

Abstract
Background
Kenyan female sex workers (FSWs) have a high HIV prevalence, increasing their tuberculosis (TB) risk. Despite recommendations that HIV-positive individuals be offered isoniazid preventive therapy (IPT), uptake has been limited.
Methods
In this longitudinal cohort of HIV-positive FSWs, we retrospectively characterized the IPT care cascade between March 2000–January 2010, including reasons for cascade loss or appropriate exit. Cascade success required completion of 6 months of IPT. Baseline characteristics were assessed as potential correlates of cascade losses using multivariable logistic regression.
Results
Among 642 HIV-positive FSWs eligible for IPT evaluation, median age was 31 years (IQR 26–35) with median CD4 lymphocyte count of 409 (IQR 292–604) cells/mm3. There were 249 (39%) women who successfully completed 6 months of IPT, 157 (24%) appropriately exited the cascade, and 236 (37%) were cascade losses. Most cascade losses occurred at symptom screen (38%, 90/236), CXR evaluation (28%, 66/236), or during IPT treatment (30%, 71/236). Twenty-nine women were diagnosed with TB, including one after IPT initiation. Most women initiating IPT completed the course (71%, 249/351); <5% had medication intolerance. Younger women (<25 and 25–35 vs. >35 years; adjusted odds ratio [AOR] 2.65, 95% confidence interval [CI] 1.46–4.80 and AOR 1.78, 95% CI 1.13–2.80, respectively), and those evaluated for IPT after antiretroviral availability in 2004 (AOR 1.92, 95%CI 1.31–2.81), were more likely to be cascade losses.
Conclusions
Implementation of IPT among HIV-positive FSWs in Kenya is feasible. However, significant losses along the IPT care cascade underscore the need for strategies improving retention in care.
Keywords: isoniazid preventive therapy (IPT), tuberculosis, HIV, female sex workers (FSWs), care cascade, latent tuberculosis infection (LTBI)
INTRODUCTION
Tuberculosis (TB) is the leading cause of mortality in people living with HIV (PLHIV).1,2 Among 10.4 million new TB cases in 2015, HIV co-disease was highest in sub-Saharan Africa.2 Key populations including female sex workers (FSWs) have a high HIV prevalence,3 placing them at increased risk for TB.4,5
Isoniazid preventive therapy (IPT) decreases risk of progression from latent TB infection (LTBI) to active TB,6–8 and IPT provision to high-risk groups is a cornerstone of the World Health Organization (WHO) End TB Strategy.9,10 Despite WHO recommendations,7 there has been limited global uptake of this intervention.2 Similar to the HIV care continuum,11 successful IPT implementation requires completion of several steps.12 The optimal approach for IPT delivery is unknown, and few published reports examine this cascade of care in high TB/HIV burden settings,13,14 or within key populations including FSWs.15–18
Kenya is one of the top twenty high TB/HIV burden countries, with TB incidence of 233/100,000,2 and over a third of TB cases occurring in PLHIV.19 In 2014, Kenya guidelines included a strong recommendation for IPT provision to PLHIV.20 However, only 33% of patients newly-enrolled in HIV care initiated IPT in 2015.2
Assessment of the IPT care cascade is useful to inform national roll-outs in Kenya and other high TB/HIV burden countries. Challenges to IPT provision may vary by population. Data from general and key populations is important for program planning and implementation. Our objective was to characterize the cascade of IPT delivery, including reasons for cascade losses, among HIV-positive FSWs enrolled in a research cohort in Mombasa, Kenya, which began providing IPT as part of routine HIV care in 2000.
METHODS
Study Setting and Participants
Mombasa Cohort
We abstracted data from clinical care records from a prospective research cohort of HIV-positive FSWs followed at the Ganjoni Clinic in Mombasa, Kenya (the Mombasa Cohort), between March 2000 – January 2010. The Mombasa Cohort was established in 1993 to investigate HIV incidence and risk factors among FSWs.3 Additional detailed Mombasa Cohort description and procedures have been published.21,22
IPT provision and routine HIV care
In 2000, the program initiated IPT as part of routine HIV care due to growing evidence of IPT benefit for TB prevention in PLHIV.23,24 Routine IPT was not provided in Kenya at the time, and Kenyan guidelines recommended limiting IPT to controlled settings where thorough screening and follow-up for potential side effects could be ensured, without specific recommendations for CXR screening or concomitant ART use.25 The 2000 WHO IPT guidelines did not include recommendations for those with history of TB or during pregnancy.24 Therefore the program did not provide IPT to women with a history of TB, current pregnancy, or irregular clinic attendance, and included CXR as part of the screening process for IPT. In 2004, the site became one of the first in Kenya to provide antiretroviral therapy (ART) to participants with CD4 lymphocyte counts <200 cells/μl or AIDS-defining illness, following WHO and Kenya guidelines.22 ART initiation (in eligible women) was then prioritized over IPT due to concerns about pill burden and potential toxicity leading to possible poor adherence in during the initial rollout of ART. In 2005, Kenyan ART guidelines were modified to include individuals with Stage III disease and CD4 lymphocyte counts <350 cells/μl, which was incorporated into cohort procedures.21
Procedures
IPT program procedures and cascade of care
For women eligible for IPT screening, the care cascade comprised of several steps (Figure 1). First, women underwent TB symptom screening (presence of cough >2 weeks, fever >2 weeks, unintentional weight loss >2kg, night sweats, shortness of breath, or pleuritic chest pain). Women with positive symptom screens were referred to the Ministry of Health TB clinic within the facility for further work-up (Supplemental Figure 1). Patients were screened for TB symptoms at follow-up visits, however data regarding subsequent symptom screening was not routinely recorded for the purpose of this study.
