

Abstract
Aim:
The aim of the study is to assess the efficacy of Calendula officinalis gel as cost-effective treatment modality in comparison to lycopene gel in the treatment of leukoplakia.
Materials and Methods:
The study comprised of sixty patients of clinically diagnosed and histopathologically confirmed cases of homogeneous leukoplakia which were divided into Group I and Group II with thirty patients each. Group I patients were dispensed C. officinalis extract gel whereas Group II patients were given lycopene gel. The therapy was instituted for 1 month to assess the change in the size of the lesion at the baseline and posttreatment.
Results:
The results revealed a statistically significant difference in both Group I and Group II when the pre- and post-treatment results were compared in the same group. The mean difference in the reduction in size before and after treatment for Group I was 2.0% ±1.0 cm while for the Group II, it was 1.57% ±0.87 cm. The intergroup comparison for the evaluation of reduction in the size of the lesion did not reveal statistically significant results.
Conclusion:
C. officinalis extract gel can be effectively used as an alternative to conventional treatment modality.
Keywords: Calendula officinalis, leukoplakia, lycopene
INTRODUCTION
Oral leukoplakia (OL) is one among important potentially malignant disorders of the oral mucosa.[1,2] Leukoplakia may occur anywhere on the oral mucosa, and its prevalence varies from 0.2% to 5.2% of the Indian population.[3,4] The tobacco chewing habit both in smoking and smokeless form is the most common cause for OL. Many oral squamous cell carcinomas develop from potentially malignant disorders.[5] It has been reported that between 16% and 62% of oral squamous cell carcinomas are associated with OL.[2,6] Early diagnosis and treatment of these potentially malignant disorders is required to prevent their progression to malignancy. Hence, it is important for the clinician to diagnose leukoplakia in its initial stages and manage effectively.
Current treatment modalities include cessation of tobacco chewing habit and lycopene as a powerful antioxidant, a member of carotenoid family of phytochemicals obtained from tomatoes, other red fruits and vegetables (red carrots, watermelons, papayas).[7] Lycopene exhibits the highest physical quenching rate constant with singlet oxygen, thereby known for its antioxidizing property.[8] The conjugated polyene structure of lycopene provides an electron-rich system which neutralizes harmful free radicals and prevents cell death.[9] Tomato products and lycopene consumption reduce the risk of upper aerodigestive tract cancers of oral cavities, pharynx, larynx, and esophagus.[10] The ability of lycopene is supposed to modify intercellular exchange junctions, thereby effective in potentially malignant disorders.[11]
Many herbal medicines have been tried in the management of oral diseases including premalignant disorders. Calendula officinalis is one among the herbal medicines which has the potential antioxidant property. C. officinalis also known as pot marigold is an annual herb belonging to family Asteraceae.[12] Pharmacological studies have confirmed that C. officinalis has a broad range of biological activity such as antimicrobial, anti-inflammatory, immunomodulatory, wound healing, antiviral, and antitumoral property.[13]
Research has shown that C. officinalis contains flavonoids, polyphenols, lutein, flavoxanthin, lycopene, auroxanthin, beta-carotene which possesses antioxidant property[14] and hence can be utilized in the treatment of leukoplakia. In the light of above properties of C. officinalis, this study was proposed to assess the effect of herbal gel in treatment of homogeneous leukoplakia. This gel is a cost-effective treatment modality when compared with lycopene gel for the treatment of homogeneous leukoplakia.
MATERIALS AND METHODS
Sixty patients of either sex with clinically diagnosed and histopathologically confirmed cases of homogeneous leukoplakia were selected reporting to the Department of Oral Medicine and Radiology, KLE Vishwanath Katti Institute of Dental Sciences and Research Centre, Belagavi. Informed consent was obtained from all the patients, and approval was seeked from the Institutional Ethical Committee and review board of KLE Vishwanath Katti Institute of Dental Sciences, Belagavi. Individuals willing to participate in the study with the signed informed consent were included in the study. Patients with potentially malignant disorders other than homogeneous leukoplakia, any past history of major illness within a period of 6 months, allergy to Asteraceae family and lycopene were excluded from the study.
Patients included 60 clinically and histopathologically confirmed cases of homogeneous leukoplakia based on the classification given by Warnakulasuriya S et al. (2007)[15] which were randomly divided into following 2 Groups with thirty patients each. Patients in Group I were dispensed C. officinalis gel containing antioxidants 2 mg by weight, per gram of gel. Patients in Group II were dispensed lycopene gel containing lycopene antioxidant 2 mg by weight, per gram of gel.
