with various types of fibers such as carbon/graphite, aramid, ultra-high-modulus polyethylene fibers, and glass fibers.[8,23,27,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47] Carbon and aramid fibers were useful in strengthening PMMA but produced important clinical problems, namely, difficult polishing and poor esthetics.[32,33] Inclusion of metal wires and plate reinforcement improves denture performance against fracture due to extensive biting forces or impact forces problems[28,32,48] but results in poor esthetics that restrict their use only in locations where esthetics are least important. Woven polyethylene fibers normally develop anisotropic properties to the composite. They are more esthetic but the process of etching, preparing, and positioning layers of the woven fibers may not be practical in the dental office. On the other hand, glass fibers have shown better potential for provisional restorations, despite difficulties to achieve adequate impregnation of the fibers with PMMA.[27,28]
Various factors affecting the strength of fiber composites are an adequate impregnation of reinforcing fibers with resin matrix, quantity and orientation of fibers, and adhesion of fibers. Problem constantly faced with the fiber reinforcement of acrylic resin is to achieve adequate impregnation of reinforcing fibers with resin, which is a prerequisite for proper bonding of fibers to the polymer matrix and thus for the strength of composite. This problem is solved to a great extent by Vallittu[48] with the use of the polymer preimpregnation of the novel fiber reinforcements S and SN tested in his study seemed to have resolved the problem of impregnating reinforcing fibers with resin of the polymer matrix. The porous preimpregnated polymer was wetted and dissolved with monomers of the mixture of acrylic resin powder and liquid. The use of the mixture of polymer powder and monomer liquid instead of plain monomer liquid was important to avoid excess of monomers inside the fiber reinforcement. When acrylic resin polymer powder and monomer liquid were mixed, monomers dissolved and swelled the surface of the powder beads. Subsequently, after mixing the powder and liquid, small quantities of “free” monomers were left to penetrate into the porous polymer of S and SN reinforcements and dissolve the preimpregnated polymer. This plasticized the reinforcement and made it possible to form the reinforcement and place it into the desired region of the restoration. After polymerization of the resin, the reinforcement formed a dense fiber composite structure.
In the present study, the FS of unreinforced and reinforced acrylic resin specimens was tested in accordance with ISO/DIS 1567.[49] Quantity of glass fibers used in this study is in consensus with the studies conducted by Aydin et al.,[50] who experimented the same novel system of S-glass fibers. The glass fibers were oriented perpendicular to the direction of applied force providing greatest potential for improvement of flexural fatigue and bending properties of the DBRs.[51] The quantity of nylon fibers added in each specimen was 2% by weight of the polymer: monomer ratio.[23]
When S-glass fibers were used, a clear and considerable improvement in FS (12.22 ± 1.16 kgf/mm2) was found over the strength of unreinforced acrylic resin specimens (8.77 ± 1.33 kgf/mm2). The difference noted between these groups was statistically significant (P < 0.001). This finding is in agreement with the results of the previously documented studies.[2,15,43,44,50] The results of the present study suggest that S-glass fibers were well impregnated with the resin of polymer matrix. When S-glass fiber was used in heat-polymerized acrylic resin specimens, a clear improvement in FS approximately 50% was noticed over the strength of the unreinforced specimens. These results revealed that the reinforcement of DBRs with glass fibers may be a useful approach of strengthening denture bases beyond their normal limits. S-glass fibers offered the highest strength to the fiber composite and are found suitable in applications where the direction of highest stress is required. These fibers efficiently reinforced the polymer matrix in only one direction, that is, in the direction of fibers in contrast to the bidirectional woven glass fibers which reinforce the polymer matrix in two directions and are therefore useful when it is difficult to predict the direction of highest stress. Hence, the reinforcing effects of unidirectional S-glass fibers are anisotropic offering improved mechanical properties to the composite.