Figure 1. Major steps in the IPT care cascade.
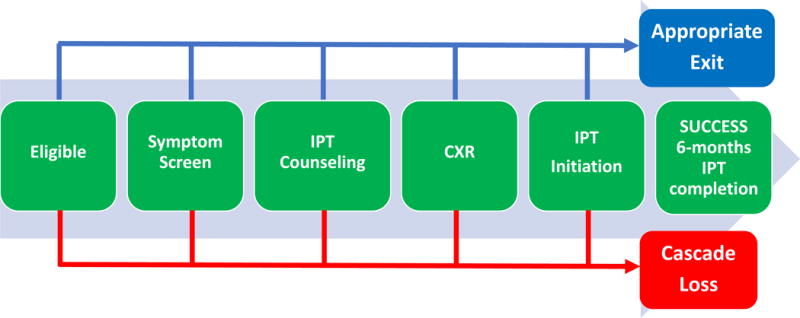
At each step in the cascade, women may either exit due to cascade failure (primarily due to lost to follow-up) (red), appropriately exit (blue), or successfully continue on to the next step (green). Success requires completion of 6 months of IPT.
TB diagnosis included sputum smear evaluation and a clinical algorithm for identifying patients with smear-negative TB based on continued symptoms, CXR abnormality, and lack of response to antibiotics for typical causes of pneumonia.25 Women with initially positive symptom screens could continue IPT cascade procedures once TB work-up was negative. Those with negative symptom screens (or negative TB work-up for initially positive screens) were referred for counseling regarding IPT to reduce risk of active TB, cough hygiene/ventilation to prevent TB exposure, adherence counseling, potential side effects, and refill procedures. After counseling, women were referred for CXR. Those with abnormal CXR were referred to the Ministry of Health TB clinic for further evaluation.
Women with negative symptom screen and CXR (or negative TB work-up) were offered a 6-month course of IPT.24 Initial medication supply was dispensed by nurses. Isoniazid was co-administered with pyridoxine to reduce neuropathy risk. Refills were provided at one to three month intervals, during scheduled HIV care visits. Tuberculosis screening (including CXR), IPT, and pyridoxine were provided at no cost, and women received reimbursement for transport (approximately 100–200 Kenyan shillings) for study visits. Testing for LTBI (tuberculin skin test or interferon gamma-release assay) was not performed based on WHO and Kenyan guidelines.25
At each step, women could appropriately exit, successfully proceed to the next step, or be considered cascade losses. Cascade success required completion of 6 months of IPT within a 9-month period.
Clinic-level interventions to improve IPT delivery and documentation
Beginning in March 2000, initiation and completion of IPT was documented in clinical notes within participants’ research files and an IPT register. In July 2000, an “IPT stamp” was created to mark the front cover of participants’ files to record IPT initiation and completion dates. In December 2004, an IPT/TB screening form was added to support efficient and consistent TB symptom screening prior to IPT initiation.
Data collection procedures
Retrospective chart review was performed by study staff using a standardized data collection form. Baseline characteristics, progress through IPT cascade, and reasons for appropriate cascade exit or losses were noted.
Study Endpoints
For the primary analysis, women were categorized as 1) successfully completed, 2) appropriately exited, or as 3) cascade losses (Figure 1). Women were considered to have appropriately exited the cascade if they became pregnant, were diagnosed with active TB prior to initiating and/or during IPT, were ART eligible (once available at the site), had irregular clinic attendance that would likely compromise close follow-up, or IPT discontinuation due to medication intolerance. Cascade losses included all losses along the cascade that did not fit appropriate exit criteria, including loss to follow-up, or unknown/missing reason for exit. The proportion of women who successfully completed, appropriately exited, or were considered cascade losses were calculated for each step, and cumulatively. Correlates of cascade losses were identified by comparing baseline characteristics of FSWs with cascade success vs. cascade losses.
Statistical Analysis
Categorical baseline characteristics were summarized by frequency and proportion, and by median and interquartile range (IQR) for continuous variables. Bivariable logistic regression was used to assess associations between potential correlates and the outcome of cascade loss using unadjusted odds ratios (ORs). Adjusted odds ratios (AORs) were calculated using multivariable logistic regression models adjusted for variables associated with cascade losses in unadjusted analyses (p ≤ 0.10). Odds ratio estimates were reported with 95% confidence intervals (CI). STATA version 12.0 (StataCorp, College Station, TX, USA) was used for all statistical analysis.
Sensitivity Analyses
Because WHO and Kenyan IPT eligibility criteria during the study period differ from current guidelines, we performed additional analyses to assess whether our primary results were sensitive to differences in appropriate cascade exit definitions. After reclassifying individuals not offered IPT due to irregular clinic attendance, participant refusal, ART eligibility, or pregnancy as cascade losses, we repeated analyses calculating overall cascade losses and appropriate exits and correlates of cascade loss.
