

Abstract
Hispanics represent a critical target for culturally-adapted diet interventions. In this formative research, we translated HealthyYouTXT, an mHealth program developed by the U.S. National Cancer Institute, into HealthyYouTXT en Español, a linguistically and culturally appropriate version for Spanish speakers. We report a three-stage, mixed-methods process through which we culturally adapted the text messages, evaluated their acceptability, and revised the program based on the findings. In Stage 1, we conducted initial translations and adaptations of the text libraries using an iterative, principle-guided process. In Stage 2, we used mixed methods including focus groups and surveys with 109 Hispanic adults to evaluate the acceptability and cultural appropriateness of the program. Further, we used survey data to evaluate whether Self-Determination Theory factors (used to develop HealthyYouTXT) of autonomous motivation, controlled motivation, and amotivation and Hispanic cultural beliefs about familism, fatalism, and destiny predict program interest and its perceived efficacy. Mixed-methods analyses revealed substantial interest in HealthyYouTXT, with most participants expressing substantial interest in using it and viewing it as highly efficacious. Both cultural beliefs (i.e., beliefs in destiny and, for men, high familism) and SDT motivations (i.e., autonomy) predicted HealthyYouTXT evaluations, suggesting utility in emphasizing them in messages. Higher destiny beliefs predicted lower interest and perceived efficacy, suggesting they could impede program use. In Stage 3, we implemented the mixed-methods findings to generate a revised HealthyYouTXT en Español. The emergent linguistic principles and multi-stage, multi-methods process can be applied beneficially in health communication adaptations.
Keywords: mHealth, Latino, intervention, health communication, nutrition
Cultural and Linguistic Adaptation of a Healthy Diet Text Message Intervention for Hispanic Adults
Unhealthy eating represents a serious health issue worldwide. Diets high in fat and low in produce and whole grains are common (Fryar, & Ervin, 2013; Rennie, Johnson, & Jebb, 2005). For example, U.S. adults consume on average 1.1 servings of fruit and 1.6 of vegetables per day (CDC, 2013), well under the recommended 1.5-2 fruits and 2-3 vegetables per day (USDA, 2016). Unhealthy eating contributes to high obesity rates (Kushner, 2010); currently, 69% of U.S. adults are overweight or obese (CDC, 2014). Obesity increases risk for multiple conditions including diabetes, heart disease, and cancer (Hu, 2003; Song et al., 2015; The, 2011). Diet behavior change interventions could help reduce obesity and related comorbidities (Sampsel & May, 2007).
Programs to improve diet must be disseminated in ways that achieve broad reach, particularly within vulnerable minority populations (Glasgow, Klesges, Dzewaltowski, Bull, & Eastabrooks, 2004; Kagawa-Singer et al., 2015). Behavior change interventions are more successful when culturally relevant and in the dominant language of the group (Bender, Harbour, Thorp, & Morris, 2001; Dyson, 2015; Pottie, Hadi, Chen, Welch, & Hawthorne, 2013). Transforming messages to enhance cultural relevance involves infusing them with cultural themes and values, using culturally meaningful terms, and meeting the information needs of the group (Kreuter et al., 2003; Quinn et al., 2006; Ramirez, 2013; Simmons, Cruz, Brandon, & Quinn, 2010; Solomon et al., 2005).
Hispanics represent a critical target for culturally-adapted diet interventions. Hispanics are the largest ethnic minority group in the U.S.; accounting for 54 million residents (2014 Census) this group is projected to grow to 31% of the U.S. population and 49% of the California population by 2060. Moreover, Hispanics (versus non-Hispanic Whites) have higher rates of obesity and obesity-related illnesses (Dominguez et al., 2015). Yet reaching Hispanics with effective health communications remains a challenge, partly because language barriers limit their use of English-language programs. One-third of U.S. Hispanics are Spanish monolingual (7%) or speak English less than very well (26%; Krogstad, Lopez, & Rohal, 2015).
The aim of this formative research was to translate HealthyYouTXT, a mobile phone-based health promotion (mHealth) program developed by the U.S. National Cancer Institute (NCI), into HealthyYouTXT en Español, a linguistically and culturally appropriate version for Spanish speakers. We report a multi-stage, iterative process through which we culturally adapted the text messages, used a mixed-methods approach with qualitative and quantitative methods to test their acceptability, and revised the program based on the findings.
mHealth Interventions for Behavior Change
mHealth programs represent a potentially powerful tool for health communication. They promote healthy choices by targeting beliefs, motivations, and support delivery through interactive communications that reach users “in the moment” as they go through daily activities. Many mHealth programs are designed to assist cigarette smokers in quitting, and growing evidence supports their efficacy (Free et al., 2011; Whittaker et al., 2009). Other mHealth programs promoting healthy behavior change include interventions targeting maternal and child health (Ditta, Ranganathan, & Sivakumar, 2014) and alcohol use (Mason, Benotsch, Way, Kim, & Snipes, 2014). mHealth diet programs are popular among consumers; although evidence of their effectiveness is currently limited, their potential for disease prevention warrants their study (Burke, et al., 2015; Kumar, et al., 2013). mHealth approaches hold particular promise for Hispanic communities, where cell phone use is higher than for non-Hispanic Whites (Lee et al., 2012). Further, many Hispanic communities live in rural regions with access to clinic-based health promotion.
The HealthyYouTXT Program
NCI recently developed HealthyYouTXT to promote healthy dietary practices. HealthyYouTXT, available free of charge to continental U.S. residents, sends users one to five text messages each day for several weeks. Implementing principles of self-regulation and Self-Determination Theory (SDT; Williams, Ryan, & Deci, 2015), the messages provide advice, non-judgmental support, and positive feedback on healthy eating progress. Consistent with SDT, the program promotes autonomous (intrinsic) motivations to eat healthy rather than controlled (extrinsic) motivations to do so or amotivation (lack of motivation). The messages target autonomous motivation by emphasizing personal control (e.g., emphasizing personal choice in setting goals and selecting healthy foods), connectedness with others (e.g., personalized messages conveying support and understanding), and competence (e.g., providing action plans or highlighting successes). NCI's longer-term goals include tailored versions of HealthyYouTXT for multiple segments of the population including adolescents, pregnant women, and cultural groups. The present project represents an early step in this process: Developing a culturally appropriate Spanish version of HealthYouTXT.
