

Abstract
Hemifacial hyperplasia is a rare developmental anomaly characterized by marked unilateral facial tissues. It involves orofacial soft tissues, bones of the face, and teeth. The cause remains ambiguous although several predisposing factors have been reported. A case report of a 32-year-old girl with unilateral hemifacial enlargement, pain in temporomandibular joint, and limited mouth opening associated is presented to highlight the clinical and imaging findings and to discuss the differential diagnosis.
Keywords: Congenital anomaly, facial asymmetry, hemifacial hyperplasia
Introduction
Hemifacial hyperplasia (HFH) is a rare congenital developmental disorder characterized by asymmetrical overgrowth of one or more body parts. HFH was initially described by Meckel in 1822 and later reported by Wagner in 1839.[1] HFH affects the facial soft tissues, bone, and the associated structures.[2] It has been reported that first case of HFH was described in 1863 by Beck.[3] Asymmetry in HFH is usually obvious at birth and accentuated at the end of adolescence. The prevalence rate of HFH is 1:86,000 live births.[4] Rowe developed an anatomic classification of hemihyperplasia into simple hemihyperplasia, which involves a single limb, complex hemihyperplasia, which involves half of the body, and HFH, which involves one side of the face.[5] Rowe further subclassified HFH into (1) true hemifacial hyperplasia (TFHF), presenting unilateral enlargement of the viscerocranium extending superiorly from the frontal bone (not including the eye) to the inferior border of the mandible and from the midline to the pinna of the ear with enlargement of all soft tissues, teeth, and bone in the area and (2) partial hemifacial hypertrophy (PHFH) if the enlargement is limited to one structure.
Case Report
A 32-year-old healthy female presented to a clinic (LS). The main complaint was severe pain in right temporomandibular joint (TMJ) region, right ear, mouth opening limitation, and asymmetrical of the face. The patient reported that she was born at full term by spontaneous vaginal delivery and no perinatal problems and no notable postnatal illness were reported. However, in the months following birth, the parents observed progressive enlargement of her right cheek and a differing eyelid width. According to the patient, the facial asymmetry had become more marked over the following years but had not increased in the past few years. No other family members were affected. Patient's mother reported a normal pregnancy. The enlargement extended from the midline to the preauricular region and inferiorly to the lower border of mandible [Figure 1]. The skin of the involved right side of the face was normal in appearance with no alteration in thickness. The extraoral examination revealed that the right side of the mandible was larger than the left side. The outer contour of the right ear was slightly larger and had a different shape compared to that of the left side [Figure 2]. The nose was normal with no deviation although the chin was deviated toward the side of her face. The lower lip on the right side was appeared thicker with drooping of the corner of the mouth on this side. The lips on the right side seemed very dry. The patient complained clicking in the left TMJ and disability in chewing and headache in the right side. Physical examination revealed normal symmetric body. The patient was mentally healthy. The mouth opening was 12 mm. On intraoral examination, asymmetry of the tongue was evident [Figure 3]. The right part of the tongue shows unilateral enlargement of fungiform papillae. The teeth size on the affected side appeared normal except the dimensions of maxillary right first molar, which was considerably greater than maxillary left first molar. The size of the lower right first molar was slightly greater than lower left first molar. The lower dental centerline was deviated to the right in relation to the midline and a downward canting of the occlusal plane was observed [Figure 4]. On occlusal examination, the central relation was unattainable. Furthermore, there was early contact in both central occlusion and right lateral movement. A discrepancy in range of mandibular motion was observed. The patient was referred for radiography. The radiographs confirmed the clinical findings. The panoramic radiograph [Figure 5] showed that the right condyle, ramus, condylar neck, and the body of the mandible were enlarged. There was significant deposition of bone growth on the right mandible, and the bony trabeculation alteration was observed. The size of the right inferior dental canal was normal compared to the left mandibular canal and was displaced. Crowns and roots of the right mandibular molars were larger than the contralateral mandibular molars. The roots of the lower right first and second molars were remarkably divergent. Cone-beam computed tomography (CBCT) images of the face and skull revealed that the zygomatic and frontal bones, right mastoid process, right half of the mandible and maxilla, maxillary sinus, and associated soft tissues were enlarged [Figure 6a and b]. CBCT also demonstrated thickening the mucosal membrane of the right maxillary sinus [Figure 7a and b]. There was no obstruction in the sinus meatus. Brain computed tomography (CT) showed no abnormalities [Figure 8a and b]. 3D skull reconstruction CT image revealed hypertrophy of the right mandible, condyle, TMJ, zygomatic bone, petrous bone, and mastoid process [Figure 9]. The posteroanterior radiograph [Figure 10] revealed enlargement of right half of the mandible, maxilla, and zygoma. The patient was referred to physician. Physician consultation reported systemic abnormality. Blood investigations were within normal limits. Depending on the clinical and radiographic abnormalities were thus consistent with the diagnosis of a hemifacial hypertrophy and fibrous hyperplasia. The patient was referred to oral surgeon. Surgical recontouring of right maxillary and mandibular bone was performed. After 6 months, condylectomy was performed for the right condyle; the size of the condyle was 5 cm × 3 cm [Figure 11]. The mouth opening was significantly increased to 4 cm.