Nylon is a type of thermoplastic polymer, more precisely polyamides having wide commercial application. This polymer possesses an outstanding features of toughness, low density, abrasion resistance, high melting point, high strength adjoined with ductility, and resistance to chemical attack.[9] However, in spite of their excellent physical properties, they were found to be unsatisfactory for denture base use due, principally, to a combination of high molding shrinkage which led to warpage, high water absorption, and yellowing.[3] Commercial unavailability of preimpregnated nylon fibers led to utilize an alternative approach to ensure proper bonding of these fibers with denture polymer matrix. These fibers were wetted with MMA liquid for 10 min. Based on the concept of solubility parameters for polymers,[52,53] any two polymers are miscible or compatible with each other if the difference in their solubility is ≤3.5 × 103 J1/2 M−3/2. When solubility parameters of PMMA and nylon was calculated, it was observed that the difference in solubility of both the materials was <3.5 × 103 J1/2 M−3/2. This difference emitted the need of coupling agent for the nylon fibers. Nylon fibers were randomly oriented in acrylic resin as their placement parallel to the long axis of the specimen caused their spreading out in lateral direction. Furthermore, these fibers were lost when the flasks were closed and bench pressed. When compared with the unreinforced acrylic resin specimens (8.77 ± 1.33 kgf/mm2), nylon reinforced specimens (8.49 ± 1.30 kgf/mm2) showed a decrease in FS which was statistically insignificant (P > 0.05). This result is in agreement with Ladha and Shah,[2] who observed a decreased FS with nylon-reinforced specimens (8.473 ± 0.508 kgf/mm2) over the control group specimens (8.815 ± 0.660 kgf/mm2). Nylon fibers were found to be unsuitable and undesirable as the reinforcement filler for the use with DBRs.
To simulate the oral environment, all the specimens were stored into the water bath at 37°C ± 1°C for 7 days. S-fiber-reinforced specimens were further stored for 14 and 21 days’ interval. In the present study, the storage of specimens in water decreased the FS in all the groups, i.e. reinforced and unreinforced specimens. For unreinforced and S-fiber and nylon-reinforced specimens, a decrease in FS observed was 8.43 ± 1.01, 11.12 ± 0.56, and 8.20 ± 0.54 kgf/mm2, respectively. A statistically significant difference (P < 0.001) was noted between unreinforced and reinforced groups. For this decreased FS, detrimental effects of water storage on the mechanical properties of acrylic resin have been suggested. This result is in agreement with the previously reported studies.[2,53] Improper impregnation and improper wetting are associated with an increased water sorption and inhibition of the radical polymerization of acrylic resin due to oxygen entrapment in the voids of poorly impregnated fiber composite.[53,54] This might be associated with the reduced strength of the fiber composite. Results of recent study by Vallittu[44] suggest that polymerization shrinkage of DBR between the reinforced fibers can also reduce the strength of fiber-reinforced composite. Discoloration of the reinforcement may also occur due to penetration of oral microbes in these voids.[55] High water absorption tendency of nylon fibers could be the contributing factor in decreasing the FS of specimens stored in water.[3]
The approach of testing FS of S-fiber-reinforced specimens after water storage interval of 7, 14, and 21 days in this investigation is a clinically relevant means to study the FS of the DBR since it simulates closely the loading arrangement in the clinical situation. S-fiber-reinforced specimens showed a significant increase in FS at 21 days’ storage interval (11.83 ± 0.80 kgf/mm2), compared to 7 days’ interval (11.12 ± 0.56 kgf/mm2). The difference between these two groups was statistically significant (P < 0.01). The specimens stored at 7 days and 14 days showed a nonsignificant difference between the mean values of FS. Similarly, the specimens stored at 14 and 21 days demonstrated a nonsignificant difference. Vallittu[56] reported 14% decrease in the transverse strength of the E-glass fiber-reinforced test specimens after 48 weeks of storage in water. Most of this reduction was found to occur during the first 4 weeks of storage in water. Lastumäki et al.[56] reported a 60% decrease in FS of the glass fiber-reinforced composites after 3 months of water storage. The reasons of decreased flexural property could be that the water has caused leaching of ions or oxides from the glass fiber surface. It has been also reported that the elements such as boron (B2O3), which are added to E-glass fibers to decrease high calcium oxide (CaO) content, may increase the hydrolytic degradation and negatively influence the polymer-fiber system.[55] In the present study, the increase in FS of S fiber-reinforced specimens was observed after 3 weeks. The future study evaluating the FS of S fiber composite after a water storage interval of more than 3 weeks till 48 weeks can be investigated.
