

Abstract
Hemangiomas of the rib are extremely rare benign neoplasm. Here we present a case in a 47-year-old female, detected by chest X-ray and underwent a surgical resection. Histologically, the tumor was composed of a homogeneous conglomerate, irregular, thin walled and dilated blood vessels containing red blood cells, supported by fibrous stroma and intermingled to regular bone trabeculae. The postoperative courses were uneventful, and there was no recurrence during 64 months follow-up.
Keywords: Hemangioma, Rib, Surgery, Histopathology
1. Introduction
Hemangiomas are benign vascular tumors that usually involve the skin, liver, eyes and central nervous system. Bone hemangiomas have low incidence, accounting for 1% of all bone tumors [1]. They are predominantly found in the spine and skull while uncommonly observed in the ribs or long bones [2]. Hemangiomas of the rib usually expansively grow and disrupt the cortex thus they can be misdiagnosed as aggressive tumors or infectious processes [3]. Though the reports in the literature are sporadic, rib hemangioma is part of the differential diagnosis of chest wall tumors [4-7]. In the current study, we illustrated the manner of presentation, imaging, treatment and pathology of this unusual tumor, and then carry out a thorough literature review.
2. Case report
An asymptomatic 47-year-old female with no medical history or history of trauma to the chest wall was admitted due to a bone tumor in the right seventh rib which was incidentally discovered on routine chest X-ray in November 2007 (Figure 1). No abnormality was found in the physical examination. Electrocardiography was normal and blood laboratory test showed within normal limits including biochemistry, coagulation routine hematology. Computed tomography (CT) demonstrated a localized mass, measuring 65.0×45.0 mm, expansile with disrupted cortex and coarse trabeculae with a “honeycomb” appearance along the inner surface of the right seventh posterior rib (Figure 2). Emission Computed Tomography (ECT) showed radionuclide uptake on the right seventh posterior rib (Figure 3). On November 23, 2007, the patient underwent resection of the mass through a right posterolateral thoracotomy and en bloc resection of the posterior portions of rib seven and associated soft tissue. To reduce the likelihood of local tumor recurrence, frozen sections should be made to ensure that the resected margins are free of tumor. Uneventful postoperative course was found with the patient and recovered quickly. The patient did not receive radiation therapy or chemotherapy postoperatively. No recurrence of the tumor was found by CT scanning during 64 months follow-up.
Figure 1.
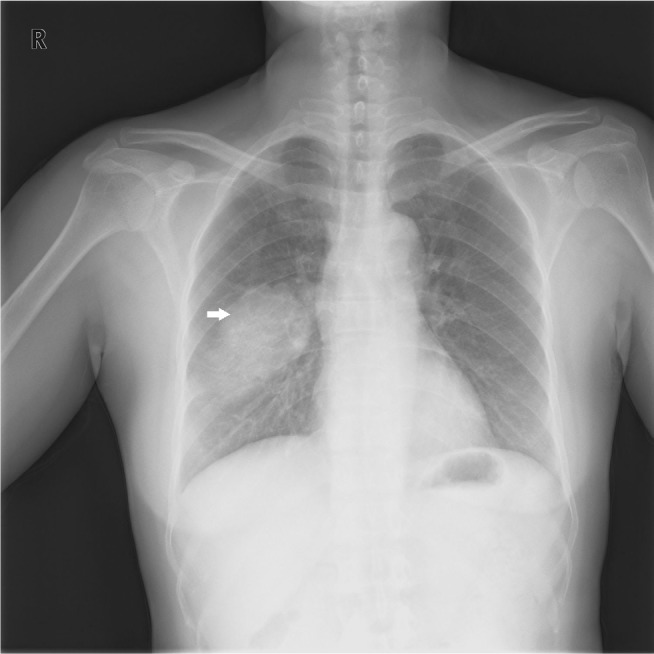
Chest radiograph revealed lesion on the right seventh rib (arrow).
Figure 2.
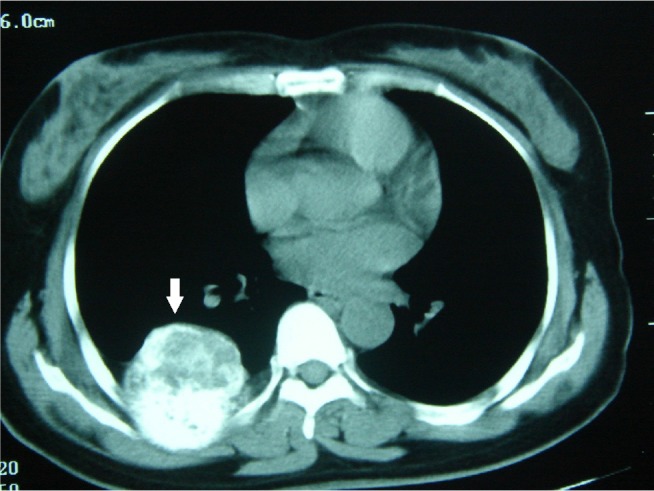
Chest computed tomography scan showed the localized expansive and heterogeneous growth of the tumor projecting toward the thoracic cavity (arrow).