One aspect of HealthyYouTXT that could influence its acceptability, efficacy, and effectiveness is the cultural relevance of its theoretical framework. SDT and related self-regulation theories were developed through research conducted mainly with non-Hispanic samples in the U.S. These principles focus primarily on individualistic values and motives such as autonomy. Yet for Hispanics, these individualistic values may be less important than cultural values and beliefs in guiding health behaviors. Values widely held in Hispanic cultures include familism (familismo—prioritizing family values over individual interest; Campos et al., 2014; Perez & Cruess, 2011); fatalism (fatalismo—beliefs that events are pre-determined and cannot be changed; Abraido-Lanza et al., 2007, de los Monteros, 2013); and destiny (destino—beliefs that outcomes are destined to occur; Floréz et al., 2009). Studies have found positive associations of familism with healthy behaviors (Fisher et al., 2000; Perez & Cruess, 2011); social support from family and obligations to be healthy for the sake of one's family appear to drive this relationship. On the other hand, family obligations could be prioritized over individual health needs and undermine self-care (Katiria Perez & Cruess, 2014). Fatalism can lead to avoidance of health behavior change (Chavez, Hubbel, Mishra, & Valdez, 1997; Umezawa, Kagawa, Leake, Maly, & You, 2012). Destiny beliefs have also been associated with unhealthy habits (Carpenter & Colwell, 1995; Colón, 1992), although evidence suggests that it could sometimes motivate healthy behaviors (Floréz et al., 2009). These values could shape interest and perceived efficacy of HealthyYouTXT for Hispanic consumers.
Study Aims
This formative research focused on developing a Spanish-language version of HealthyYouTXT using a three-stage, mixed-methods process of cultural adaptation. In Stage 1, we conducted initial translations and adaptations of the text libraries using an iterative, principle-guided process. In Stage 2, we used mixed methods including focus groups and surveys with Hispanics to evaluate the acceptability and cultural appropriateness of the program. We also used survey data to evaluate whether individualistic factors of autonomous motivation, controlled motivation, and amotivation and beliefs about familism, fatalism, and destiny predict program interest and its perceived efficacy. Our analyses tested these hypotheses and research question.
H1: Consistent with SDT, higher autonomy motivations predict higher interest and perceived efficacy whereas controlled motivations and amotivation predict lower interest and perceived efficacy.
H2: Higher familism and lower fatalism and destiny beliefs predict higher interest and perceived efficacy.
Given the importance of gender roles in Hispanic cultures (Chuang & Tamis-LeMonda, 2013), cultural values shaping program interest and evaluations might differ for men and women. Research reveals gender differences in associations of cultural values with health outcomes; e.g., familism correlates with better mental health for men but not women (Lugo & Steidel, 2006) whereas fatalism correlates with poorer health outcomes for women but not men (Urizar & Sears, 2006).
RQ1: Does gender moderate relationships of cultural beliefs with program interest and perceived efficacy?
In Stage 3, we revised the text libraries by implementing the qualitative and quantitative findings through an iterative revision process.
Method
Overview of the Translation and Cultural Adaptation Process
Figure 1 presents the three-stage process used to create HealthyYouTXT en Español: (1) Initial translation and development of culturally-relevant text messages; (2) Mixed-methods study examining the acceptability of the program and text messages; and (3) implementation of the findings to revise the messages and program. We detail these stages below. The university's Institutional Review Board approved the study.
Figure 1. Overview of the Cultural Adaptation Process.

Stage 1 Procedures: Initial Spanish Translation and Adaptation
HealthyYouTXT is accessed at http://smokefree.gov/healthyyou. We conducted initial translations and adaptations of the text libraries into Spanish through multiple iterations of activities. These activities included research team discussions of linguistic principles and cultural themes guiding the translations (all authors), message translations made collaboratively by bicultural researchers fluent in Spanish (AD, MU), and back-translations made independently by bicultural, Spanish-speaking researchers (RC, SP). Examples of linguistic principles include: (1) Use of short words and sentences, due to the 160 character limit for texts and the longer length of Spanish words relative to their English counterparts; (2) Use of alternative words with no tildes or accents when possible, since many cell phones do not display symbols; and (3) Use of Pan-American words accessible to most Spanish speakers; e.g., platano (note missing accent, as displayed in texts) instead of guineo or banano. Examples of thematic principles include: (1) Infusion of familism into messages with references to family, such as information about benefits of healthy eating within the family and suggestions for family meals; (2) Focus on culturally relevant foods, including popular fruits (e.g., avocados and oranges), vegetables (e.g., jicama and peppers), dishes (e.g., salsa and caldos), and spices (e.g., cilantro and cinnamon); (3) Use of friendly tone while avoiding commanding language (e.g., “Stocking up your pantry with healthy foods can help you stay on track” rather than, “To stay on track, you must stock up your pantry with healthy foods”); and (4) Use of language reflecting support (apoyo) rather than help (ayuda), as the latter implies vulnerability or lack of ability to do something oneself that could challenge machismo (masculine pride).
We focused on creating culturally relevant messages while preserving the SDT themes of autonomy. For example, the following message was adapted to preserve the autonomy focus: “El cambiar sus habitos alimenticios tiene sus pasos y toma tiempo. Como empezara? Hoy intente comer menos comida grasosa o salada. Usted decida! (Changing your eating habits has steps and takes time. How will you start? Today try eating less fatty or salty food. You decide!).” Table 1 provides examples of initial adaptations and their back-translations.
Table 1.
Examples of Culturally Adapted Text Messages.