Material fatigue is the predominant failure mechanism of dental prosthesis.[27,29,57,58,59,60] The fatigue failure is caused by repeated occlusal loads that cause tensile stresses in some regions of the restoration; after a period of wearing time, the prosthesis fractures. Fatigue fractures can occur even though the static strength of the material is high enough to carry the occlusal stresses.[61] There is evidence from dynamic in vitro tests that glass fiber reinforcement in increased fatigue resistance of dental prosthesis up to 100 times compared with fatigue resistance of an unreinforced restoration.[27] This finding is not surprising because fiber composites are reputed to have high fatigue strength, and therefore, fiber composites have been used for years in structures such as aircraft, which requires high fatigue strength.[62] By combining the reinforcing effect of S-glass fibers, the mechanical properties of dental prosthesis can be tailored to specific needs. Reinforcement of prosthesis can be planned to carry the stresses by the masticatory system using accurately placed reinforcement of S-type fibers.
Limitations
The present study was conducted in an in vitro environment, and other factors such as the presence of saliva, pH of saliva, and cytotoxicity from oral microbes which would have an effect on the fiber composite were not considered. One more limitation of this study was that no aging or thermal cycling of resin materials was evaluated. Thermocycling process could more accurately interpret true oral conditions and affect the mechanical properties of resin materials.
Since only one brand of glass fibers and heat-polymerizing acrylic resin was used, the restricted generalization of results could have been avoided by testing the glass fibers and acrylic resin of other brands.
Future scope
Since it has been reported that the glass reinforcement significantly affects the water sorption and solubility of DBR, the future studies need to be conducted to investigate the mechanical properties such as FS after a long-term water storage interval. To simulate an oral environment, future in vitro studies can be conducted using the artificial saliva for the storage of specimens instead of distilled water. In previous studies,[63] it was found that the glass fiber-reinforced heat-polymerizing acrylic resin caused moderate cytotoxicity by decreasing the proliferation of gingival fibroblasts by approximately 20%. Hence, the cytotoxicity of recently introduced reinforcing fibers in prosthetic field is to be considered in future investigations. To investigate the effects of periodontal ligament, proprioceptors, complicated occlusal contact patterns and occlusal loading, intraoral thermal changes, and pH variations, future studies based on randomized well-controlled clinical trials can be carried.
Conclusions
Within the limitations of this study, the following conclusions were drawn:
S-glass fiber-reinforced specimens showed an increase in the FS compared to unreinforced and nylon fiber-reinforced samples, when tested under dry condition
Nylon fiber-reinforced specimens showed a decrease in the FS compared to unreinforced specimens when tested under dry condition
Reinforced and unreinforced specimens showed a decrease in the FS when tested after 7 days of water storage interval
