

Abstract
Aim:
The purpose of this study was to examine the prevalence of dental caries in primary dentition of 5–6-year-old children in urban and rural areas of Jabalpur city.
Materials and Methods:
The present cross-sectional study was conducted in the rural and urban areas of Jabalpur city, India. A power analysis was carried out to select a representative sample of 5–6-year-old children (n = 408), 204 from government schools and 204 from private schools. Parents were interviewed using a self-structured questionnaire to collect data with regard to variables under evaluation.
Statistical Analysis:
Collected data were subjected to descriptive analysis using the SPSS 12.0 version. Risk factor association with dental caries was investigated using a stepwise logistic regression analysis with P < 0.05 considered significant.
Results:
This shows significantly higher decayed missing filled teeth among rural children than urban children. It was seen that 46.5% of children whose mothers were illiterate were affected with dental caries. In urban area, 91.5% of children whereas 77% of children in rural area have parental control on sugar consumption.
Conclusion:
It is important to focus on parents’ education level when planning preventive programs for young children. Assessing family-related risk factors is essential when instituting preventive/treatment programs for young children.
Keywords: Dental caries, family, prevalence
Introduction
In 2003, the American Academy of Pediatric Dentistry defined Early Childhood Caries (ECC) as the presence of one or more decayed (noncavitated or cavitated), missing (due to caries), or filled tooth surfaces in any primary tooth in a child up to 71 months of age or younger. The factors responsible for ECC include a susceptible host, fermentable carbohydrate diet, presence of dental plaque, high number of cariogenic microorganisms such as Streptococcus mutans, Lactobacillus, and most importantly, time. Dietary habits, socioeconomic status (SES), working status of mother, oral hygiene habits, and frequent intake of medications are certain risk factors for this condition.[1]
Parents inculcate good habits in their children based on their own attitudes and beliefs. Various intergeneration processes connect parental oral health status with that of their offspring. Health is predominantly dictated by the caregivers at the age of 5 years. Oral health attitudes, behaviors as well as various sociodemographic factors are the choices parents make and are influenced by a variety of factors.[2]
Thus, the present study was conducted to examine the prevalence of dental caries in primary dentition of 5–6-year-old children in urban and rural areas of Jabalpur city.
Materials and Methods
The present cross-sectional study was conducted in the rural and urban areas of Jabalpur city, India. A power analysis was carried out to select a representative sample of 5–6-year-old children (n = 408), 204 from government schools and 204 from private schools. Graph 1 demonstrates the distribution of study population. The ethical clearance for conduct of the study was obtained from the Institutional Ethics Committee of Hitkarini Dental College and the various government and private schools selected for the study.
Graph 1.
Distribution of study population
Sample selection
Every third school was selected randomly using a list obtained from the local governing body. After taking necessary permission from the school administration to carry out the survey, we proceeded to select the children to be enrolled. All children aged 5–6 years and accompanied by their parent were included in the study.
Exclusion criteria comprised of those children with developmental enamel defects and systemic diseases. Distribution of study population in urban and rural areas was done according to age and gender, is elicited in Graph 2. Clinical examination was done using a mouth mirror, and a probe was only used when in doubt with minimal pressure to remove debris, under sterile conditions. The decayed missing filled teeth (dmft) indices (dmft, Greubbell, 1944) were recorded, and treatment cards were issued for those children who required treatments. Graph 3 presents with comparison of decayed missing filled teeth scores between urban and rural children.
Graph 2.
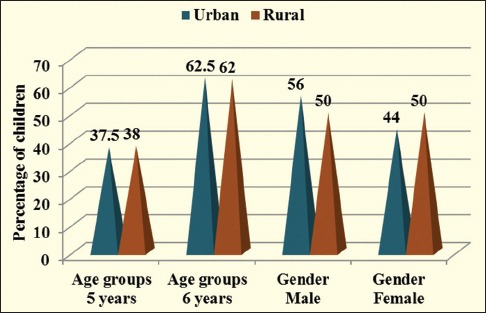
Distribution of study population in urban and rural areas according to age and gender
Graph 3.