| Text Message Version | Key Constructs Targeted by Text Message: Autonomy, Choice | Key Constructs Targeted by Text Message: Family Support | Key Constructs Targeted by Text Message: Control, Practical Steps to Facilitate Action | Key Constructs Targeted by Text Message: Control, Practical Steps to Facilitate Action |
|---|---|---|---|---|
| English Version | Cutting out all treats can feel like punishment. Take charge by selecting when and if you have treats. It's your choice! | When kids have a part in planning or putting together meals, healthy eating becomes “theirs.” Find age-appropriate ways to get them involved. | It's corn season! Take those kernels off the cob & try out this yummy side dish: [LINK] | Is the Thanksgiving menu out of your hands? Try going for smaller portions & white meat, instead of dark – easy on the gravy. |
| Initial Spanish Translation | Dejar de comer sus antojitos puede parecer como un castigo. Tome control decidiendo si va a comer sus antojitos y cuando. Es su decision! | Sus hijos se sienten incluidos cuando toman parte en planear o preparar alimentos. Encuentre formas apropiadas a su edad para que participen. | Es temporada de elotes! Saque la mazorca de la hoja y pruebe este delicioso platillo: [ENLACE] | No tiene control de lo que se servira durante el dia de gracias? Trate de comer porciones chicas, carne blanca y no mucho jugo de carne. |
| Back-Translation | To stop eating your snacks can seem like a punishment. Take control by deciding if you will eat your snacks and when. It is your decision! | Your children feel included when they take part in planning or preparing dishes. Find appropriate forms to their age so they participate | It's the season of corn! Take the cob out of the husk and try this delicious dish: [LINK] | You don't have control over what is served during Thanksgiving? Try to eat smaller portions, white meat and not too much meat juice. |
| Adapted Spanish Version | Dejar de comer sus antojitos es un buen sacrificio para el bienestar de su familia. Limite cuando y cuantos antojitos comen. Es su decision! | Para que sus hijos se sientan incluidos en sus decisions, invitelos a planear o preparar alimentos. Intente actividades apropiadas para sus hijos. | Es la temporada del elote! Comalos de manera saludable y deliciosa. Evite grasas y solo use limon y chile en lugar de mayonesa y mantequilla. | Vienen los dias festivos. Tiene menos control en estas fechas? Coma porciones mas chicas, comidas bajas en grasas, y pollo en vez de carne roja. |
| Back-Translation of Adapted Spanish Version | To quit eating your snacks is a good sacrifice for the wellbeing of your family. Limit when and how many snacks you all eat. It is your decision! | So that your children feel included in your decisions, invite them to plan or prepare dishes. Aim for activities appropriate for your children. | It's the season of corn! Eat them in a healthy and delicious way. Avoid fats and only use lemon and chili instead of mayonnaise and butter. | The holidays are coming. Do you have less control on these dates? Eat smaller portions, foods low in fat, and chicken instead of red meat. |
| Key Cultural Adaptation | Familism: Healthy eating for the well-being of one's family; making choices for the family | Familism: A clearer focus on personal actions one can take to promote children's participation in meal preparation | Traditional foods: Provides a healthier alternative for a traditional and popular recipe for corn on the cob with mayonnaise and chili | Traditional holidays: The adaptation includes all holidays as Hispanics celebrate other holidays before Thanksgiving; it also uses clearer and more appropriate phrases and examples |
Stage 2 Procedures: Formative Evaluations of the Acceptability of HealthyYouTXT en Español
Design
Our mixed-methods approach combined quantitative survey methods with a grounded–theory, qualitative methodology using focus group interviews (Corbin & Strauss, 1998). Grounded theory methods are designed to yield coherent patterns of dominant themes and their interconnections as derived from interview data.
Participants
We recruited participants through invitations to people attending community events such as health fairs, flea markets, church and school events, and English language classes. Inclusion criteria were self-identification as Hispanic or Latino; 18 years or older; residence in the local, primarily rural region; interest in eating healthier; and regular cell phone use. In total, 109 adults completed an initial survey and focus group session; 101 (93%) completed a follow-up survey one week later.
Procedure
Interested individuals contacted a researcher who verified inclusion criteria and scheduled a session. Four facilitators (AD, RC, SP, MU) conducted focus group sessions; two facilitators at each session. Each session (14 in Spanish, 10 in English) included same-gender participants (4-6 participants on average). After providing informed consent, participants completed a survey with measures of socio-demographic characteristics, cultural beliefs, and SDT motivations. The facilitator then led a videotaped discussion using a semi-structured interview guide. Participants received $20 gift cards upon completion. One week later, participants were mailed a survey with measures of HealthyYouTXT interest and perceived efficacy. Each received a $20 gift card after returning the survey.
Survey Measures
Table 1 presents the socio-demographic characteristics assessed. Table 2 presents the measures of cultural beliefs (initial survey), SDT constructs (initial survey), and measures of program interest and perceived efficacy (follow-up survey). Measure scores reflect item means.
Table 2.
Demographic, Media Use, and Health Characteristics of the Sample.
| Characteristic | Mean (range) / Percent (N = 109) |
|---|---|
| Age | M = 36.15 (range: 18-75) |
| Gender: | |
| Females | 74% |
| Males | 26% |
| Marital Status: | |
| Married/Living with Partner | 68% |
| Single/Never married | 25% |
| Language Preference: | |
| Spanish | 67% |
| English | 33% |
| Education: | |
| Elementary-8th grade | 42% |
| High school or GED | 24% |
| Some college | 32% |
| Employment: | |
| Fulltime | 22% |
| Part time | 18% |
| Not employed | 60% |
| Household Income: | |
| < $20K | 68% |
| $20-34K | 13% |
| $35-74K | 12% |
| $75K or more | 3% |
| Nativity: | |
| Mexico | 58% |
| US | 40% |
| Generation: | |
| First (Born in Mexico) | 58% |
| Second (Born in U.S., 1+ immigrant parent) | 19% |
| Third or more (Born in U.S.,U.S.-born parents) | 23% |
| Own cell phone | 100% |
| Use phone to text | 81% |
| Self-rated health: | |
| Excellent | 8% |
| Very good | 20% |
| Good | 32% |
| Fair | 33% |
| Poor | 5% |
| Body Mass Index: | |
| <25 | 29% |
| 25-29 | 42% |
| 30+ | 29% |
The familism measure of family values related to food choices was adapted from a general measure of Hispanic familism (Gaines et al., 1997). The items assess the importance of traditional foods, family obligations to eat a healthy diet, and general family values. For fatalism, a standard measure (Shen, Condit, & Wright, 2009) was shortened and adapted to target fatalistic beliefs about diet and health. The destiny beliefs measure included three items used by Florez et al. (2009), two of which were adapted to target diet-related beliefs. SDT motivations were assessed with the SDT Questionnaire-Diet Version (Williams, Ryan, & Deci, 2014), which includes subscales for autonomous motivation, controlled motivation, and amotivation. The follow-up survey included measures of interest in HealthyYouTXT and perceived efficacy of HealthyYouTXT.
Semi-structured interview guide
A focus group guide provided a standardized set of open-ended questions and prompts. Participants were first asked about their reasons for wanting to improve their diet, perceived benefits and barriers, and concerns about changing these behaviors. Example questions are, “What do you consider to be a healthy diet?” and “What are some of the challenges or difficulties in trying to eat a healthy diet?” The facilitator then introduced HealthyYouTXT along with examples of texts and asked participants about their initial reactions and interest. Example questions are, “What do you think about the idea of receiving text messages to help you eat better?” and “Is this something you would be interested in?” Participants then viewed selected texts and discussed their cultural appropriateness and effectiveness. Example questions are, “How useful do you believe this text message will be as a support to changing your diet?” and “How appropriate is the language for you/your friends/your family?”
Data analysis
For descriptive analyses of socio-demographic characteristics, we calculated percentages or means (ranges) and used χ2 and t tests to assess gender differences in these factors. For qualitative analyses of focus group data, recordings were transcribed verbatim by trained transcribers and checked for accuracy by a second transcriber. We conducted thematic analyses of the transcripts using an inductive, iterative approach. We developed coding categories by progressing from open (descriptive) coding to an analytical coding framework wherein original codes were revised, merged, and refined until a coherent set of themes emerged and we reached consensus on the final coding framework and interpretive analysis.