S-glass fiber-reinforced specimens showed an increase in the FS after 21 days of water storage interval when compared with 7 and 14 days of interval
Use of nylon fiber as a reinforcement filler for DBRs is not desirable.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Peyton FA. History of resins in dentistry. Dent Clin North Am. 1975;19:211–22. [PubMed] [Google Scholar]
- 2.Ladha K, Shah D. An in-vitro evaluation of the flexural strength of heat-polymerized poly (methyl methacrylate) denture resin reinforced with fibers. J Indian Prosthodont Soc. 2011;11:215–20. doi: 10.1007/s13191-011-0086-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Smith DC. Recent developments and prospects in dental polymers. J Prosthet Dent. 1962;12:1066–8. [Google Scholar]
- 4.Stafford GD, Smith DC. Flexural fatigue tests of some denture base polymers. Br Dent J. 1970;128:442–5. doi: 10.1038/sj.bdj.4802483. [DOI] [PubMed] [Google Scholar]
- 5.Jagger DC, Harrison A, Jandt KD. Review. The reinforcement of dentures. J Oral Rehabil. 1999;26:185–94. doi: 10.1046/j.1365-2842.1999.00375.x. [DOI] [PubMed] [Google Scholar]
- 6.Stafford GD, Bates JF, Huggett R, Handley RW. A review of the properties of some denture base polymers. J Dent. 1980;8:292–306. doi: 10.1016/0300-5712(80)90043-3. [DOI] [PubMed] [Google Scholar]
- 7.Ruffino AR. Effect of steel strengtheners on fracture resistance of the acrylic resin complete denture base. J Prosthet Dent. 1985;54:75–8. doi: 10.1016/s0022-3913(85)80074-3. [DOI] [PubMed] [Google Scholar]
- 8.Vallittu PK, Lassila VP. Reinforcement of acrylic resin denture base material with metal or fibre strengtheners. J Oral Rehabil. 1992;19:225–30. doi: 10.1111/j.1365-2842.1992.tb01096.x. [DOI] [PubMed] [Google Scholar]
- 9.Matthews E, Smith DC. Nylon as a denture base material. Br Dent J. 1955;98:231–7. [Google Scholar]
- 10.John J, Gangadhar SA, Shah I. Flexural strength of heat-polymerized polymethyl methacrylate denture resin reinforced with glass, aramid, or nylon fibers. J Prosthet Dent. 2001;86:424–7. doi: 10.1067/mpr.2001.118564. [DOI] [PubMed] [Google Scholar]
- 11.Kelly E. Fatigue failure in denture base polymers. J Prosthet Dent. 1969;21:257–66. doi: 10.1016/0022-3913(69)90289-3. [DOI] [PubMed] [Google Scholar]
- 12.Ramos V, Jr, Runyan DA, Christensen LC. The effect of plasma-treated polyethylene fiber on the fracture strength of polymethyl methacrylate. J Prosthet Dent. 1996;76:94–6. doi: 10.1016/s0022-3913(96)90348-0. [DOI] [PubMed] [Google Scholar]
- 13.Stipho HD. Effect of glass fiber reinforcement on some mechanical properties of auto-polymerizing polymethyl methacrylate. J Prosthet Dent. 1998;79:580–4. doi: 10.1016/s0022-3913(98)70180-5. [DOI] [PubMed] [Google Scholar]
- 14.Cucci AL, Vergani CE, Giampaolo ET, Afonso MC. Water sorption, solubility, and bond strength of two autopolymerizing acrylic resins and one heat-polymerizing acrylic resin. J Prosthet Dent. 1998;80:434–8. doi: 10.1016/s0022-3913(98)70008-3. [DOI] [PubMed] [Google Scholar]
- 15.Vallittu PK. Flexural properties of acrylic resin polymers reinforced with unidirectional and woven glass fibers. J Prosthet Dent. 1999;81:318–26. doi: 10.1016/s0022-3913(99)70276-3. [DOI] [PubMed] [Google Scholar]
- 16.Narva KK, Lassila LV, Vallittu PK. The static strength and modulus of fiber reinforced denture base polymer. Dent Mater. 2005;21:421–8. doi: 10.1016/j.dental.2004.07.007. [DOI] [PubMed] [Google Scholar]