Figure 3.
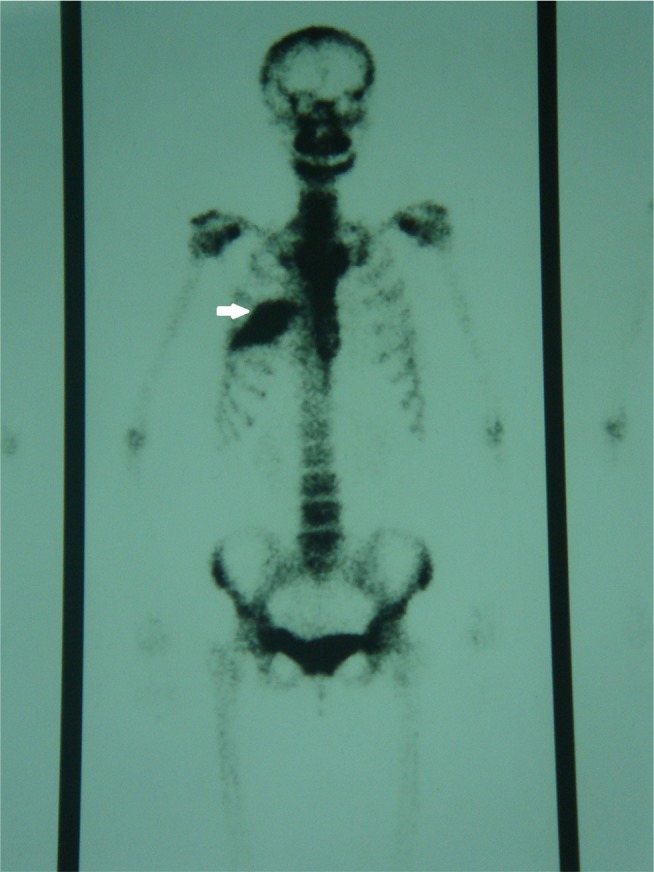
Emission Computed Tomography showed radionuclide uptake on the right seventh posterior rib (arrow).
Ethical approval: The research related to human use has been complied with all the relevant national regulations, institutional policies and in accordance the tenets of the Helsinki Declaration, and has been approved by the authors’ institutional review board or equivalent committee.
Informed consent: Informed consent has been obtained from all individuals included in this study.
3. Histopathology
Gross examination of the tumor measured 65.0×45.0×40.0 mm and identified bulging from the inner aspect of the seventh rib toward the thoracic cavity. The surface of the tumor was covered with a smooth pleura and no tumor extension beyond the membrane was observed. The specimen was fixed with 4% neutral formaldehyde and conventionally made into paraffin sections. HE staining was performed. Microscopic examination showed that the tumor was composed of a homogeneous conglomerate, irregular, thin walled and dilated blood vessels containing red blood cells, supported by fibrous stroma, and intermingled with regular bone trabeculae (Figure 4). There was no necrosis in the tumor. The pathologic diagnosis of this tumor was hemangioma of the rib. No tumor tissue was detected at the surgical margin.
Figure 4.

A Microscopic examination revealed thin walled and dilated blood vessels containing red blood cells and bone trabeculae (HE×100).
B Microscopic examination revealed homogeneous conglomerate, irregular, thin walled and dilated blood vessels containing red blood cells, supported by fibrous stroma, and intermingled to regular bone trabeculae (HE×200).Green arrow: blood vessels containing red blood cells. Black arrow: bone trabeculae. Blue arrow: homogeneous conglomerate. Red arrow: fibrous stroma.
4. Discussion
Hemangioma is defined as a neoplastic entity which arises from blood vessels. Although skin is the most common primary site of hemangioma, other organs including the bone can be affected. There are two types of hemangiomas in histology: cavernous and capillary. The cavernous type consists of large dilated vessels lined by a single layer of endothelial cells surrounded by a fibrous stroma layer. The capillary hemangioma, which is less common, shows numerous tortuous small vascular channels lined with epithelium [8]. Bone hemangiomas are benign tumors of vascular origin and are mostly incidental findings in middle aged females [9]. The majority of the rib hemangioma were solitary tumors and half of them were reported as asymptomatic [10]. Occasionally they may present with pain and swelling when associated with a pathological fracture. In addition, few of them presented with rapid accumulation of one-sided pleural effusion mimicking malignant pleurisy [11].
Hemangiomas of the rib are usually discovered incidentally during a chest radiograph examination. The size of tumor and the extent of cortical destruction can be identified more clearly by chest CT and magnetic resonance imaging (MRI). Usually rib hemangiomas in imaging are characteristically expansile and well circumscribed, with a thin, intact bony cortex. While some rib hemangiomas in imaging showed a sunburst appearance or disruption of the bony cortex with extraosseous extension, or both, although these are generally malignant findings [8,12]. Honeycomb appearance to the medullary cavity of the rib is also common [12]. By MRI, hemangiomas of the rib typically have a long relaxation time at T1 and T2-weighted and have low to intermediate signal on T1-weighted images and high signal on T2-weighted images [13].