Ethics Approval
This study was approved by the Kenyatta National Hospital-University of Nairobi Ethics and Research Committee, the University of Washington Human Subjects Research Committee, and the Fred Hutchinson Cancer Research Center’s Institutional Review Board.
Results
Between March 2000 and January 2010, 846 HIV-positive FSWs were seen for at least one Mombasa Cohort study visit. Of these, 204 (24%) were considered ineligible for IPT evaluation. Ineligible women included 106 (13%) with history of active TB, 80 (39%) lost to follow-up before staff could initiate IPT evaluation (typically, immediately following Mombasa Cohort enrollment), and 18 (4%) who were ART-eligible at enrollment (Supplemental Figure 1). The remaining 642 women were considered eligible for IPT evaluation and are the basis for the remainder of analyses (Figure 2). Baseline median age was 31 years (IQR 26–35) with median CD4 lymphocyte count of 409 (IQR 292–604) cells/μL (Table 1). The majority of women were widowed or divorced (421, 66%). Sixty-three (10%) smoked tobacco, 519 (81%) reported alcohol use, and 77 (12%) reported drug use (marijuana, khat, or both). One woman reported injection drug use.
Figure 2. Cascade of IPT implementation among HIV-positive female sex workers including reasons for cascade losses and appropriate cascade exit.
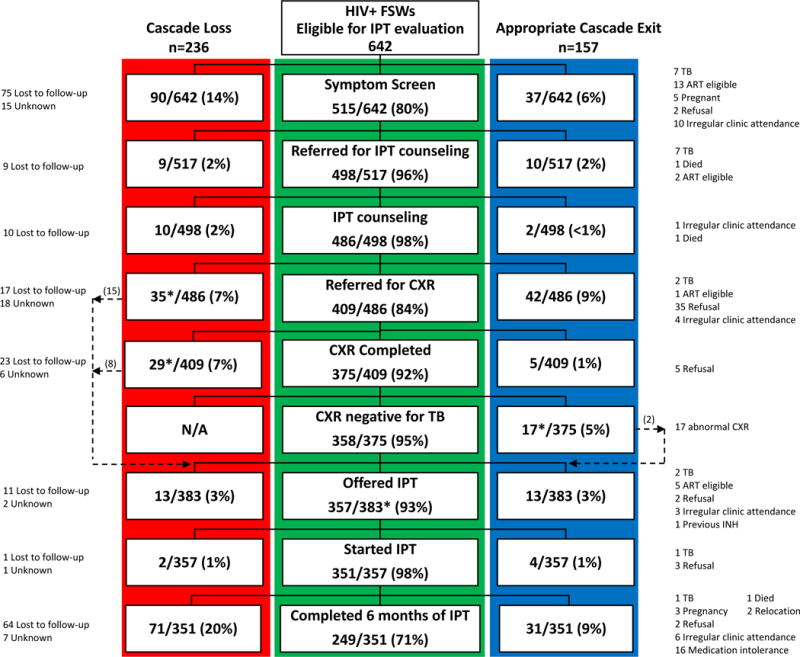
At each step in the cascade, women may exit due to cascade loss (red), appropriately exit (blue), or successfully continue to the next step (green). Proportions indicate the number of women evaluable at each cascade step. In total, 249 completed a 6-month course of IPT, 236 were considered cascade losses, and 157 appropriately exited the cascade.
*25 women exited then re-entered the cascade to be offered IPT (15 not referred for CXR for unknown reason, 8 CXR not completed for unknown reason, and 2 with abnormal CXR, but not consistent with TB who were then referred for IPT).
Table 1.
Baseline characteristics of HIV-positive female sex workers eligible for IPT evaluation, Mombasa, Kenya, 2000–2010
| Eligible N= 642 |
||
|---|---|---|
| N or median | (% or IQR) | |
| Age (years) | 31 | (26–35) |
| Education (years) | 8 | (7–10) |
| Marital status | ||
| Never married | 214 | (33) |
| Currently married | 7 | (1) |
| Widowed/divorced | 421 | (66) |
| Workplace | ||
| Bar/restaurant/guesthouse | 521 | (81) |
| Nightclub | 46 | (7) |
| Home-based/other | 75 | (12) |
| Smoker | 63 | (10) |
| Alcohol use | 519 | (81) |
| Drug use | 77 | (12) |
| Years as sex worker* | 2 | (0–5) |
| CD4 (cells/mm3) (n=640) | ||
| < 200 | 66 | (10) |
| 200–350 | 169 | (26) |
| >350 | 405 | (63) |
| Median CD4 (cells/mm3) | 409 | (292–604) |
| Year eligible for IPT evaluation | ||
| 2000–2003 | 376 | (59) |
| 2004–2010** | 266 | (41) |
Women engaged in sex work <6 months are coded as “0 years”
In 2004 ART became available at the site. Starting in 2004 ART-eligible women were preferentially offered ART prior to IPT.