The double-blinded protocol was followed in which both the patient and the investigator were unknown about the medication given. Tobacco cessation counseling was done for all the patients at the very first appointment and they were instructed to apply the gel thrice daily after breakfast, lunch and dinner for a period of 1 month [Figure 1]. Both the gels were dispensed in a sterile plastic bottle with a nozzle. Patients were instructed to use sterile ear buds for gel application at the site of the lesion. Patients were also demonstrated about the quantity and method of gel application on the lesion at the first appointment itself.
Figure 1.

Application of gel at the site of lesion
The therapy was followed up for the next 3 months. Patients were examined on the 30th day to assess the change in the size of the lesion at the baseline [Figure 2] and posttreatment [Figure 3]. The evaluation of the treatment was assessed by quantitative bidimensional measurement using clinical photographs of the lesion and measuring the size of the lesion by Photoshop software version 5. The two longest diameters calculated by the software were used to calculate the total size of the lesion. The measurements were done twice, first at the baseline (before application of the gel) and at the posttreatment (end of 1 month). The data obtained were statistically analyzed using paired t-test to evaluate the correlation in C. officinalis group and lycopene group (pre- and post-treatment), and unpaired t-test was done to evaluate the correlation between C. officinalis and lycopene group (posttreatment).
Figure 2.

Pretreatment homogeneous leukoplakia
Figure 3.

Posttreatment after application of C. officinalis gel
Gel preparation
C. officinalis flowers were collected from Horticulture Department (Civil) NTPC Barh, Patna, during November 2015. Flowers were authenticated by the trained and experienced faculty of Regional Medical Research Centre, Nehru Nagar, Belagavi, and the herbarium specimen was deposited at ICMR with accession number RMRC-1280. Other chemicals such as Hydroxymethyl propyl cellulose, methyl paraben, and propyl paraben used in the formulations were of analytical grade procured from the local dealers at Belagavi. The material for lycopene gel was procured from Lycored Jagsonpal Pharmaceutics Limited. C. officinalis and lycopene gels were prepared in the Department of Pharmaceutics, KLEU college of Pharmacy, Belagavi.
Per gram of Calendula officinalis gel contained
Compound extract-2 mg by weight
Gelling agent-hydroxymethyl propyl cellulose (5% w/v)
Preservative-methyl paraben (0.1% w/v), propylparaben (0.01% w/v)
Humectant-glycerine (5% w/v)
Solvent for menthol-ethanol (2 drops)
Sweetening agent-xylitol (1% w/v)
Flavoring agent-menthol (0.05% w/v).
Per gram of lycopene gel contained
Compound-2 mg by weight
Thickening agent-sodium alginate (0.3% w/v), calcium gluconate (0.005% w/v)
Sweetener-Sodium saccharin (0.1% w/v)
Humectant-glycerine (5% w/v)
Flavoring agent-peppermint oil (0.001% w/v).
RESULTS
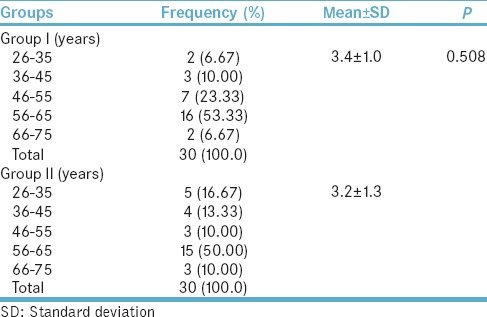
In the present study, the majority of the patients in Group I and Group II were males. There were 28 males and 2 females in Group I and 22 males and 8 females in Group II [Table 1]. The majority of patients in Group I and Group II were in the age group of 56–65 years [Table 2]. No significant difference was present in Group I and Group II in regard to age and gender.
Table 1.
Sex distribution in Group I and Group II
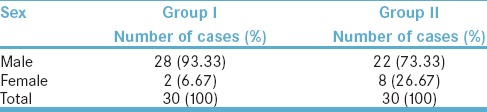
Table 2.
Age distribution in Group I and Group II
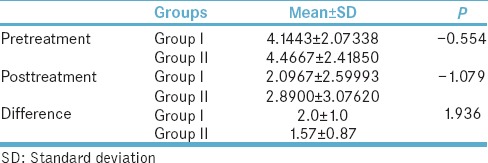
The average size of leukoplakia before treatment was 4.14 cm2 (standard deviation [SD] = 2.07) and after treatment was 2.09 cm2 (SD = 2.59) in Group I [Graph 1]. The average size of leukoplakia before treatment was 4.46 cm2 (SD = 2.41) and after treatment, it was 2.89 cm2 (SD = 3.07) in Group II. The mean difference in the reduction in size before and after treatment for Group I was 2.0 ± 1.0 cm while for the Group II, it was 1.57 ± 0.87 cm [Table 3].