Figure 1.
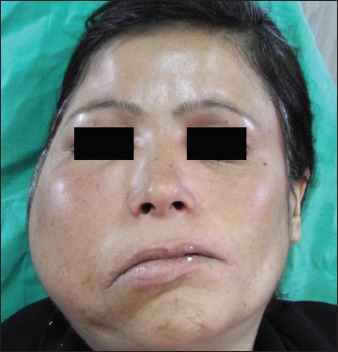
Demonstrated facial asymmetry
Figure 2.

The outer contour of the right ear is slightly larger than the left ear
Figure 3.

Asymmetry of the tongue. The right part of the tongue shows a peculiar picture of enlargement of fungiform papillae with unilateral enlargement and contralateral displacement
Figure 4.

Dental casts
Figure 5.

Panoramic radiograph showing hyperplasia of right ramus, right body of the mandible, condyle and condylar neck
Figure 6.
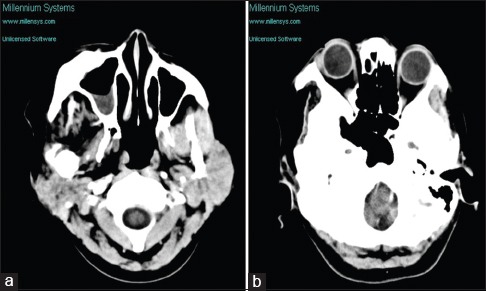
(a and b) Axial plane: Computed tomography view shows irregular and hyperdense growth of the right hemiface with involvement of the zygomatic, temporal and maxillary process, sphenoid, occipital bone, maxilla (enlargement of the cheek and palate), mandibular ramus and condyle
Figure 7.
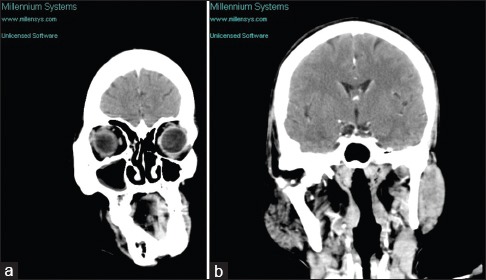
(a and b) Coronal section computed tomography view showing hypoplasia of the left maxillary antrum
Figure 8.
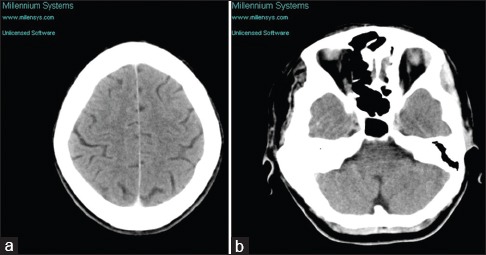
(a and b) Brain computed tomography shows no abnormalities
Figure 9.
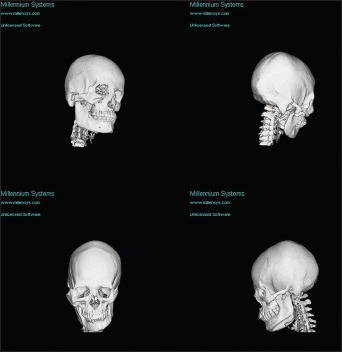
3D reconstructed computed tomography images of the skull showing facial asymmetry, hypertrophy of the right mandible, condyle, temporomandibular joint, zygomatic bone, petrous bone, and mastoid process
Figure 10.
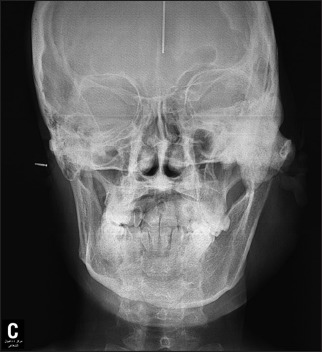
Posteroanterior cephalometric film revealed a prominent distortion of the right hemimandible and deformation right ramus and body of the mandible
Figure 11.