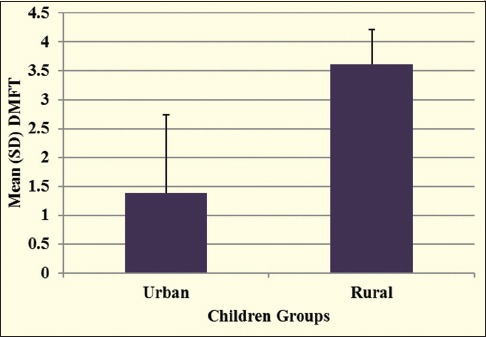
Comparison of decayed missing filled teeth scores between urban and rural children
Questionnaire
Data concerning the independent variables were collected using a self-structured questionnaire and were divided into four broad categories. Children were given questionnaire forms and were instructed to get them filled by their parents/caregivers. These questionnaires enquired about the children's personal details such as age, SES, diet, oral hygiene practices, and child's and parent's attitude toward dental awareness. Parents were provided with questionnaire in regional language (Hindi) to avoid linguistic barriers. Distribution of urban and rural children according to parent's education is demonstrated in Graph 4. It contained questions about socioeconomic, demographic data, dietary, and oral hygiene habits of children. These questionnaires were collected, and data were analyzed.
Graph 4.
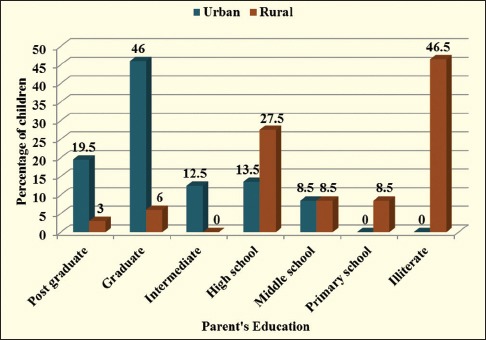
Distribution of urban and rural children according to parent's education
Sociodemographic variables
These factors were assessed by questioning parents about their occupation, educational level, and monthly income. These together were used to evaluate the parents SES using the revised version of the Kuppuswamy's SES Scale.
Family structure
These factors were assessed by questioning whether the family was nuclear or joint, how many siblings the child had, and the child order in family.
Attitudinal variables
These variables were assessed by concerning the sugar consumption, tooth brushing, and dental caries. Distribution of urban and rural children according to parental control on sugar consumption is seen in Graph 5.
Graph 5.
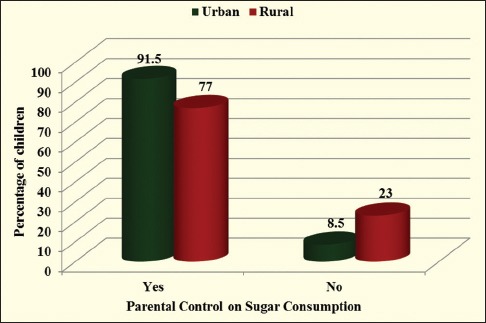
Distribution of urban and rural children according to parental control on sugar consumption
With regard to sugar consumption, the parents were asked about the frequency of sugar snacking (both snacks as well as beverages) by the child and ability of the parent to control their child's sugar consumption.
Parents’ oral hygiene and dental care-seeking behavior were also evaluated. Brushing frequency was determined and the parent was questioned whether they went for regular dental checkups.
Statistical analysis
Mean dmft, dt, mt, and ft were calculated through descriptive statistical analysis using the SPSS 12 version version (IBM Corporation). A bivariate analysis was carried out to check for association between each independent variable and the dental caries status of the child. Variables showing a significant association were then subjected to a logistic regression analysis. Odds ratio and 95% confidence interval were calculated, with P < 0.05 considered significant.
Results
Table 1 shows the characteristics of study population. No significant difference for age and gender in urban and rural children were seen in the study. The total sample dropped down to 400 after the collection of questionnaire from the various schools because the incompletely filled forms were eliminated. The mean dmft of urban population is 1.3 and the mean dmft of rural area is 3.6. It shows significantly higher dmft among rural children than urban children. It was seen that 46.5% of children whose mothers were illiterate were affected with dental caries. In urban area, 91.5% of children whereas 77% of children in rural area have parental control on sugar consumption.
Table 1.