IPT care cascade
Of 642 women eligible for IPT evaluation, 517 (80%) completed TB symptom screening, 486 (76%) completed IPT counseling, 375 (58%) completed CXR, and 351 (55%) initiated IPT (Figure 3). Of 351 women who initiated IPT, 249 (71%) completed a 6-month course, 71 (20%) were lost to follow-up or left the cascade for unknown reasons, and 31 (9%) appropriately discontinued IPT. Figure 2 details the stepwise attrition of participants, including proportion of women evaluable at each step, and reasons for cascade losses or appropriate exit. Sixteen (5%) women discontinued IPT due to medication intolerance, and one developed TB while on IPT (0.003%) (Supplemental Table 1).
Figure 3. Cumulative proportion of cascade losses, appropriate cascade exit, and successful completion of IPT among HIV-positive female sex workers.

The greatest cascade losses prior to IPT initiation occurred at initial symptom screen and CXR.
Overall, of the 642 women who entered the IPT care cascade, 249 (39%) successfully completed a 6-month course of IPT, 236 (37%) were considered cascade losses, and 157 (24%) exited the cascade appropriately (Figure 3). The greatest cascade drop-offs occurred at initial symptom screen, where 90 (14%) participants were reported as cascade losses, and at CXR completion, where an additional 64 (10%) participants from the previous step failed to progress. Among 157 women with appropriate cascade exit, the most common reasons included participant refusal of IPT (49, 31%) or identification of active TB prior to IPT initiation (34, 22%) (Supplemental Table 1). For 236 women considered as cascade losses, the majority were lost to follow-up (208, 88%), while the remaining (28, 12%) exited the cascade for unknown/missing reasons.
We compared baseline characteristics of women identified as cascade losses to those with successful cascade completion. There was a progressive stepwise increased risk of cascade loss with younger age compared to women >35 years (25–35 years: OR 1.65 [95% CI 1.06–2.56], p = 0.03; <25 years: OR 2.39 [95% CI 1.34–4.26], p = 0.003) (Table 2). Women eligible for IPT evaluation from 2004 onwards (when ART became available) were more likely to have cascade loss (OR 1.78 [95% CI 1.23–2.56], p=0.002). Among women with CD4 lymphocyte counts ≥200 cells/mm3, there was also a trend for cascade loss (OR 1.85 [95% CI 0.96–3.55], p = 0.07). In multivariate analysis, after adjusting for age, CD4 lymphocyte count, and year of IPT eligible evaluation, younger women and participants eligible for IPT evaluation after 2004 remained at significantly higher risk of cascade loss. Results were similar and remained statistically significant when repeating the analysis with year of IPT eligible evaluation treated as a continuous variable (data not shown).
Table 2.
Comparison of characteristics of HIV-positive female sex workers considered cascade losses vs. those with successful IPT completion and correlates of cascade losses
|
Cascade Losses N= 236 |
Cascade Success* N= 249 |
Unadjusted Odds Ratio (OR) |
Adjusted Odds Ratio (AOR) |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | OR | 95% CI | p | AOR** | 95% CI | p | |
| Age (years) | ||||||||||
| <25 | 48 | 59.3 | 33 | 40.7 | 2.39 | 1.34–4.26 | 0.003 | 2.65 | 1.46–4.80 | 0.001 |
| 25–35 | 143 | 50.1 | 142 | 49.3 | 1.65 | 1.06–2.56 | 0.03 | 1.78 | 1.13–2.80 | 0.01 |
| >35 | 45 | 37.8 | 74 | 60.7 | ref | ref | ||||
| Education | ||||||||||
| Completed primary school | 137 | 51.3 | 130 | 48.0 | 1.27 | 0.88–1.81 | 0.18 | – | ||
| Marital status | ||||||||||
| Ever married | 152 | 57.5 | 169 | 51.5 | 0.86 | 0.58–1.25 | 0.42 | – | ||
| Workplace | ||||||||||
| Bar/restaurant/guesthouse | 197 | 50.1 | 196 | 49.1 | ref | – | ||||
| Nightclub | 16 | 44.4 | 20 | 55.6 | 0.80 | 0.40–1.58 | 0.52 | |||
| Home-based/other | 23 | 41.1 | 33 | 58.9 | 0.69 | 0.39–1.22 | 0.21 | |||
| Current smoker | 23 | 46.8 | 25 | 52.1 | 0.92 | 0.50–1.68 | 0.79 | – | ||
| Current ETOH | 196 | 49.6 | 199 | 50.0 | 1.23 | 0.78–1.95 | 0.38 | – | ||
| Current drug use | 33 | 57.9 | 24 | 41.4 | 1.52 | 0.87–2.66 | 0.14 | – | ||
| CD4 (cells/mm3) | ||||||||||
| CD4 < 200 | 15 | 34.9 | 28 | 65.1 | ref | ref | ||||
| CD4 ≥ 200 | 219 | 48.8 | 221 | 49.6 | 1.85 | 0.96–3.55 | 0.07 | 1.59 | 0.81–3.11 | 0.17 |
| Year eligible for IPT evaluation | ||||||||||
| 2000–2003 | 125 | 43.0 | 166 | 57.0 | ref | ref | ||||
| 2004–2010*** | 111 | 57.2 | 83 | 41.5 | 1.78 | 1.23–2.56 | 0.002 | 1.92 | 1.31–2.81 | 0.001 |
Completion of a 6-months course of IPT
Adjusted for age, CD4 lymphocyte count, year eligible for IPT evaluation
In 2004 ART became available at the site. Starting in 2004 ART-eligible women were preferentially offered ART prior to IPT.