Panoramic radiograph shows condylectomy of the right condyle
Discussion
HFH is a congenital morphological anomaly that causes facial asymmetry resulting from unilateral overgrowth of all tissues or part of the tissues on the affected side including soft tissues, bone, and teeth.[5] The etiology of HFH is unknown. Over the last decades, several theories were suggested. However, a number of possible etiologic factors have been suggested including endocrine dysfunctions, chromosomal abnormalities,[4] central nervous system disorders,[6] vascular or lymphatic malformations, and somatic mutations.[4] Few studies supported heredity as a potential cause.[7] Another study suggested disturbances in the development of the first branchial arch overgrowth.[8] An embryological hypothesis put forth by Pollock et al. postulates increased number of neural crest cells on the enlarged half of the neural tube.[9] The increased number of crest cells continues through pre- and post-natal growth periods of life and resulting in unilateral overgrowth of the crest-derived structures. Gesell attributed congenital hemihyperplasia to deviation from normal process of twinning which suggests an inequality of regulatory abilities in embryologic development leading to an aberrant twinning mechanism.[10] Noe and Berman postulated as the main cause damage of mitochondria in an overripe one half of the fertilized egg resulting in over generation of cells.[11] Yoshimoto et al. concluded that the pathogenesis is thought to be due to basic fibroblast growth factor along with its receptor-stimulated osteoblastic differentiation on the affected side in comparison with the normal part of the face.[12] In 2015 study, Yamazaki et al. reported that facial overgrowth may result from a downregulation of phosphatase-tensin homolog transcripts.[13] Histologically, according to Pollock et al., the overgrowth process involves an increase in number of cells rather than in size.[9] Hence, hemifacial hypertrophy is more accurately termed HFH. Depending on Row's classification, our case report shows a PHFH since he had unilateral overgrowth of the orofacial soft tissues and bones and tongue asymmetry. HFH affects men more often than women[5] with marked predilection for right-sided involvement. Lee reported that partial HFH is even rarer than TFHF.[4] HFH is associated with several abnormalities such as enlargement of hard tissue and soft tissue on the affected side. Soft tissue anomalies include lips, buccal mucosa, uvula, and tonsils. Tongue frequently exhibits unilateral enlargement with thickened and hypertrophic fungiform papillae.[14] Miles reported velvety and soft pendulous folds in the involved buccal mucosa.[15] Extraorally, the skin did not exhibit any kind of abnormality on the involved side; this is in agreement with the findings of Gorlin and Meskin[16] and Lawoyin et al.[17] Furthermore, ipsilateral pinna enlargement has not been reported.[9] However, our patient exhibits enlargement of pinna on the affected side. In our case, nasal septum deviation was not observed. This is inconsistent with finding of Oktay et al.[18] However, this finding was as a result of involvement of the facial musculature around the nasolabial fold and hypertrophied turbinates on the affected side.[19] In respect of unilateral distribution of dental abnormalities, rate of development, crown size, root size, and shape are the most prominent features characteristic of HFH.[1] Our case demonstrated a distinct tooth and root size discrepancies were noted between right and left side. In cervicoincisal, mesiodistal, and labiolingual dimensions, significant difference was observed between size of crowns of the right and left teeth. This finding is consistent with Row study.[5] Moreover, root size and shape of the right mandibular molars are larger than their contralateral counterparts. Since most of the features of partial HFH are generally manifested in the orofacial region, the differential diagnoses of the following partial hyperplasia should be considered: CLOVES Syndrome, Klippel–Trenaunay syndrome, which associated with capillary-lymphatic-venous deformation, fibrous dysplasia, and other overgrowth syndromes. However, partial HFH exhibits sufficient clinical differences. Treatment of HFH is generally for cosmetic considerations. The main objective is to follow the patient up for prolonged period until the growth has ceased. HFH is generally associated with good prognosis.