Graph 1.
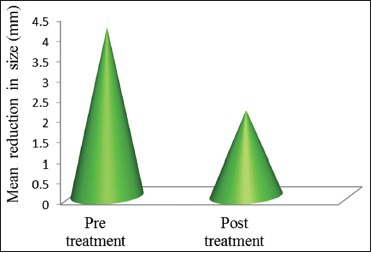
Comparison of change in size after C. officinalis gel application
Table 3.
Comparison of mean±SD of size (cm) of lesion in Group I and II (pre- and post-treatment)
There was statistically significant difference in both Group I and Group II when the pre- and post-treatment results were compared in the same group. However, no significant difference was observed between the two groups.
DISCUSSION
Leukoplakia is one of the most common potentially malignant disorders of the oral mucosa.[1,15] The annual malignant transformation rate of OL ranges between 3% and 17.5%.[15]
Leukoplakia is more common among the elderly men over 40 years of age, and its prevalence increases with age.[16] In the present study, the majority of patients of OL were above 55 years of age, and a higher male predominance was seen. Bánóczy also reported the prevalence of leukoplakia in the age group of 51–60 years with higher male predominance.[17] Espinoza et al. also concluded that there was higher prevalence of leukoplakia in men after 50 years of age.[18] Liu et al. conducted a study on 218 patients of leukoplakia and reported that peak incidence was during the fifth decade of life.[19] Brouns et al. found the mean age of 57 years among 275 patients of leukoplakia.[20] A study done by Gupta et al. also showed the annual incidence of 1.1%–2.4% among men and 0.2%–0.03% among women.[21] Various other investigators like Waldron and Shafer[22] and Mohitpal Singh et al.[8] also reported male predominance for OL.
In the present study, patients in Group II (n = 30) were dispensed lycopene gel. The treatment was instituted for 1 month and followed up for another 3 months. The results of the study showed significant reduction in the size of the lesion with no side effects. Similar results were reported by Mohitpal Singh et al. who compared two different doses of systemic lycopene (8 mg/day and 4 mg/day) with placebo in the treatment of leukoplakia and stated that patients receiving lycopene in both groups showed a significant reduction in size as compared to the placebo group.[8]
The effectiveness of lycopene has also been evaluated in combination with micronutrients, and significant results are reported. Patel et al. found that lycopene in combination with Vitamin E and selenium was effective in reducing the clinical size of the lesion in patients with leukoplakia.[23] Studies carried out by investigators like Nagasawa et al.,[24] Sharoni et al.,[25] Narisawa et al.,[26] and Bhuvaneshwari et al.[27] have suggested lycopene to be an effective agent in inhibiting carcinogenesis.
Several herbal products have been used in the treatment of leukoplakia, and their effectiveness is well documented in the literature. Palak H et al. concluded the role of curcumin in treating precancerous lesions.[28] Deshpande et al. evaluated the effect of Triphala mouth rinse on the reversal of precancerous lesions and reported significant results.[28] Mathew et al. evaluated the effectiveness of Spirulina fusiformis in the chemoprevention of oral cancer. Complete regression of lesions was observed in 16 of 28 (57%) patients supplemented with Spirulina of patients with homogeneous leukoplakia.[29]
Considering the promising effects of herbal medicine in the treatment of leukoplakia, the present study was undertaken to evaluate and compare the effectiveness of C. officinalis extract with lycopene and to propose it as an innocuous, cheap, and easily available treatment modality for the treatment of leukoplakia. There is no evidence in literature about any study done to evaluate the effectiveness of C. officinalis extract in the management of leukoplakia, and hence, this is the first study.
In the present study, all the 30 patients in C. officinalis group demonstrated significant reduction in the size of the lesion in 1 month. The significant differences obtained in Group I indicate that C. officinalis extract can be readily used as an effective treatment modality in the management of leukoplakia. However, no significant differences were seen between the C. officinalis and lycopene group thus indicating that both the drugs are equally effective and can be successfully employed in the treatment of homogeneous leukoplakia. Patients were followed up for a period of 4 months to evaluate the stability in the reduction of size and record any recurrences.
In future, further studies should be carried out by modifying the concentration of C. officinalis gel and following up with histopathological changes.