In our sensitivity analyses, women who were initially considered to have appropriately exited due to irregular clinic attendance, refusal to continue in the cascade, or not offered IPT due to ART eligibility or pregnancy, were reclassified as cascade losses.12 This increased cascade losses from 236 (37%) to 336 (52%), while reducing appropriate cascade exits from 157 (24%) to 57 (9%). However, the correlates of cascade loss based on these revised definitions resulted in similar or stronger statistically significant associations with younger age and year eligible for IPT evaluation after 2004 (when ART became available (data not shown).
Discussion
To our knowledge, this is the first study to address the IPT care cascade in HIV-positive African FSWs. Overall, 39% successfully completed IPT, 24% appropriately exited the cascade, and 37% were considered cascade losses. Among those initiating IPT, 6-month completion rates were 71%. The burden of TB was high, with six percent of women diagnosed with active TB prior to IPT initiation. Only one woman developed TB after starting IPT. Younger age and undergoing IPT evaluation after availability of ART were associated with greater risk of cascade loss.
Program-based exclusion criteria and CXR screening of women without TB symptoms likely contributed to cascade losses. Program decisions regarding exclusion criteria were based on country-specific guidelines at the time, as well as the lack of data regarding IPT safety, efficacy, and feasibility during pregnancy, in patients with previous TB, and in patients concurrently initiating and continuing ART. Provision of IPT began in this program in 2000, ten years before release of the 2010 WHO guidelines for intensified TB case-finding and IPT for PLHIV in resource-constrained settings.7 Prior to 2011, routine IPT for PLHIV in Kenya was recommended only in controlled settings like the research clinic supporting the Mombasa Cohort.25 In 2011, Kenyan HIV care guidelines recommended IPT for PLHIV (including pregnant women and those on ART) in whom active TB had been excluded.26 The 2014 Kenyan HIV care guidelines have since expanded eligibility to include those with previous TB, with IPT initiation recommended at any time after successful TB treatment completion.20 Current WHO guidelines do not require or recommend CXR as part of the routine assessment for IPT eligibility. Elimination of CXR requirement and more inclusive eligibility criteria (including during pregnancy and concurrent ART) would likely increase the number of women receiving IPT. Other barriers, such as individual preference for not initiating IPT and loss to follow-up, are likely to remain relevant under more inclusive contemporary guidelines. In our study, IPT cascade failure was associated with younger age as well as IPT evaluation eligibility after the availability of ART. Younger age has been associated with lower rates of retention in the HIV care cascade,27–30 and factors impacting HIV care cascade retention likely play a role in TB screening and prevention care cascades. Younger PLHIV may be less likely to perceive their risk for TB and be less willing to take a medication for prevention (like IPT) as opposed to treatment a symptomatic illness. Interventions targeting those at highest risk of loss to follow-up prior to IPT initiation may strengthen IPT programs. The high proportion of participant refusal of IPT represents an opportunity for improved education and counseling regarding the benefits of IPT to prevent active TB, and remains an important contributor to cascade failure currently. Healthcare provider promotion of IPT and close follow-up to ensure completion of cascade steps, as well as patient acceptance of IPT, may be higher now that this intervention has been more widely promoted and implemented. LTBI status assessment was not performed (i.e. TST or interferon gamma-release assay), however current WHO and Kenyan guidelines recommend IPT be offered to all PLHIV even when TST is not feasible in programmatic settings.7,25 Notably, in the context of the IPT cascade, adding a step could potentially create an additional bottleneck, decreasing the proportion of women successfully completing treatment and will be an important area for future implementation research. To increase comparability of our findings to conditions found under contemporary IPT guidelines, we performed sensitivity analyses reclassifying women who were considered to have appropriately exited the cascade during the time under evaluation, as cascade losses under current recommendations. Although cascade losses increased, correlates of cascade losses remained similar.
Strengths of this study include a focus on a key population for which IPT implementation data is lacking, large sample size and longitudinal follow-up, and detailed assessment of reasons for cascade losses at each step. Although FSWs are considered a key population with regards to HIV, there are few studies evaluating IPT provision in this population at risk for TB.15–18 The Global Plan to End TB 2016–2020 has called for a similar 90-90-90 approach inspired by UNAIDS goals for HIV testing, treatment, and viral suppression coverage.31 The plan includes preventive treatment for persons at high risk for TB (including PLHIV), focuses on key populations with increased exposure to TB (including sex workers), and highlights the importance of operational research.31 Available data regarding FSW and the HIV care continuum primarily from research settings, suggest that once engaged in HIV care, FSWs can achieve high levels of ART uptake, retention, adherence, and HIV viral suppression.32 The long period of cohort follow-up (10 years), with accrual of over 650 participants eligible to enter the IPT care cascade provided power to detect significant differences in baseline characteristics associated with cascade failure. Detailed assessment of clinical records allowed us to determine individual-level outcomes, including reasons for cascade losses at each step. Prior studies of IPT implementation have primarily focused on completion of IPT among those who initiate therapy, rather than all potentially eligible patients.33,34 By evaluating the entire IPT care cascade, we demonstrated that the majority of cascade losses occur prior to IPT initiation.