For quantitative analyses of survey evaluations of HealthyYouTXT, we calculated means (SD) for descriptive evaluations and t tests to examine gender differences. We then conducted regression analyses to test whether SDT motivations (autonomy, controlled, and amotivation) and cultural beliefs (familism, destiny, and fatalism) predict HealthyYouTXT interest and perceived efficacy. These analyses tested whether gender moderates relationships of cultural beliefs with interest and efficacy using Gender X Belief interaction terms, with independent variables centered about the mean. Significant interactions were graphed using independent variable values of ± 1 SD from means. Preliminary regression analyses included all main and Gender X Belief interaction terms and tested demographic and personal characteristics as potential covariates. The final models included only those variables emerging as significant predictors (main effects or in interaction with gender) of interest or perceived efficacy.
Stage 3 Procedures
Using findings from the quantitative and qualitative analyses, we further adapted the Spanish messages through multiple iterations of research team discussions (all authors), message revisions made collaboratively by two researchers (AD, MU), and back-translations made independently by two researchers (RC, SP).
Results
Stage 1 Results
The initial translation and adaptation process yielded Spanish versions of the four HealthyYouTXT libraries. The authors reached consensus that all text messages were consistent with the guiding translational, linguistic, and thematic adaptation principles.
Stage 2 Descriptive Results: Sample Characteristics and Overall Evaluations of HealthyYouTXT
Table 1 presents socio-demographic, media use, and health characteristics of the sample. The majority was female, married/living with a partner, and preferred Spanish over English focus groups and surveys. Overall, 42% completed school by 8th grade; 60% were unemployed; two-thirds had household annual incomes under $20,000. Over half were first-generation Mexican-Americans. Over 80% used their cell phones for texting regularly. Almost 40% reported fair or poor health. Based on body mass indices (BMI), 71% were overweight.
Men and women did not differ in age, marital status, education, nativity, generational status, or cell phone use. Women (84.5%) were more likely than men (55.6%) to report annual incomes below $20,000; χ2(3,N=100)=15.87, p<.01). Women (73.1%) were also more likely than men (26.9%) to be unemployed, χ2(2, N=100)=9.21, p<.05; and to report fair or poor health and to report fair or poor health (52.0% versus 25.0%, respectively), χ2(4,N=100)=12.01, p<.05.
Stage 2 Qualitative Results: Analysis of the Focus Group Data
Thematic analyses of focus group data revealed five primary themes about challenges to healthy eating, views of HealthyYouTXT, and reactions to translated messages: (1) Social environments do not support healthy eating; (2) Self-regulation and support facets of HealthyYouTXT are salient and appealing; (3) A generational divergence in preferences for formal language exists; (4) Absence of Spanish grammatical symbols undermines the credibility of the program; and (5) Diminutive language softens suggestions and makes them more acceptable. The analyses also identified specific problematic terms in messages.
Social environments do not support healthy eating
Participants voiced strong views that, although they were interested in improving their diet, multiple forces within their social environment prevent them from doing so. Many identified lack of time and lack of healthy recipes as key factors impeding healthy eating efforts. High prices of healthy foods emerged as a critical barrier; many noted difficulties in affording what they perceived to be healthy foods:
“Maybe the fact that organic foods are more expensive. So I mean we really want to eat very healthy but if we buy a gallon of organic milk it is more expensive than the regular one.”
(female, age 46)
“Cost of the good food. The good food is more expensive than processed foods”
(male in his 40s).
Participants, and women in particular, noted resistance or lack of support from family members as barriers to healthy eating:
“What happens is that sometimes when one wants to eat healthy, the others don't want the same thing and one cannot be making two or three different kinds of food.”
(female, age 36).
“The children also, sometimes they don't help a lot. As a mom I want the best for them but they always say “I don't like it, I don't like it, and I don't like it.”
(female, age 36)
Positive resonance to self-regulation and support aspects of HealthyYouTXT
Participants generally expressed positive views about HealthyYouTXT. They resonated in particular to the sense of social support provided by the program:
“Sometimes that is what one needs, someone to tell us “you can do it” or “don't eat this or that.” Someone that is there for you and that is making you feel like you matter and takes your effort into account”
(female, age 41).
Participants also resonated to aspects promoting effective self-regulation, such as prompts to action:
“I think it will serve as a good reminder,”
(female, age 26)
“It makes me think more about eating healthier. You know just to get that little hint or something”
(female, age 21)
“It would be like a little more encouragement for somebody who wants to but doesn't think about it constantly.”
(female, age 38)
Generational divergence in preferences for use of formal language
Participants expressed strong views about the use of formal language (e.g., “usted”), with debates arising in many focus groups. Whereas older participants tended to report that use of formal language was appropriate and showed respect, younger participants tended to find it off-putting and suggested that informal language (e.g., tú) would be friendlier and more effective. Examples of views held by older participants included:
“‘Usted’ is used with respect, and the informal “tú” is used when you know the person. The formal sounds more educating, as well, so I think it is better”
(female, age 43).
In contrast, younger participants tended to prefer informal language:
“I think that if they send it to me with “tú” I would feel more comfortable and I would take it as if the text was directed to me, as if the program really knew me. And I think I would take the message more seriously. Yes, because like [usted] is kind of like anyone is just talking to me but if you use “tú” then I would take it as if the program really knew me and I would take it more seriously.”
(female, age 19).
Absence of Spanish grammatical symbols undermines the credibility of the program
Some felt that the lack of Spanish grammatical symbols (e.g., tildes, accents, and inverted question or exclamation marks) made the program seem less credible and, consequently, less relevant personally. Although the sentiment was not shared by all participants, those who objected had strong feelings about this.
“…yes, [it bothers me] because it should be written correctly, if they are trying to make this appropriate for us…”
(female, age 24).
“That kind of things bother me a lot because I am very proud of my language and I like to see it written appropriately. It's like in English when people start writing “ur” instead of “you are.”
(male, age 46).
“If they are providing information it will affect their credibility because they don't know how to write properly”
(female, age 25).
Use of diminutives positively softens dietary suggestions
Participants identified the use of diminutives such as “antojitos” (little snacks) and “poquito” (very little). These terms appear to soften the tone of the suggestions, making the changes seem “little” while enhancing the friendliness of the tone.
“I like it a lot that it says “antojitos” in this messages, it sounds friendly”
(female, age 24).