CONCLUSION
Thus, it can be concluded that C. officinalis extract can be effectively used as an alternative to conventional treatment modality. Looking at the promising results of the study, initiative should be taken in collaboration with herbal healthcare companies to introduce C. officinalis extract at a commercial level so that it is easily available for the patients. Further studies with larger sample size can determine optimal therapeutic dose levels and frequency of administration to improve effectiveness.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to acknowledge Mr. Udayakumar Bolmal Asst. Professor, Department of Pharmaceutics, KLEU college of pharmacy, Belagavi, for providing with the preparation of gel and carrying the study.
REFERENCES
- 1.Brouns E, Baart J, Karagozoglu KH, Aartman I, Bloemena E, van der Waal I. Malignant transformation of oral leukoplakia in a well-defined cohort of 144 patients. Oral Dis. 2014;20:e19–24. doi: 10.1111/odi.12095. [DOI] [PubMed] [Google Scholar]
- 2.Parlatescu I, Gheorghe C, Coculescu E, Tovaru S. Oral leukoplakia – An update. Maedica (Buchar) 2014;9:88–93. [PMC free article] [PubMed] [Google Scholar]
- 3.Reddy KS, Gupta PC. Report on Tobacco Control in India. Joint Report Supported by Ministry of Health and Family Welfare, Government of India, Centre of Disease Control and Prevention. Vol. 2. USA: World Health Organization; 2004. Economic history of tobacco production: From colonial origins to contemporary trends; pp. 19–32. [Google Scholar]
- 4.Radwan-Oczko M, Mendak M. Differential diagnosis of oral leukoplakia and lichen planus – On the basis of literature and own observations. J Stomatol. 2011;64:355–70. [Google Scholar]
- 5.Mortazavi H, Baharvand M, Mehdipour M. Oral potentially malignant disorders: An overview of more than 20 entities. J Dent Res Dent Clin Dent Prospects. 2014;8:6–14. doi: 10.5681/joddd.2014.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Brouns E, Baart JA, Bloemena E, Karagozoglu H, Waal I. The relevance of uniform reporting in oral leukoplakia: Definition, certainty factor and staging based on experience with 275 patients. Med Oral Patol Oral Cir Bucal. 2013;18:e19–26. doi: 10.4317/medoral.18756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Manigandan T, Hemalatha VT. Insight of various medical management of oral leukoplakia. Biomed Pharmacol J. 2015;8:393–401. [Google Scholar]
- 8.Singh M, Krishanappa R, Bagewadi A, Keluskar V. Efficacy of oral lycopene in the treatment of oral leukoplakia. Oral Oncol. 2004;40:591–6. doi: 10.1016/j.oraloncology.2003.12.011. [DOI] [PubMed] [Google Scholar]
- 9.Holzapfel NP, Holzapfel BM, Champ S, Feldthusen J, Clements J, Hutmacher DW. The potential role of lycopene for the prevention and therapy of prostate cancer: From molecular mechanisms to clinical evidence. Int J Mol Sci. 2013;14:14620–46. doi: 10.3390/ijms140714620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.De Stefani E, Oreggia F, Boffetta P, Deneo-Pellegrini H, Ronco A, Mendilaharsu M. Tomatoes, tomato-rich foods, lycopene and cancer of the upper aerodigestive tract: A case-control in Uruguay. Oral Oncol. 2000;36:47–53. doi: 10.1016/s1368-8375(99)00050-0. [DOI] [PubMed] [Google Scholar]
- 11.Rao AV, Agarwal S. Role of antioxidant lycopene in cancer and heart disease. J Am Coll Nutr. 2000;19:563–9. doi: 10.1080/07315724.2000.10718953. [DOI] [PubMed] [Google Scholar]
- 12.Bernatoniene J, Masteikova R, Davalgiene J. Topical application of Calendula officinalis (L.): Formulation and evaluation of hydrophilic cream with antioxidant activity. J Med Plants Res. 2011;5:868–77. [Google Scholar]
- 13.Muley BP, Khadabadi SS, Banarase NB. Phytochemical constituents and pharmacological activities of Calendula officinalis Linn (Asteraceae): A review. Trop J Pharm Res. 2009;8:455–65. [Google Scholar]