A major strength of the IPT program was the identification of 41/646 (6%) women with active TB prior to IPT initiation, allowing for appropriate referral to TB care and implementation of measures to reduce transmission risk to staff and other clinic attendees. Notably, 71% of FSWs who initiated IPT in our clinic completed their 6-month course. This is considerably higher than the estimate of 52% in other low- or middle-income settings reported in a recent systematic review.12 Importantly, there were very few discontinuations due to medication intolerance (<5%), or development of active TB (1 case) while on IPT. Our study adds to the growing body of literature that although provider concerns regarding potential medication intolerance and development of isoniazid-resistant TB on IPT are noted barriers to IPT implementation,12 they remain relatively rare events.
This study had limitations. Data were collected through a retrospective review of clinical data recorded in research participant files within the Mombasa Cohort established to explore the incidence, correlates, prevention, and treatment of HIV and STIs in FSWs, and not originally designed to study IPT implementation. However, IPT provision was added in 2000 as a non-research component of HIV care, and this analysis of IPT implementation may be generalizable to routine HIV care settings. Nonetheless, we recognize that the research clinic is likely to have more staff per participant than a typical HIV care setting. Most women were characterized as lost to follow-up if it was clear they did not continue in the cascade, or unknown if no reason was recorded. As such, it is difficult to discern participant- versus clinic-level reasons for cascade losses. Our analysis of reasons for cascade losses was limited to quantitative evaluation of baseline participant characteristics. Systematic reviews of both quantitative and qualitative data have identified individual-level characteristics and beliefs, as well as interpersonal and structural factors, associated with IPT adherence.12,35 In addition, systematic reviews specific to FSW populations have identified substance use, food insecurity, and treatment knowledge and attitudes as factors that influence linkage and retention in HIV care,36 and likely impact IPT uptake as well. Although adherence counseling was performed at follow-up visits, direct measures of adherence were not performed. Details regarding TB diagnosis were not available, and given limited rapid TB diagnostics at the time, there may have been either over- or under-ascertainment of TB cases.
In conclusion, this analysis demonstrated IPT implementation in a population of HIV-positive FSWs in a high TB burden setting was feasible. However, significant losses along the IPT care cascade prior to IPT initiation underscore the need to identify solutions to improve the efficiency of the screening process. Reducing pre-IPT initiation losses earlier in the cascade could provide greater public health benefit.12 Although ART significantly reduces the risk of TB in PLHIV,37 the risk of active TB remains considerably higher in PLHIV compared to HIV-uninfected individuals even after early ART initiation and immune reconstitution.38,39 Universal ART modeling data suggest ART alone will be insufficient to prevent future HIV-associated TB. Recent data demonstrate the ART and IPT have additive TB prevention and mortality benefits, compared to either strategy alone.40–42 Further research is needed regarding long-term follow-up of PLHIV, including key populations, on concurrent ART and IPT under programmatic conditions. Successful TB prevention efforts for PLHIV, including FSWs, will require integration into the HIV care continuum to prevent cascade losses and ensure successful IPT implementation.
Supplementary Material
Acknowledgments
We thank the study staff at the Women’s Health Project and study participants.
RSM and SML designed the study and analyses. RSM, RWD, SMG, LNM, WJ, and KNM conducted the field work for the study. SML conducted statistical analyses. RSM and JO secured funding for the Mombasa Cohort. All co-authors contributed to manuscript writing and approved the final draft for publication.
SOURCE OF FUNDING: The Mombasa Cohort was supported by NIH R01 AI38518 to JO. SML was supported by NIH T32 AI07140, K23 AI 120793-01 and the Firland Foundation. Logistical and infrastructure support for the Mombasa Field Site was provided by the University of Washington and Fred Hutchinson Cancer Research Center’s Center for AIDS Research NIH P30 AI027757.
Footnotes
PRIOR REPORTS: Preliminary study results were presented at the International Union Against Tuberculosis and Lung Disease World Conference (Barcelona, Spain), November 2014.
CONFLICTS OF INTEREST: RSM receives research funding (paid to the University of Washington) from Hologic Corporation.
References
- 1.UNAIDS. Global HIV Statistics Fact Sheet 2016. 2016 http://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf. Accessed 15 February, 2017.
- 2.World Health Organization. Global Tuberculosis Report 2016. 2016 http://www.who.int/tb/publications/global_report/en/. Accessed February 15, 2017.
- 3.Martin HL, Jr, Nyange PM, Richardson BA, et al. Hormonal contraception, sexually transmitted diseases, and risk of heterosexual transmission of human immunodeficiency virus type 1. J Infect Dis. 1998;178(4):1053–1059. doi: 10.1086/515654. [DOI] [PubMed] [Google Scholar]
- 4.Gilks CF, Godfrey-Faussett P, Batchelor BI, et al. Recent transmission of tuberculosis in a cohort of HIV-1-infected female sex workers in Nairobi, Kenya. AIDS. 1997;11(7):911–918. doi: 10.1097/00002030-199707000-00011. [DOI] [PubMed] [Google Scholar]
- 5.World Health Organization. Consolidated guidelines on HIV prevention, diagnosis, treatment and care for key populations. 2014 http://www.who.int/hiv/pub/guidelines/keypopulations/en/. Accessed Februrary 15, 2017. [PubMed]
- 6.Akolo C, Adetifa I, Shepperd S, Volmink J. Treatment of latent tuberculosis infection in HIV infected persons. The Cochrane database of systematic reviews. 2010;(1):CD000171. doi: 10.1002/14651858.CD000171.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.World Health Organization. Guidelines for intensified tuberculosis case-finding and isoniazid preventive therapy for people living with HIV in resource-constrained settings. 2011 http://whqlibdoc.who.int/publications/2011/9789241500708_eng.pdf. Accessed February 1, 2017.