Identification of problematic terms
Participants identified specific terms that seemed problematic and suggested alternatives. In particular, consensus emerged that use of “comida chatarra” for “junk food” was inappropriate. Participants found this term to be value-laden and suggested alternatives, including the English term “junk food”.
“To us “comida chatarra” includes everything that is not good.”
(female, age 36).
“To me [“junk food”] is a very common word among those of us who speak Spanish. To me that is more common that saying ‘comida chatarra’ or ‘comida grasosa’” (greasy food).
(female, age 31)
“Comida chatarra” is like you are despising that food”
(female, 43)
“but when it comes to writing it down “comida chatarra” would be the one that includes everything we shouldn't eat”
(female, age 40)
Difficult-to-understand or unfamiliar terms included blueberries, kale, chard, and dark chocolate. Terms found to be culturally irrelevant for some Hispanics included jitomate (for tomato), especias (for spices), transformar (transform), despensa (pantry), and jornada (journey as a metaphor for progress in changing diet).
Stage 2 Quantitative Results: Survey Evaluations of HealthyYouTXT
Interest in healthy diet text messages
Survey responses revealed strong interest in HealthyYouTXT. Mean interest ratings (ranging 1-7) were comparably high for women (M=5.38, SD=1.49) and men (M=5.14, SD=1.92). Moreover, 70% of participants had interest scores over 4.0.
Perceived efficacy
Participants generally perceived HealthyYouTXT as highly efficacious in promoting healthy diet and weight loss. Mean perceived efficacy ratings were similar for women (M=5.45, SD=1.15) and men (M=5.87, SD=1.50).
Cultural beliefs and SDT motivations as predictors of HealthyYouTXT interest and perceived efficacy
Regression analyses revealed that no personal characteristics except gender predicted program interest and perceived efficacy; therefore, the final analyses included gender only. Fatalism, controlled motivations, and amotivations did not predict either interest or perceived efficacy and so were omitted from the final models. Familism, destiny, and autonomy motivations predicted one or both dependent measures and were therefore retained in the final models. Gender did not moderate relationships of destiny and autonomous motivations with interest or perceived efficacy; the final models thus omitted these interaction terms.
Table 4 presents the final regression models. For interest in HealthyYouTXT, higher destiny beliefs predicted lower interest. Gender moderated the relationship of familism with interest; higher familism predicted greater interest for men but not for women (Figure 2). For perceived efficacy, higher destiny beliefs were marginally associated with lower perceived efficacy; autonomous motivations predicted higher perceived efficacy. Gender again moderated familism: higher familism predicted higher perceived efficacy for men but not for women (Figure 2).
Table 4. Regression Analyses of Gender, Familism, Destiny Beliefs, and Autonomous Motivation as Predictors of Interest and Perceived Efficacy of HealthyYouTXT.
| Predictor Variable | B | SE B | β | t | CI (95%) |
|---|---|---|---|---|---|
| DV: Interest | |||||
| Gender | -0.43 | .33 | -.12 | -1.28 | -1.09 -0.23 |
| Destiny Beliefs | -0.75 | .20 | -.36 | -3.76*** | -1.14 -0.35 |
| Familism | 0.25 | .25 | .11 | 1.01 | -.24 0.74 |
| Autonomous Motivation | 0.12 | .19 | .06 | 0.64 | -0.25 0.50 |
| Gender X Familism | 1.31 | .51 | .26 | 2.56** | 0.29 2.32 |
| DV: Perceived Efficacy | |||||
| Gender | 0.29 | .27 | .10 | 1.06 | -0.25 0.83 |
| Destiny Beliefs | -0.32 | .16 | -.20 | -1.95+ | -0.64 0.00 |
| Familism | -0.07 | .20 | -.04 | -0.37 | -0.47 0.33 |
| Autonomous Motivation | 0.35 | .15 | .22 | 2.28* | 0.05 0.66 |
| Gender X Familism | 0.94 | .42 | .24 | 2.24* | 0.11 1.76 |
Note. DV = Dependent variable. For Interest, model F(5,95) = 6.26, p < .001. For Perceived Efficacy, model F(5, 95) = 4.39, p = .001.
p = .054
p < .05
p < .01
p < .001
Figure 2.
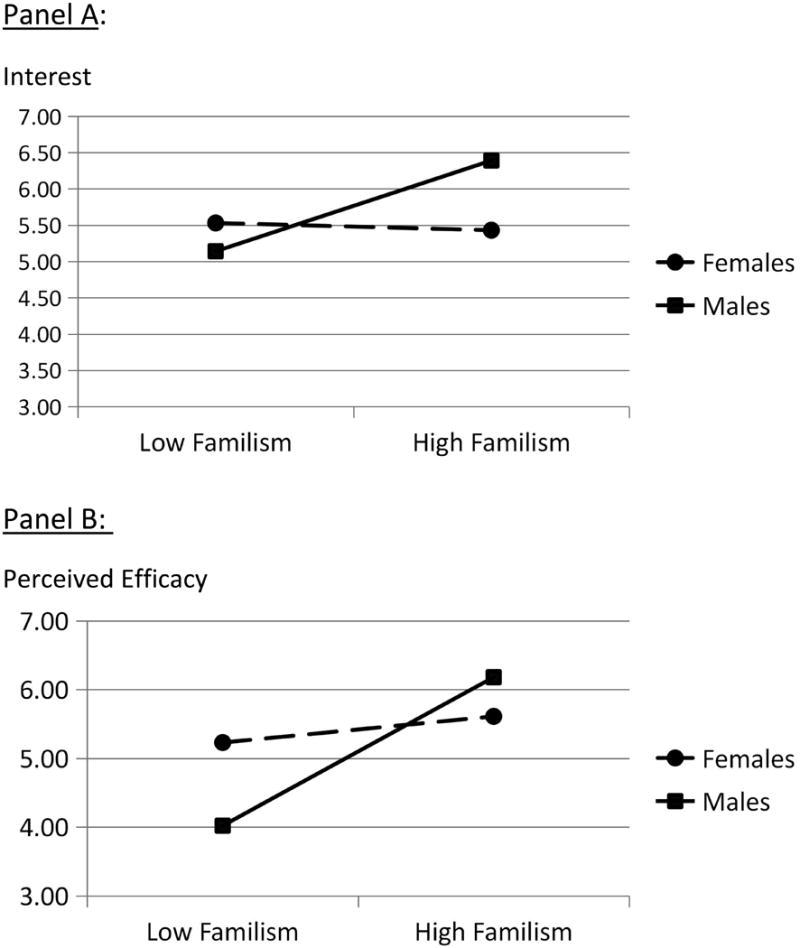
Moderating Effects of Gender on the Relationship of Familism with Interest in HealthyYouTXT (Panel A) and Perceived Efficacy of HealthyYouTXT (Panel B).