Characteristics of study population

Discussion
In both industrialized and developing countries, ECC continues to be a significant public health problem despite the decline in dental caries in western countries, especially concentrated in deprived families.[3]
Evaluating the prevalence of dental caries in 5–6-year-old children was the primary purpose of the study. Determining the prevalence rate of caries in preschool children is a difficult process as the children of this age group are not easily accessible and are uncooperative. In accordance with previous studies, caries prevalence was seen to increase with age. Any change in their dietary habits, and oral hygiene practices pose a greater cariogenic challenge.[4]
Family-related risk factors for dental caries experience in the primary dentition were identified. According to some studies, parental employment status, dental attitudes, and dental behavior strongly influence the caries status of their 5-year-old children. A number of maternal factors have been suggested to influence child's dental health. These include mother's age, her level of education, her domicile of residence, and the family's income. The main factors associated with a child's dmft >0 in 5 years old children were - mothers’ lower level of basic education, higher number of siblings, higher snacking frequency permitted by parents, inability of parents to control sugar consumption, parents lax attitude when regulating brushing frequency, unassisted brushing by the children, and parents not brushing their own teeth twice daily.[4]
Mashoto et al. stated that social disparities in oral health outcomes constitute one of the main challenges for public health. Contemporary evidence suggests that the lower the material standard of living, the worse the health status irrespective of the measure used to assess it.[5,6,7,8] It is assumed that the effect of socioeconomic factors on oral health is mediated through environmental exposure, psychosocial factors, lifestyle, and availability of health care services.[8]
Petersen presented a risk factor model for dental caries, suggesting that socioenvironmental factors influence behavioral and attitudinal factors which in turn has an impact on clinical and subjective oral health outcomes.[9] Socioeconomic factors might influence oral health outcomes. These factors might influence oral health outcomes directly or indirectly through oral health-related behaviors. In UK, Chan et al. concluded that the socioeconomic gradient in the number of sound teeth was partially explained by dental attendance patterns.[10] However, recent studies among the US adolescents revealed that socioeconomic disparities in caries experience could not be accounted for by similar disparities in oral health behaviors.[11]
Reisine and Psoter reported an inverse relation of dental caries with social class supporting our result, along with the case–control study of Slade et al., who reported that children from low social class had 1.74-fold increased risk for dental caries.[12,13] This finding was explained by Tyagi who noted that dental caries is probably more common in lower social classes due to ignorance of parents and the poor dental hygiene practices.[14] Petersen et al. added that low perception of the need for treatment of dental caries within the socially disadvantaged section of the society places a low priority for oral health care compared to other needs.[6] This could be the reason for not restoring the teeth.[8]
Parents’ education level has been associated with the level of caries experience in their children. In our study, only the mothers’ level of education was found to be associated with the dental caries experience in their children, while no such association was seen with the fathers’ level of education. Two other studies have also observed that the mothers’ level of education, and not the fathers’, influence oral health-related quality of life. These results may have resulted from the differences in parental roles, fathers being primarily the breadwinners, and mothers being involved in child-rearing.[15] Stephen et al. stated that those children whose parents had no schooling had significantly higher nursing caries experience.[4]
Despite the decline in dental caries in western countries, ECC continues to be a significant public health problem in both industrialized and developing countries, especially concentrated in deprived families.[16]
Limitations of the study
The dmft/DMFT index can only be used for coronal caries; it cannot record root caries. Hence, underestimation of caries is possible.[17] The rate of caries progression cannot be assessed by this index which may hinder in providing proper treatment plan in the population.[18,19]
This index does not give an account of the treatment needs in a population and only records the carious and the treated lesions. Larger sample should be considered.[20]
Conclusion