Conclusion
Report of a cases of hemifacial hypertrophy associated with fibrous dysplasia is presented. This entity is rare and difficult to diagnose. An accurate diagnosis can be made from clinical and radiographic information, but only if one is aware of the differentiating criteria.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Khanna JN, Andrade NN. Hemifacial hypertrophy. Report of two cases. Int J Oral Maxillofac Surg. 1989;18:294–7. doi: 10.1016/s0901-5027(89)80098-0. [DOI] [PubMed] [Google Scholar]
- 2.Islam MN, Bhattacharyya I, Ojha J, Bober K, Cohen DM, Green JG. Comparison between true and partial hemifacial hypertrophy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:501–9. doi: 10.1016/j.tripleo.2006.11.053. [DOI] [PubMed] [Google Scholar]
- 3.Urban PP, Bruening R. Congenital isolated hemifacial hyperplasia. J Neurol. 2009;256:1566–9. doi: 10.1007/s00415-009-5148-9. [DOI] [PubMed] [Google Scholar]
- 4.Lee S, Sze R, Murakami C, Gruss J, Cunningham M. Hemifacial myohyperplasia: Description of a new syndrome. Am J Med Genet. 2001;103:326–33. [PubMed] [Google Scholar]
- 5.Rowe NH. Hemifacial hypertrophy. Review of the literature and addition of four cases. Oral Surg Oral Med Oral Pathol. 1962;15:572–87. doi: 10.1016/0030-4220(62)90177-9. [DOI] [PubMed] [Google Scholar]
- 6.Cohen MM., Jr Perspectives on craniofacial asymmetry. IV Hemi-asymmetries. Int J Oral Maxillofac Surg. 1995;24:134–41. doi: 10.1016/s0901-5027(06)80086-x. [DOI] [PubMed] [Google Scholar]
- 7.Rudolph CE, Norvold RW. Congenital partial hemihypertrophy involving marked malocclusion. J Dent Res. 1944;23:133–9. [Google Scholar]
- 8.Horswell BB, Holmes AD, Barnett JS, Hookey SR. Primary hemihypertrophy of the face: Review and report of two cases. J Oral Maxillofac Surg. 1987;45:217–22. doi: 10.1016/0278-2391(87)90118-2. [DOI] [PubMed] [Google Scholar]
- 9.Pollock RA, Newman MH, Burdi AR, Condit DP. Congenital hemifacial hyperplasia: An embryologic hypothesis and case report. Cleft Palate J. 1985;22:173–84. [PubMed] [Google Scholar]
- 10.Gessel A. Hemihypertrophy and twinning. Am J Med Sci. 1927;173:542. [Google Scholar]
- 11.Noe O, Berman HH. The etiology of congenital hemihypertrophy and one case report. Arch Pediatr. 1962;79:278–88. [PubMed] [Google Scholar]
- 12.Yoshimoto H, Yano H, Kobayashi K, Hirano A, Motomura K, Ohtsuru A, et al. Increased proliferative activity of osteoblasts in congenital hemifacial hypertrophy. Plast Reconstr Surg. 1998;102:1605–10. doi: 10.1097/00006534-199810000-00041. [DOI] [PubMed] [Google Scholar]
- 13.Yamazaki K, Eng C, Kuznetsov SA, Reinisch J, Yamashita DD, Walker J, et al. Missense mutation in the PTEN promoter of a patient with hemifacial hyperplasia. Bonekey Rep. 2015;4:654. doi: 10.1038/bonekey.2015.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Azevedo RA, Souza VF, Sarmento VA, Santos JN. Hemifacial hyperplasia: A case report. Quintessence Int. 2005;36:483–6. [PubMed] [Google Scholar]
- 15.Miles AE. A case of unilateral gigantism of the face and teeth. Br Dent J. 1944;77:197–9. [Google Scholar]
- 16.Gorlin RJ, Meskin LH. Congenital hemihypertrophy. Review of the literature and report of a case with special emphasis on oral manifestations. J Pediatr. 1962;61:870–9. doi: 10.1016/s0022-3476(62)80198-x. [DOI] [PubMed] [Google Scholar]
- 17.Lawoyin JO, Daramola JO, Lawoyin DO. Congenital hemifacial hypertrophy. Report of two cases. Oral Surg Oral Med Oral Pathol. 1989;68:27–30. doi: 10.1016/0030-4220(89)90110-2. [DOI] [PubMed] [Google Scholar]
- 18.Oktay MF, Topcu I, McKinney A, Turunz V, Aras O. Isolated hemifacial hypertrophy: A case with upper airway obstruction and sensorineural hearing loss. J Laryngol Otol. 2006;120:691–3. doi: 10.1017/S0022215106001381. [DOI] [PubMed] [Google Scholar]
- 19.Bou-Haidar P, Taub P, Som P. Hemifacial lipomatosis, a possible subtype of partial hemifacial hyperplasia: CT and MR imaging findings. AJNR Am J Neuroradiol. 2010;31:891–3. doi: 10.3174/ajnr.A1857. [DOI] [PMC free article] [PubMed] [Google Scholar]