To summarize, analyses partially supported the hypotheses. Consistent with H1, higher autonomy motivations predicted greater perceived efficacy. Contrary to H1, autonomous motivations did not predict interest and controlled motivations and amotivations were unrelated to either interest or perceived efficacy. Consistent with H2, lower destiny beliefs predicted greater interest and (marginally) perceived efficacy, and higher familism predicted greater interest and perceived efficacy for men (although not for women). Contrary to H2, fatalism did not predict either interest or perceived efficacy. Regarding RQ1, analyses indicated that gender moderates the relationships of familism with both interest and perceived efficacy; it does not moderate the relationships of fatalism or destiny with these attitudes.
Stage 3 Results
We applied the qualitative and quantitative findings in revising the text libraries to enhance their cultural appropriateness (see Table 1 for examples of adapted messages and their key cultural adaptations). We revised messages to preserve and enhance emphasis on autonomy (e.g., messages conveying choice and control) and family values (e.g., messages about family engagement; healthy diet choices and benefits for family members). Given the split in preferences for formal (usted) versus informal (tú) language, we developed formal and informal versions of the text libraries. The final HealthyYouTXT en Español program will be available to consumers in late 2016.
Discussion
The multi-stage, mixed-methods process used to transform HealthyYouTXT into HealthyYouTXT en Español yielded insights into its potential efficacy and reach for Spanish speakers and led to substantial improvements in the final text libraries. This process builds on translation and transcreation procedures using qualitative methods in adapting health education materials (Ko et al., 2014; Quinn et al., 2006; Simmons et al., 2010; Solomon et al., 2005) by combining qualitative with quantitative methods to inform the adaptation.
Mixed-methods analyses revealed substantial interest in HealthyYouTXT, with most participants expressing moderate or strong interest in using it. Moreover, participants on average viewed it as highly efficacious in promoting healthy diet and weight loss. These high levels of interest and perceived efficacy suggest that Hispanics are likely to initiate program use.
Qualitative findings reveal that unsupportive social environments represent a primary barrier to healthy eating for Hispanic community members. In turn, participants identified the encouragement, support, and self-regulation aids (e.g., prompts to take specific actions) as particularly beneficial features of HealthyYouTXT. By providing advice and assistance in generating family support for healthy eating, the program could help users overcome critical constraints within unsupportive environments.
Both cultural beliefs (i.e., beliefs in destiny and, for men, high familism) and SDT motivations (i.e., autonomy) predict evaluations of HealthyYouTXT. Higher destiny beliefs predicted lower interest and perceived efficacy, suggesting that they could be a barrier to program use. In developing the final translations, we avoided use of terms that might trigger considerations of destiny. This finding could be applied further by developing media for HealthyYouTXT promotion that emphasize personal control and ability to change disease risk. Communications could potentially harness the influence of destiny beliefs by highlighting how the program can help individuals achieve their true destiny of being healthy.
Higher familism predicted greater interest and perceived program efficacy for men, although they were unrelated to interest or perceived efficacy for women. Further research could test whether men high (versus low) in familism are more likely to use HealthyYouTXT, and whether they are relatively more responsive to messages about behaviors involving family and more likely to encourage family members to change their diets.
The positive association of autonomy motivations with perceived efficacy of HealthyYouTXT supports its importance in promoting positive program evaluations for Hispanics. Given that promotion of autonomy is an integral component guiding the HealthyYouTXT contents, this study lends promising evidence that Hispanics might respond positively to the program and that increasing their autonomy motivations could promote behavior change. From a broader theoretical perspective, these findings suggest value in integrating both cultural beliefs and SDT motivations into theoretical models to better capture key drivers of healthy behaviors in diverse populations.
Qualitative findings revealed aspects of the Spanish messages that could undermine program interest and efficacy. First, participants were divided in their reactions to the use of the formal (usted) language. Whereas older adults tended to view it as appropriate and respectful, younger adults tended to feel that informal (tú) language would be friendlier and more personal. Providing consumers signing up for the program with the option for formal or informal text messages could enhance message persuasiveness and program adherence. This choice could also attract use by conveying respect for this important aspect of Spanish language and culture and by promoting a sense of autonomy and control. Second, focus groups revealed numerous terms that were culturally inappropriate (e.g., “comida chatarra” for junk food) and terms that could be used to greater effect (e.g., diminutives to soften suggestions). We implemented these findings in the adapted translations of the libraries. Finally, the lack of Spanish grammatical symbols tended to undermine the perceived credibility and cultural appropriateness of HealthyYouTXT. At the time of writing, many phones lack the functionality to exhibit these symbols; including them would thus make the program less accessible and interpretable for Spanish speakers who cannot afford sophisticated phones. Until phones with symbol functionality become standard, Spanish mHealth programs could offer explanations of this message feature to users at the time of registration to show understanding and respect of the importance of Spanish grammar. Synonyms without these symbols should be used when possible.
Research strengths included a sample of a hard-to-reach population of Spanish speakers who, living in rural communities, have low access to clinic-based health promotion services and high reliance on mobile phones for communications. These communities are particularly likely to benefit from minimal-cost mHealth programs such as HealthyYouTXT and thus represent important segments to reach. The participants were primarily of Mexican origin; with 64% of U.S. Hispanics and 82% of California Hispanics are of Mexican origin (Census, 2010; Census, 2014), the sample represents a substantial proportion of Spanish speakers with access to HealthyYouTXT en Español. The generalizability of findings to other Hispanic subgroups warrants further study. The sample included fewer men than women, an imbalance potentially due to Hispanic men having relatively less interest in diet behavior (Anderson et al., 1998) or group discussions (Umaña-Taylor & Bámaca, 2004).
To conclude, the study revealed strong interest and positive evaluations of HealthyYouTXT among Hispanic men and women. The findings guided revisions to the Spanish libraries to enhance their acceptability and cultural relevance. They support further research evaluating the efficacy and effectiveness of HealthyYouTXT en Español in promoting healthy diets for Spanish speakers. If effective, it could help reduce health disparities associated with poor nutrition for these vulnerable populations. Findings supporting specific linguistic principles can be applied in future communications adaptations. The multi-stage, multi-methods approach holds promise for use in formative research to adapt health communications into another language or for different cultural communities.