- 17.Barbosa DB, de Souza RF, Pero AC, Marra J, Compagnoni MA. Flexural strength of acrylic resins polymerized by different cycles. J Appl Oral Sci. 2007;15:424–8. doi: 10.1590/S1678-77572007000500010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Diaz-Arnold AM, Vargas MA, Shaull KL, Laffoon JE, Qian F. Flexural and fatigue strengths of denture base resin. J Prosthet Dent. 2008;100:47–51. doi: 10.1016/S0022-3913(08)60136-5. [DOI] [PubMed] [Google Scholar]
- 19.Mutneja P, Raghavendraswamy KN, Gujjari AN. Flexural strength of heat cure acrylic resin after incorporating different percentages of silver zinc zeolite- An In-Vitro Study. Int J Clin Case Investig. 2012;4:25–31. [Google Scholar]
- 20.Fonseca RB, Marques AS, Bernades Kde O, Carlo HL, Naves LZ. Effect of glass fiber incorporation on flexural properties of experimental composites. Biomed Res Int. 2014;2014:542678. doi: 10.1155/2014/542678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ajaj-Alkordy NM, Alsaadi MH. Elastic modulus and flexural strength comparisons of high-impact and traditional denture base acrylic resins. Saudi Dent J. 2014;26:15–8. doi: 10.1016/j.sdentj.2013.12.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Vallittu PK, Lassila VP, Lappalainen R. Acrylic resin-fiber composite – Part I: The effect of fiber concentration on fracture resistance. J Prosthet Dent. 1994;71:607–12. doi: 10.1016/0022-3913(94)90446-4. [DOI] [PubMed] [Google Scholar]
- 23.Polyzois GL, Andreopoulos AG, Lagouvardos PE. Acrylic resin denture repair with adhesive resin and metal wires: Effects on strength parameters. J Prosthet Dent. 1996;75:381–7. doi: 10.1016/s0022-3913(96)90029-3. [DOI] [PubMed] [Google Scholar]
- 24.Darbar UR, Huggett R, Harrison A. Denture fracture – A survey. Br Dent J. 1994;176:342–5. doi: 10.1038/sj.bdj.4808449. [DOI] [PubMed] [Google Scholar]
- 25.Larson WR, Dixon DL, Aquilino SA, Clancy JM. The effect of carbon graphite fiber reinforcement on the strength of provisional crown and fixed partial denture resins. J Prosthet Dent. 1991;66:816–20. doi: 10.1016/0022-3913(91)90425-v. [DOI] [PubMed] [Google Scholar]
- 26.Vallittu PK. Comparison of the in vitro fatigue resistance of an acrylic resin removable partial denture reinforced with continuous glass fibers or metal wires. J Prosthodont. 1996;5:115–21. doi: 10.1111/j.1532-849x.1996.tb00285.x. [DOI] [PubMed] [Google Scholar]
- 27.Solnit GS. The effect of methyl methacrylate reinforcement with silane-treated and untreated glass fibers. J Prosthet Dent. 1991;66:310–4. doi: 10.1016/0022-3913(91)90255-u. [DOI] [PubMed] [Google Scholar]
- 28.Beyli MS, von Fraunhofer JA. An analysis of causes of fracture of acrylic resin dentures. J Prosthet Dent. 1981;46:238–41. doi: 10.1016/0022-3913(81)90206-7. [DOI] [PubMed] [Google Scholar]
- 29.Jennings RE, Wuebbenhorst AM. The effect of metal reinforcements on the transverse strength of acrylic resin. J Dent Child. 1960;27:162–8. [Google Scholar]
- 30.Vallittu PK. A review of methods used to reinforce polymethyl methacrylate resin. J Prosthodont. 1995;4:183–7. doi: 10.1111/j.1532-849x.1995.tb00338.x. [DOI] [PubMed] [Google Scholar]
- 31.Schreiber CK. Polymethylmethacrylate reinforced with carbon fibres. Br Dent J. 1971;130:29–30. doi: 10.1038/sj.bdj.4802623. [DOI] [PubMed] [Google Scholar]
- 32.Ekstrand K, Ruyter IE, Wellendorf H. Carbon/graphite fiber reinforced poly (methyl methacrylate): Properties under dry and wet conditions. J Biomed Mater Res. 1987;21:1065–80. doi: 10.1002/jbm.820210902. [DOI] [PubMed] [Google Scholar]