During the formative years of a child's life, the foundation of lifestyle choices in adulthood is laid down. The importance of first dental visit, diet counseling, and proper oral care methods should be stringently advocated to expectant parents, new parents and preschool teachers and caregivers to inculcate lasting oral health attitudes among children. Children are dependent on their environment (that is the family) to institute favorable oral health behaviors. Thus, assessing family-related risk factors is essential when instituting preventive/treatment programs for young children.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Weinstein P, Harrison R, Benton T. Motivating parents to prevent caries in their young children: One-year findings. J Am Dent Assoc. 2004;135:731–8. doi: 10.14219/jada.archive.2004.0299. [DOI] [PubMed] [Google Scholar]
- 2.Mattila ML, Rautava P, Sillanpää M, Paunio P. Caries in five-year-old children and associations with family-related factors. J Dent Res. 2000;79:875–81. doi: 10.1177/00220345000790031501. [DOI] [PubMed] [Google Scholar]
- 3.Kuriakose S, Prasannan M, Remya KC, Kurian J, Sreejith KR. Prevalence of early childhood caries among preschool children in Trivandrum and its association with various risk factors. Contemp Clin Dent. 2015;6:69–73. doi: 10.4103/0976-237X.149295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Stephen A, Krishnan R, Ramesh M, Kumar VS. Prevalence of early childhood caries and its risk factors in 18-72 month old children in Salem, Tamil Nadu. J Int Soc Prev Community Dent. 2015;5:95–102. doi: 10.4103/2231-0762.155731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rehman MM, Mahmood N, Rehman B. The relationship of caries with oral hygiene status and extra-oral risk factors. J Ayub Med Coll Abbottabad. 2008;20:103–8. [PubMed] [Google Scholar]
- 6.Petersen PE, Hoerup N, Poomviset N, Prommajan J, Watanapa A. Oral health status and oral health behaviour of urban and rural schoolchildren in Southern Thailand. Int Dent J. 2001;51:95–102. doi: 10.1002/j.1875-595x.2001.tb00829.x. [DOI] [PubMed] [Google Scholar]
- 7.Sathe PV. A Text Book of Community Dentistry. 1st ed. Greenland Road, Ameerpet: Hyderabad Paras Medical; 1998. pp. 84–94. [Google Scholar]
- 8.Mashoto KO, Astrom AN, Skeie MS, Masalu JR. Socio-demographic disparity in oral health among the poor: A cross sectional study of early adolescents in Kilwa district, Tanzania. BMC Oral Health. 2010;10:7. doi: 10.1186/1472-6831-10-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kiwanuka SN, Astrøm AN, Trovik TA. Dental caries experience and its relationship to social and behavioural factors among 3-5-year-old children in Uganda. Int J Paediatr Dent. 2004;14:336–46. doi: 10.1111/j.1365-263X.2004.00570.x. [DOI] [PubMed] [Google Scholar]
- 10.Chan SC, Tsai JS, King NM. Feeding and oral hygiene habits of preschool children in Hong Kong and their caregivers’ dental knowledge and attitudes. Int J Paediatr Dent. 2002;12:322–31. doi: 10.1046/j.1365-263x.2002.00389.x. [DOI] [PubMed] [Google Scholar]
- 11.Mahejabeen R, Sudha P, Kulkarni SS, Anegundi R. Dental caries prevalence among preschool children of Hubli: Dharwad city. J Indian Soc Pedod Prev Dent. 2006;24:19–22. doi: 10.4103/0970-4388.22829. [DOI] [PubMed] [Google Scholar]
- 12.Reisine ST, Psoter W. Socioeconomic status and selected behavioral determinants as risk factors for dental caries. J Dent Educ. 2001;65:1009–16. [PubMed] [Google Scholar]
- 13.Slade GD, Sanders AE, Bill CJ, Do LG. Risk factors for dental caries in the five-year-old South Australian population. Aust Dent J. 2006;51:130–9. doi: 10.1111/j.1834-7819.2006.tb00416.x. [DOI] [PubMed] [Google Scholar]
- 14.Tyagi R. The prevalence of nursing caries in Davangere preschool children and its relationship with feeding practices and socioeconomic status of the family. J Indian Soc Pedod Prev Dent. 2008;26:153–7. doi: 10.4103/0970-4388.44030. [DOI] [PubMed] [Google Scholar]
- 15.Sujlana A, Pannu PK. Family related factors associated with caries prevalence in the primary dentition of five-year-old children. J Indian Soc Pedod Prev Dent. 2015;33:83–7. doi: 10.4103/0970-4388.155108. [DOI] [PubMed] [Google Scholar]
- 16.Ramamurthy PH, Swamy HS, Bennete F, Rohini M, Nagarathnamma T. Relationship between severe-early childhood caries, salivary mutans streptococci, and lactobacilli in preschool children of low socioeconomic status in Bengaluru city. J Indian Soc Pedod Prev Dent. 2014;32:44–7. doi: 10.4103/0970-4388.127054. [DOI] [PubMed] [Google Scholar]
- 17.Brizon VS, Rojas GC, Ambrosano GM, Guerra LM, Pereira AC. Association of dental caries experience with individual and contextual variables in Brazilian children. Eur J Gen Dent. 2016;5:104–10. [Google Scholar]
- 18.Gokhale N, Nuvvula S. Influence of socioeconomic and working status of the parents on the incidence of their children's dental caries. J Nat Sci Biol Med. 2016;7:127–9. doi: 10.4103/0976-9668.184697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Borges HC, Garbín CA, Saliba O, Saliba NA, Moimaz SA. Socio-behavioral factors influence prevalence and severity of dental caries in children with primary dentition. Braz Oral Res. 2012;26:564–70. doi: 10.1590/s1806-83242012000600013. [DOI] [PubMed] [Google Scholar]
- 20.Bhatia HP, Srivastava B, Khatri S, Aggarwal A, Singh AK, Gupta N. Prevalence of dental caries among 3-15 year old school children in Ghaziabad city and its adjoining areas – A correlated survey. J Oral Health Community Dent. 2012;6:135–40. [Google Scholar]