Table 3. Measures of Cultural Values and Beliefs, Self-Determination Theory (SDT) Motivations, and HealthyYouTXT Interest and Perceived Efficacy.
| Measurement | Items |
|---|---|
| Familism a (α = .74) |
I will do all that I can to keep alive the traditional foods and recipes passed on to me by my parents and grandparents. It is important to keep alive the traditional meals and celebration foods set in place by my family. When I am far away from home, eating traditional foods helps me feel connected to my family. Sharing traditional meals with my family is very important. I would eat a healthier diet if my family wanted me to. I have an obligation to eat healthy foods to stay healthy for my family. I rely on my family to show me what to eat. What my family serves me is what I eat. I cannot imagine what I would do without my family. I will do all that I can to keep alive the traditions passed on to me by my parents and grandparents. |
| Fatalism a (α = .84) |
My health is determined by fate. If someone is meant to get a serious disease, they will get it no matter what they do. If someone is overweight, that's the way they were meant to be If someone is meant to be overweight, it doesn't matter what kinds of food they eat, they will be overweight anyway. My health is a matter of luck. I will become overweight if I am unlucky. How many years of life I have is a matter of luck. I often feel helpless in dealing with the problems of life. Everything that can go wrong for me does. Sometimes in life, I feel that I'm easily pushed around”. |
| Destiny Beliefs a (α = .66) |
I think if it is a person's destiny to be overweight, that is the way it will be. I think if a person is destined to become overweight, he or she will become overweight no matter what he or she does. Since birth, we all have a destiny that we cannot change. |
| SDT Motivations b | The reasons I would eat a healthy diet are… |
| Autonomous (α = .84) |
9 items; e.g: …because I feel that I want to take responsibility for my own health. |
| Controlled (α = .67) |
6 items; e.g: …because others would be upset with me if I did not. |
| Amotivation (α = .64) |
3 items; e.g: …I really don't think about it. |
| Interest in HealthyYouTXT c (α = .93) |
If you were to have a cell phone and you were able to use this program free of charge… How curious would you be to learn more about the HealthyYou TXT program? How interested would you be in using the HealthyYouTXT program? How likely is it that you would use the HealthyYouTXT program? |
| Perceived Efficacy of HealthyYouTXT c |
If you were to have a cell phone and you were able to use this program free of charge… How much do you think this program will help you eat a healthier diet? If you wanted to lose weight, how much do you think the HealthyYouTXT program would help you to lose weight? In general, do you think the HealthyYouTXT program will help other people eat a healthier diet? In general, do you think the HealthyYou TXT program will help other people lose weight? |
Note.
Ratings: 1 (strongly disagree) to 5 (strongly agree).
Ratings: 1 (not at all true) to 7 (very true).
Ratings: 1 (not at all) to 7 (very much).
References
- Abraído-Lanza AF, Viladrich A, Flórez KR, Céspedes A, Aguirre AN, De La Cruz AA. Commentary: Fatalismo reconsidered: A cautionary note for health-related research and practice with Latino populations. Ethnicity & Disease. 2007;17:153. [PMC free article] [PubMed] [Google Scholar]
- Anderson RM, Goddard CE, Garcia R, Guzman JR, Vazquez F. Using focus groups to identify diabetes care and education issues for Latinos with diabetes. The Diabetes Educator. 1998;24:618–624. doi: 10.1177/014572179802400507. [DOI] [PubMed] [Google Scholar]
- Bender DE, Harbour C, Thorp J, Morris P. Tell me what you mean by “si”: Perceptions of quality of prenatal care among immigrant Latina women. Qualitative Health Research. 2001;11:780–794. doi: 10.1177/104973230101100607. [DOI] [PubMed] [Google Scholar]
- Burke LE, Ma J, Azar KM, Bennett GG, Peterson ED, Zheng Y, Turan TN. Current science on consumer use of mobile health for cardiovascular disease prevention a scientific statement from the American Heart Association. Circulation. 2015;132:1157–1213. doi: 10.1161/CIR.0000000000000232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carpenter V, Colwell B. Cancer knowledge, self-efficacy, and cancer screening behaviors among Mexican-American women. Journal of Cancer Education. 1995;10:217–222. doi: 10.1080/08858199509528377. [DOI] [PubMed] [Google Scholar]
- Center for Disease Control and Prevention. State Indicator Report on Fruits and Vegetables 2013. Division of Nutrition, Physical Activity and Obesity. 2013 Retrieved from http://www.cdc.gov/nutrition/downloads/State-Indicator-Report-Fruits-Vegetables-2013.pdf.
- Center for Disease Control. Health, United States, 2014; with Special Feature on Adults Aged 55-64. 2014 Retrieved from http://www.cdc.gov/nchs/data/hus/hus14.pdf#059.
- Chavez LR, Hubbell FA, Mishra SI, Valdez RB. The influence of fatalism on self-reported use of Papanicolaou smears. American Journal of Preventive Medicine. 1997;13:418–424. [PubMed] [Google Scholar]
- Chuang SS, Tamis-LeMonda CS, editors. Gender roles in immigrant families. New York, NY: Springer; 2013. [Google Scholar]
- Colón I. Race, belief in destiny, and seat belt usage: a pilot study. American Journal of Public Health. 1992;82:875–877. doi: 10.2105/ajph.82.6.875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corbin J, Strauss A. Basics of qualitative research: Techniques and procedures for developing grounded theory. London: Sage Publications; 1998. [Google Scholar]
- de los Monteros KE. Encyclopedia of Behavioral Medicine. Springer; New York: 2013. Fatalism; pp. 791–793. [Google Scholar]
- Dyson PA, Anthony D, Fenton B, Stevens DE, Champagne B, Li LM, Community Interventions for Health (CIH) collaboration Successful up-scaled population interventions to reduce risk factors for non-communicable disease in adults: Results from the International Community Interventions for Health (CIH) project in China, India and Mexico. PloS one. 2015;10:1–13. doi: 10.1371/journal.pone.0120941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher L, Chesla CA, Skaff MM, Gillis C, Mullan JT, Bartz RJ, Lutz CP. The family and disease management in Hispanic and European-American patients with type 2 diabetes. Diabetes Care. 2000;23:267–272. doi: 10.2337/diacare.23.3.267. [DOI] [PubMed] [Google Scholar]