- 14.Ozkol H, Tülüce Y, Koyuncu I. Subacute effect of cigarette smoke exposure in rats: Protection by pot marigold (Calendula officinalis L.) extract. Toxicol Ind Health. 2012;28:3–9. doi: 10.1177/0748233711401263. [DOI] [PubMed] [Google Scholar]
- 15.Warnakulasuriya S, Johnson NW, van der Waal I. Nomenclature and classification of potentially malignant disorders of the oral mucosa. J Oral Pathol Med. 2007;36:575–80. doi: 10.1111/j.1600-0714.2007.00582.x. [DOI] [PubMed] [Google Scholar]
- 16.Napier SS, Speight PM. Natural history of potentially malignant oral lesions and conditions: An overview of the literature. J Oral Pathol Med. 2008;37:1–10. doi: 10.1111/j.1600-0714.2007.00579.x. [DOI] [PubMed] [Google Scholar]
- 17.Bánóczy J. Follow-up studies in oral leukoplakia. J Maxillofac Surg. 1977;5:69–75. doi: 10.1016/s0301-0503(77)80079-9. [DOI] [PubMed] [Google Scholar]
- 18.Espinoza I, Rojas R, Aranda W, Gamonal J. Prevalence of oral mucosal lesions in elderly people in Santiago, Chile. J Oral Pathol Med. 2003;32:571–5. doi: 10.1034/j.1600-0714.2003.00031.x. [DOI] [PubMed] [Google Scholar]
- 19.Liu W, Wang YF, Zhou HW, Shi P, Zhou ZT, Tang GY. Malignant transformation of oral leukoplakia: A retrospective cohort study of 218 Chinese patients. BMC Cancer. 2010;10:685. doi: 10.1186/1471-2407-10-685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Brouns ER, Baart JA, Bloemena E, Karagozoglu H, van der Waal I. The relevance of uniform reporting in oral leukoplakia: Definition, certainty factor and staging based on experience with 275 patients. Med Oral Patol Oral Cir Bucal. 2013;18:e19–26. doi: 10.4317/medoral.18756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gupta PC, Mehta FS, Daftary DK, Pindborg JJ, Bhonsle RB, Jalnawalla PN, et al. Incidence rates of oral cancer and natural history of oral precancerous lesions in a 10-year follow-up study of Indian villagers. Community Dent Oral Epidemiol. 1980;8:283–333. doi: 10.1111/j.1600-0528.1980.tb01302.x. [DOI] [PubMed] [Google Scholar]
- 22.Waldron CA, Shafer WG. Current concepts of oral leukoplakia. Int Dent J. 1960;10:352–67. [PubMed] [Google Scholar]
- 23.Patel JS, Umarji HR, Dhokar AA. Randomized controlled trial to evaluate the efficacy of oral lycopene in combination with Vitamin E and selenium in the treatment of oral leukoplakia. J Indian Acad Oral Med Radiol. 2014;26:369–73. [Google Scholar]
- 24.Nagasawa H, Mitamura T, Sakamoto S, Yamamoto K. Effects of lycopene on spontaneous mammary tumour development in SHN virgin mice. Anticancer Res. 1995;15:1173–8. [PubMed] [Google Scholar]
- 25.Sharoni Y, Giron E, Rise M, Levy J. Effects of lycopene-enriched tomato oleoresin on 7,12-dimethyl-benz[a] anthracene-induced rat mammary tumors. Cancer Detect Prev. 1997;21:118–23. [PubMed] [Google Scholar]
- 26.Narisawa T, Fukaura Y, Hasebe M, Nomura S, Oshima S, Sakamoto H, et al. Prevention of N-methylnitrosourea-induced colon carcinogenesis in F344 rats by lycopene and tomato juice rich in lycopene. Jpn J Cancer Res. 1998;89:1003–8. doi: 10.1111/j.1349-7006.1998.tb00488.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bhuvaneswari V, Velmurugan B, Balasenthil S, Ramachandran CR, Nagini S. Chemopreventive efficacy of lycopene on 7,12-dimethylbenz[a] anthracene-induced hamster buccal pouch carcinogenesis. Fitoterapia. 2001;72:865–74. doi: 10.1016/s0367-326x(01)00321-5. [DOI] [PubMed] [Google Scholar]
- 28.Shah PH, Venkatesh R. Curcumin: A magic spice for oral potentially malignant disorders. Int J Phytother. 2015;5:44–7. [Google Scholar]
- 29.Mathew B, Sankaranarayanan R, Nair PP, Varghese C, Somanathan T, Amma BP, et al. Evaluation of chemoprevention of oral cancer with spirulina fusiformis. Nutr Cancer. 1995;24:197–202. doi: 10.1080/01635589509514407. [DOI] [PubMed] [Google Scholar]