Hemangiomas are often misdiagnosed due to rare occurrence in the ribs. 89% of rib tumors are malignant [4]. Cortical disruption appearance of rib hemangioma can give the false impression of aggressive behavior. The differential diagnosis of hemangioma of the rib may include metastatic and primary malignant tumors (chondrosarcoma, osteogenic sarcoma, myeloma, and Ewing sarcoma) or benign tumors (fibrous dysplasia, osteochondroma, aneurismal bone cyst and eosinophilic granuloma) [8]. There was reported in literature that hemangioma of the rib was diagnosed preoperatively by percutaneous needle biopsy which is safe and useful in obtaining a definite diagnosis [6, 12]. On the other hand, some authors advocate that needle biopsy should be avoided due to the risk of seeding the needle tract and significant bleeding, unless multiple myeloma or metastatic disease is highly suspected [14]. When hemangioma of the rib is strongly suspected, complete resection of the rib lesion should be considered. However, the diagnosis can only be confirmed by histopathological examination. Some other management options for symptomatic hemangiomas include radiotherapy, transarterial embolization and alcohol injection [14].
Acknowledgement
This work was supported by Science and Technology Planning Project of Zhejiang Province, China 2015C33194.
Footnotes
Conflict of interest: None has any conflict of interest.
References
- [1].Okumura T, Asamura H, Kondo H. et al. Hemangioma of the rib: a case report[J] Jpn J Clin Oncol. 2000;30(8):354–357. doi: 10.1093/jjco/hyd097. [DOI] [PubMed] [Google Scholar]
- [2].Ching BC, Wong JS, Tan MH. et al. The many faces of intraosseous haemangioma: a diagnostic headache[J] Singapore Med J. 2009;50(5):e195–198. [PubMed] [Google Scholar]
- [3].Tew K, Constantine S, Lew WY. Intraosseous hemangioma of the rib mimicking an aggressive chest wall tumor[J] Diagn Interv Radiol. 2011;17(2):118–121. doi: 10.4261/1305-3825.DIR.3031-09.2. [DOI] [PubMed] [Google Scholar]
- [4].Ulku R, Onat S, Avci A. et al. Resection of intercostal hemangioma with involved chest wall and ribs: in an 11-year-old girl[J] Tex Heart Inst J. 2010;37(4):486–489. [PMC free article] [PubMed] [Google Scholar]
- [5].Constans T, Denis C, Bacq Y. et al. Cavernous hemangioma of the ribs with hyperthermia[J] Rev Med Interne. 1988;9(2):194–195. doi: 10.1016/s0248-8663(88)80122-x. [DOI] [PubMed] [Google Scholar]
- [6].Kiss T, Magony J.. Cavernous hemangioma of the ribs[J] Magy Seb. 1963;16:377–380. [PubMed] [Google Scholar]
- [7].Trefftz F, Bellmann G.. Contribution to bone hemangioma(hemangioma of the ribs in polyostotic hemangioma)[J] Med Monatsschr. 1964;18:75–77. [PubMed] [Google Scholar]
- [8].Ceberut K, Aksoy YM, Savas F. et al. Cavernous hemangioma of the rib: a case report[J] Asian Cardiovasc Thorac Ann. 2008;16(3):e25–27. doi: 10.1177/021849230801600324. [DOI] [PubMed] [Google Scholar]
- [9].Jain SK, Songra M, Malhotra A. et al. Rib haemangioma: a rare differential for rib tumours[J] Indian J Surg. 2011;73(6):447–449. doi: 10.1007/s12262-011-0278-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Nakamura H, Kawasaki N, Taguchi M. et al. Cavernous hemangioma of the rib diagnosed preoperatively by percutaneous needle biopsy[J] Gen Thorac Cardiovasc Surg. 2007;55(3):134–137. doi: 10.1007/s11748-006-0086-2. [DOI] [PubMed] [Google Scholar]
- [11].Hashimoto N, Takenaka S, Akimoto Y. et al. Capillary hemangioma in a rib presenting as large pleural effusion[J] Ann Thorac Surg. 2011;91(4):e59–61. doi: 10.1016/j.athoracsur.2010.11.074. [DOI] [PubMed] [Google Scholar]
- [12].Roy L, Isler M.. Surgical images: musculoskeletal. Costal hemangioma presenting as rib pain after pneumonia[J] Can J Surg. 2005;48(2):152. [PMC free article] [PubMed] [Google Scholar]
- [13].Tateishi U, Gladish GW, Kusumoto M. et al. Chest wall tumors: radiologic findings and pathologic correlation: part 1. Benign tumors[J] Radiographics. 2003;23(6):1477–1490. doi: 10.1148/rg.236015526. [DOI] [PubMed] [Google Scholar]
- [14].Ogose A, Hotta T, Morita T. et al. Solitary osseous hemangioma outside the spinal and craniofacial bones[J] Arch Orthop Trauma Surg. 2000;120(5-6):262–266. doi: 10.1007/s004020050461. [DOI] [PubMed] [Google Scholar]