- 8.Briggs MA, Emerson C, Modi S, Taylor NK, Date A. Use of isoniazid preventive therapy for tuberculosis prophylaxis among people living with HIV/AIDS: a review of the literature. J Acquir Immune Defic Syndr. 2015;68(Suppl 3):S297–305. doi: 10.1097/QAI.0000000000000497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Uplekar M, Weil D, Lonnroth K, et al. WHO’s new end TB strategy. Lancet. 2015;385(9979):1799–1801. doi: 10.1016/S0140-6736(15)60570-0. [DOI] [PubMed] [Google Scholar]
- 10.World Health Organization. Guidelines on the management of latent tuberculosis infection. 2015 http://www.who.int/tb/publications/latent-tuberculosis-infection/en/. Accessed February 1, 2017. [PubMed]
- 11.Kay ES, Batey DS, Mugavero MJ. The HIV treatment cascade and care continuum: updates, goals, and recommendations for the future. AIDS Res Ther. 2016;13:35. doi: 10.1186/s12981-016-0120-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Alsdurf H, Hill PC, Matteelli A, Getahun H, Menzies D. The cascade of care in diagnosis and treatment of latent tuberculosis infection: a systematic review and meta-analysis. Lancet Infect Dis. 2016;16(11):1269–1278. doi: 10.1016/S1473-3099(16)30216-X. [DOI] [PubMed] [Google Scholar]
- 13.Adams LV, Talbot EA, Odato K, Blunt H, Steingart KR. Interventions to improve delivery of isoniazid preventive therapy: an overview of systematic reviews. BMC Infect Dis. 2014;14:281. doi: 10.1186/1471-2334-14-281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cobelens F, van Kampen S, Ochodo E, Atun R, Lienhardt C. Research on implementation of interventions in tuberculosis control in low- and middle-income countries: a systematic review. PLoS Med. 2012;9(12):e1001358. doi: 10.1371/journal.pmed.1001358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Daly R, Khatib N, Larkins A, Dedicoat M. Testing for latent tuberculosis infection using interferon gamma release assays in commercial sex workers at an outreach clinic in Birmingham. Int J STD AIDS. 2016;27(8):676–679. doi: 10.1177/0956462415619261. [DOI] [PubMed] [Google Scholar]
- 16.Chiang SS, Paulus JK, Huang CC, et al. Tuberculosis screening among Bolivian sex workers and their children. Journal of epidemiology and global health. 2015;5(2):205–210. doi: 10.1016/j.jegh.2014.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Velasquez MG, Laniado-Laborin R, Rodwell TC, et al. Tuberculosis testing among populations with high HIV risk in Tijuana, Baja California, Mexico. Rev Panam Salud Publica. 2012;32(1):30–35. doi: 10.1590/s1020-49892012000700005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ngamvithayapong J, Uthaivoravit W, Yanai H, Akarasewi P, Sawanpanyalert P. Adherence to tuberculosis preventive therapy among HIV-infected persons in Chiang Rai, Thailand. AIDS. 1997;11(1):107–112. doi: 10.1097/00002030-199701000-00016. [DOI] [PubMed] [Google Scholar]
- 19.Kenya Ministry of Health National Tuberculosis; Leprosy and Lung Disease Unit (NTLD) Kenya NTLD Unit Annual Report 2014. 2014 http://nltp.co.ke/annual-reports/. Accessed February 15, 2017.
- 20.Kenyan Ministry of Health, National AIDS and STI Control Program (NASCOP) Guidelines on use of antiretroviral drugs for treating and preventing HIV infection: a rapid advice. 2014 http://healthservices.uonbi.ac.ke/sites/default/files/centraladmin/healthservices/Rapid%20Advice%20Booklet%202014%2024%20June%2012%20noon_0.pdf.
- 21.McClelland RS, Richardson BA, Cherutich P, et al. A 15-year study of the impact of community antiretroviral therapy coverage on HIV incidence in Kenyan female sex workers. AIDS. 2015;29(17):2279–2286. doi: 10.1097/QAD.0000000000000829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.McClelland RS, Graham SM, Richardson BA, et al. Treatment with antiretroviral therapy is not associated with increased sexual risk behavior in Kenyan female sex workers. AIDS. 2010;24(6):891–897. doi: 10.1097/QAD.0b013e32833616c7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bucher HC, Griffith LE, Guyatt GH, et al. Isoniazid prophylaxis for tuberculosis in HIV infection: a meta-analysis of randomized controlled trials. AIDS. 1999;13(4):501–507. doi: 10.1097/00002030-199903110-00009. [DOI] [PubMed] [Google Scholar]
- 24.World Health Organization and UNAIDS. Policy statement on preventive therapy against tuberculosis in people living with HIV. 1998 http://apps.who.int/iris/bitstream/10665/64509/1/WHO_TB_98.255.pdf.