- 33.Ladizesky NH, Chow TW, Cheng YY. Denture base reinforcement using woven polyethylene fiber. Int J Prosthodont. 1994;7:307–14. [PubMed] [Google Scholar]
- 34.Braden M, Davy KW, Parker S, Ladizesky NH, Ward IM. Denture base poly (methyl methacrylate) reinforced with ultra-thin modulus polyethylene fibers. Br Dent J. 1988;164:109–13. doi: 10.1038/sj.bdj.4806373. [DOI] [PubMed] [Google Scholar]
- 35.Ladizesky NH, Chow TW, Ward IM. The effect of highly drawn polyethylene fibres on the mechanical properties of denture base resins. Clin Mater. 1990;6:209–25. doi: 10.1016/0267-6605(90)90059-5. [DOI] [PubMed] [Google Scholar]
- 36.Ladizesky NH, Ho CF, Chow TW. Reinforcement of complete denture bases with continuous high performance polyethylene fibers. J Prosthet Dent. 1992;68:934–9. doi: 10.1016/0022-3913(92)90554-n. [DOI] [PubMed] [Google Scholar]
- 37.Ladizesky NH, Cheng YY, Chow TW, Ward IM. Acrylic resin reinforced with chopped high performance polyethylene fiber – Properties and denture construction. Dent Mater. 1993;9:128–35. doi: 10.1016/0109-5641(93)90089-9. [DOI] [PubMed] [Google Scholar]
- 38.Ladizesky NH, Pang MK, Chow TW, Ward IM. Acrylic resins reinforced with woven highly drawn linear polyethylene fibres 3.Mechanical properties and further aspects of denture construction. Aust Dent J. 1993;38:28–38. doi: 10.1111/j.1834-7819.1993.tb05448.x. [DOI] [PubMed] [Google Scholar]
- 39.Gutteridge DL. Reinforcement of poly (methyl methacrylate) with ultra-high-modulus polyethylene fibre. J Dent. 1992;20:50–4. doi: 10.1016/0300-5712(92)90012-2. [DOI] [PubMed] [Google Scholar]
- 40.Gutteridge DL. The effect of variations in fibre length on the impact strength of poly (methyl methacrylate) resin reinforced with ultra-high-modulus polyethylene fibre. Clin Mater. 1993;12:137–40. doi: 10.1016/0267-6605(93)90064-e. [DOI] [PubMed] [Google Scholar]
- 41.Williamson DL, Boyer DB, Aquilino SA, Leary JM. Effect of polyethylene fiber reinforcement on the strength of denture base resins polymerized by microwave energy. J Prosthet Dent. 1994;72:635–8. doi: 10.1016/0022-3913(94)90296-8. [DOI] [PubMed] [Google Scholar]
- 42.Vallittu PK, Lassila VP, Lappalainen R. Transverse strength and fatigue of denture acrylic-glass fiber composite. Dent Mater. 1994;10:116–21. doi: 10.1016/0109-5641(94)90051-5. [DOI] [PubMed] [Google Scholar]
- 43.Vallittu PK. Acrylic resin-fiber composite – Part II: The effect of polymerization shrinkage of polymethyl methacrylate applied to fiber roving on transverse strength. J Prosthet Dent. 1994;71:613–7. doi: 10.1016/0022-3913(94)90447-2. [DOI] [PubMed] [Google Scholar]
- 44.Vallittu PK. The effect of void space and polymerization time on transverse strength of acrylic-glass fibre composite. J Oral Rehabil. 1995;22:257–61. doi: 10.1111/j.1365-2842.1995.tb00083.x. [DOI] [PubMed] [Google Scholar]
- 45.Vallittu PK. Impregnation of glass fibers with polymethylmethacrylate by using a powder coating method. Appl Compost Mater. 1995;2:51. [Google Scholar]
- 46.Vallittu PK, Vojtkova H, Lassila VP. Impact strength of denture polymethyl methacrylate reinforced with continuous glass fibers or metal wire. Acta Odontol Scand. 1995;53:392–6. doi: 10.3109/00016359509006007. [DOI] [PubMed] [Google Scholar]