- 25.Kenyan Ministry of Health DoL, Tuberculosis and Lung Disease (DLTLD) DLTLD Guidelines on management of Leprosy and Tuberculosis. 2009 http://www.who.int/hiv/pub/guidelines/kenya_tb.pdf. Accessed February 1, 2017.
- 26.Kenya National AIDS/STI Control Program (NASCOP) [Accessed February 15, 2017];Guidelines for antiretroviral therapy in Kenya. 2011 Available at: http://healthservices.uonbi.ac.ke/sites/default/files/centraladmin/healthservices/Kenya%20Treatment%20Guidelines%202011.pdf.
- 27.Horberg MA, Hurley LB, Klein DB, et al. The HIV Care Cascade Measured Over Time and by Age, Sex, and Race in a Large National Integrated Care System. AIDS Patient Care STDS. 2015;29(11):582–590. doi: 10.1089/apc.2015.0139. [DOI] [PubMed] [Google Scholar]
- 28.Shaw S, Amico KR. Antiretroviral Therapy Adherence Enhancing Interventions for Adolescents and Young Adults 13–24 Years of Age: A Review of the Evidence Base. J Acquir Immune Defic Syndr. 2016;72(4):387–399. doi: 10.1097/QAI.0000000000000977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kim SH, Gerver SM, Fidler S, Ward H. Adherence to antiretroviral therapy in adolescents living with HIV: systematic review and meta-analysis. AIDS. 2014;28(13):1945–1956. doi: 10.1097/QAD.0000000000000316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lall P, Lim SH, Khairuddin N, Kamarulzaman A. Review: an urgent need for research on factors impacting adherence to and retention in care among HIV-positive youth and adolescents from key populations. J Int AIDS Soc. 2015;18(2 Suppl 1):19393. doi: 10.7448/IAS.18.2.19393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.The Paradigm Shift 2016–2020 Global Plan to End TB. 2015 http://www.stoptb.org/assets/documents/global/plan/GlobalPlanToEndTB_TheParadigmShift_2016-2020_StopTBPartnership.pdf. Accessed February 1, 2017.
- 32.Mountain E, Mishra S, Vickerman P, Pickles M, Gilks C, Boily MC. Antiretroviral therapy uptake, attrition, adherence and outcomes among HIV-infected female sex workers: a systematic review and meta-analysis. PLoS One. 2014;9(9):e105645. doi: 10.1371/journal.pone.0105645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hirsch-Moverman Y, Daftary A, Franks J, Colson PW. Adherence to treatment for latent tuberculosis infection: systematic review of studies in the US and Canada. Int J Tuberc Lung Dis. 2008;12(11):1235–1254. [PubMed] [Google Scholar]
- 34.Fox GJ, Barry SE, Britton WJ, Marks GB. Contact investigation for tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2013;41(1):140–156. doi: 10.1183/09031936.00070812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Makanjuola T, Taddese HB, Booth A. Factors associated with adherence to treatment with isoniazid for the prevention of tuberculosis amongst people living with HIV/AIDS: a systematic review of qualitative data. PLoS One. 2014;9(2):e87166. doi: 10.1371/journal.pone.0087166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lancaster KE, Cernigliaro D, Zulliger R, Fleming PF. HIV care and treatment experiences among female sex workers living with HIV in sub-Saharan Africa: A systematic review. Afr J AIDS Res. 2016;15:377–386. doi: 10.2989/16085906.2016.1255652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Lawn SD, Wood R, De Cock KM, Kranzer K, Lewis JJ, Churchyard GJ. Antiretrovirals and isoniazid preventive therapy in the prevention of HIV-associated tuberculosis in settings with limited health-care resources. Lancet Infect Dis. 2010;10(7):489–498. doi: 10.1016/S1473-3099(10)70078-5. [DOI] [PubMed] [Google Scholar]
- 38.Gupta A, Wood R, Kaplan R, Bekker LG, Lawn SD. Tuberculosis incidence rates during 8 years of follow-up of an antiretroviral treatment cohort in South Africa: comparison with rates in the community. PLoS One. 2012;7(3):e34156. doi: 10.1371/journal.pone.0034156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kufa T, Mabuto T, Muchiri E, et al. Incidence of HIV-associated tuberculosis among individuals taking combination antiretroviral therapy: a systematic review and meta-analysis. PLoS One. 2014;9(11):e111209. doi: 10.1371/journal.pone.0111209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Rangaka MX, Wilkinson RJ, Boulle A, et al. Isoniazid plus antiretroviral therapy to prevent tuberculosis: a randomised double-blind, placebo-controlled trial. Lancet. 2014;384(9944):682–690. doi: 10.1016/S0140-6736(14)60162-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Temprano ANRS Study Group. A Trial of Early Antiretrovirals and Isoniazid Preventive Therapy in Africa. N Engl J Med. 2015;373(9):808–822. doi: 10.1056/NEJMoa1507198. [DOI] [PubMed] [Google Scholar]
- 42.Badje A, Moh R, Gabillard D, et al. Six-Month IPT Reduces Mortality Independent of ART in African Adults with High CD4. Paper presented at: Conference on Retroviruses and Opportunistic Infections; February 13–16, 2017; Seattle, WA. 2017. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.