- 47.Carroll CE, von Fraunhofer JA. Wire reinforcement of acrylic resin prostheses. J Prosthet Dent. 1984;52:639–41. doi: 10.1016/0022-3913(84)90132-x. [DOI] [PubMed] [Google Scholar]
- 48.Vallittu PK. Inst Dent Bio Proj. Finland: University of Turku; 1999. The first symposium on fiber reinforced plastics in dentistry; pp. 4–14. [Google Scholar]
- 49.Geneva: International Organization for Standardization; 1998. ISO/DIS 1567. Dentistry: Denture Base Polymers; pp. 1–27. [Google Scholar]
- 50.Aydin C, Yilmaz H, Caglar A. Effect of glass fiber reinforcement on the flexural strength of different denture base resins. Quintessence Int. 2002;33:457–63. [PubMed] [Google Scholar]
- 51.DeBoer J, Vermilyea SG, Brady RE. The effect of carbon fiber orientation on the fatigue resistance and bending properties of two denture resins. J Prosthet Dent. 1984;51:119–21. doi: 10.1016/s0022-3913(84)80117-1. [DOI] [PubMed] [Google Scholar]
- 52.Vallittu PK. Comparison of two different silane compounds used for improving adhesion between fibres and acrylic denture base material. J Oral Rehabil. 1993;20:533–9. doi: 10.1111/j.1365-2842.1993.tb01640.x. [DOI] [PubMed] [Google Scholar]
- 53.Vallittu PK, Ruyter IE, Ekstrand K. Effect of water storage on the flexural properties of E-glass and silica fiber acrylic resin composite. Int J Prosthodont. 1998;11:340–50. [PubMed] [Google Scholar]
- 54.Vallittu PK. Oxygen inhibition of auto-polymerization of polymethyl methacrylate-glass fiber composite. J Mater Sci Mater Med. 1997;8:489–92. doi: 10.1023/a:1018578210453. [DOI] [PubMed] [Google Scholar]
- 55.Vallittu PK. Prosthodontic treatment with a glass fiber-reinforced resin-bonded fixed partial denture: A clinical report. J Prosthet Dent. 1999;82:132–5. doi: 10.1016/s0022-3913(99)70145-9. [DOI] [PubMed] [Google Scholar]
- 56.Lastumäki TM, Lassila LV, Vallittu PK. Flexural properties of the bulk fiber-reinforced composite DC-tell used in fixed partial dentures. Int J Prosthodont. 2001;14:22–6. [PubMed] [Google Scholar]
- 57.Vallittu PK, Lassila VP, Lappalainen Niom R. The effect of notch shape and self-cured acrylic resin repair on the fatigue resistance of an acrylic resin denture base. J Oral Rehabil. 1996;23:108–13. doi: 10.1111/j.1365-2842.1996.tb01218.x. [DOI] [PubMed] [Google Scholar]
- 58.Vallittu PK. Fracture surface characteristics of damaged acrylic-resin-based dentures as analysed by SEM-replica technique. J Oral Rehabil. 1996;23:524–9. doi: 10.1111/j.1365-2842.1996.tb00890.x. [DOI] [PubMed] [Google Scholar]
- 59.Vallittu PK, Alakuijala P, Lassila VP, Lappalainen R. In vitro fatigue fracture of an acrylic resin-based partial denture: An exploratory study. J Prosthet Dent. 1994;72:289–95. doi: 10.1016/0022-3913(94)90342-5. [DOI] [PubMed] [Google Scholar]
- 60.Smith DC. The acrylic denture: Mechanical evaluation mid-line fracture. Br Dent J. 1961;110:257–67. [Google Scholar]
- 61.Schneider RL. Diagnosing functional complete denture fractures. J Prosthet Dent. 1985;54:809–14. doi: 10.1016/0022-3913(85)90476-7. [DOI] [PubMed] [Google Scholar]
- 62.Ohring M. How engineering materials are strengthened and toughened. In: Ohring M, editor. Engineering Materials Science. San Diego: Academic Press; 1995. pp. 431–95. [Google Scholar]
- 63.Ozen J, Spah C, Calar A, Dalkiz M. In vitro cytotoxicity of glass and carbon fiber-reinforced heat-polymerized acrylic resin denture base material. Turk Med Sci. 2006;36:121–6. [Google Scholar]