- Flórez KR, Aguirre AN, Viladrich A, Cespedes A, De La Cruz AA, Abraido-Lanza AF. Fatalism or destiny? A qualitative study and interpretative framework on Dominican women's breast cancer beliefs. Journal of Immigrant & Minority Health. 2009;11:291–301. doi: 10.1007/s10903-008-9118-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Free C, Knight R, Robertson S, Whittaker R, Edwards P, Zhou W, Roberts I. A randomised controlled trial of mobile (cell) phone text messaging smoking cessation support: txt2stop. Lancet. 2011;378:49–55. doi: 10.1016/S0140-6736(11)60701-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fryar CD, Ervin RB. Caloric intake from fast food among adults: United States, 2007–2010. NCHS data brief, (114) 2013:1–8. Retrieved from http://www.cdc.gov/nchs/data/databriefs/db114.pdf. [PubMed]
- Gaines SO, Jr, Barajas L, Hicks D, Lyde M, Takahashi Y, Yum N, Page MS. Links between race/ethniciy and cultural values as mediated by racial/ethnic identity and moderated by gender. Journal of Personality & Social Psychology. 1997;72:1460–1476. doi: 10.1037//0022-3514.72.6.1460. [DOI] [PubMed] [Google Scholar]
- Glasgow RE, Klesges LM, Dzewaltowski DA, Bull SS, Eastabrooks P. The future of health behavior change in research: What is needed to improve translation of research into health promotion practice? Annals of Behavioral Medicine. 2004;27:3–12. doi: 10.1207/s15324796abm2701_2. [DOI] [PubMed] [Google Scholar]
- Hu FB. Overweight and obesity in women: Health risks and consequences. Journal of Women's Health. 2003;12:163–172. doi: 10.1089/154099903321576565. doi: http://dx.doi.org/10.1089/154099903321576565. [DOI] [PubMed] [Google Scholar]
- Ko LK, Reuland D, Jolles M, Clay R, Pignone M. Cultural and linguistic adaptation of a multimedia colorectal cancer screening decision aid for Spanish-speaking Latinos. Journal of Health Communication. 2014;19:192–209. doi: 10.1080/10810730.2013.811325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kagawa-Singer M, Dressler WW, George SM, Elwood WN. The cultural framework for health: An integrative approach for research and program design and evaluation. Bethesda, MD: National Institutes of Health; 2015. Available at: http://obssr.od.nih.gov/pdf/cultural_framework_for_health.pdf https://obssr-archive.od.nih.gov/pdf/cultural_framework_for_health.pdf. [Google Scholar]
- Katiria Perez G, Cruess D. The impact of familism on physical and mental health among Hispanics in the United States. Health Psychology Review. 2014;8:95–127. doi: 10.1080/17437199.2011.569936. [DOI] [PubMed] [Google Scholar]
- Krogstad JM, Stepler R, Lopez MH. English proficiency on the rise among Latinos: U.S born driving language changes. Pew Research Center; Washington, D.C.: 2015. [Google Scholar]
- Kumar S, Nilsen WJ, Abernethy A, Atienza A, Patrick K, Pavel M, Hedeker D. Mobile health technology evaluation: The mHealth evidence workshop. American Journal of Preventive Medicine. 2013;45:228–236. doi: 10.1016/j.amepre.2013.03.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kushner RF, Choi SW. Prevalence of unhealthy lifestyle patterns among overweight and obese adults. Obesity. 2010;18:1160–1167. doi: 10.1038/oby.2009.376. [DOI] [PubMed] [Google Scholar]
- Lee S, Elkasabi M, Streja L. Increasing cell phone usage among Hispanics: Implications for telephone surveys. American Journal of Public Health. 2012;102:19–24. doi: 10.2105/AJPH.2012.300681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mason MJ, Benotsch E, Way T, Kim H, Snipes D. Text messaging to increase readiness to change alcohol use in college students. Journal of Primary Prevention. 2014;35:47–52. doi: 10.1007/s10935-013-0329-9. [DOI] [PubMed] [Google Scholar]
- Paxton AE, Strycker LA, Toobert DJ, Ammerman AS, Glasgow RE. Starting the conversation: Performance of a brief dietary assessment and intervention tool for health professionals. American Journal of Preventive Medicine. 2011;40:67–71. doi: 10.1016/j.amepre.2010.10.009. [DOI] [PubMed] [Google Scholar]
- Pottie K, Hadi A, Chen J, Welch V, Hawthorne K. Realist review to understand the efficacy of culturally appropriate diabetes education programmes. Diabetic Medicine. 2013;30:1017–1025. doi: 10.1111/dme.12188. [DOI] [PubMed] [Google Scholar]
- Quinn GP, Hauser K, Bell-Ellison BA, Rodriguez NY, Frias JL. Promoting pre-conceptional use of folic acid to Hispanic women: A social marketing approach. Maternal and Child Health Journal. 2006;10:403–412. doi: 10.1007/s10995-006-0074-2. [DOI] [PubMed] [Google Scholar]
- Ramirez AS. Effects of ethnic targeting on the perceived effectiveness of cancer prevention messages among Latinas and non-Latina White women. Journal of Health Communication. 2013;18:1256–1273. doi: 10.1080/10810730.2013.778362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rennie L, Johnson L, Jebb SA. Behavioural determinants of obesity. Best Practice & Research Clinical Endocrinology & Metabolism. 2005;19:343–358. doi: 10.1016/j.beem.2005.04.003. [DOI] [PubMed] [Google Scholar]
- Sampsel S, May J. Assessment and management of obesity and comorbid conditions. Disease Management. 2007;10:252–265. doi: 10.1089/dis.2007.105712. [DOI] [PubMed] [Google Scholar]
- Shen L, Condit C, Wright L. The psychometric property and validation of a fatalism scale. Psychology & Health. 2009;24:597–613. doi: 10.1080/08870440801902535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simmons VN, Cruz LM, Brandon TH, Quinn GP. Translation and adaptation of smoking relapse-prevention materials for pregnant and postpartum Hispanic women. Journal of Health Communication. 2010;16:90–107. doi: 10.1080/10810730.2010.529492. [DOI] [PubMed] [Google Scholar]
- Solomon FM, Eberl-Lefko AC, Michaels M, Macario E, Tesauro G, Rowland JH. Development of a linguistically and culturally appropriate booklet for Latino cancer survivors: Lessons learned. Health Promotion Practice. 2005;6:405–413. doi: 10.1177/1524839905278447. [DOI] [PubMed] [Google Scholar]
- Song M, Choi J, Yang JJ, Sung H, Lee Y, Lee H, Kang D. Obesity at adolescence and gastric cancer risk. Cancer Causes & Control. 2015;26:247–256. doi: 10.1007/s10552-014-0506-z. Retrieved from http://search.proquest.com/docview/1671634877?accountid=14515. [DOI] [PubMed] [Google Scholar]
- The NS. The development of young adult obesity and its role on diabetes. 2011 (Order No. AAI3418750). Available from PsycINFO. (868227337; 2011-99060-325). Retrieved from http://search.proquest.com/docview/868227337?accountid=14515.
- Umaña-Taylor AJ, Bámaca MY. Conducting focus groups with Latino populations: Lessons from the field. Family Relations. 2004;53:261–272. [Google Scholar]
- United States Census Bureau. Race and Hispanic or Latino Origin: 2010 2010 Census Summary File 1. 2010 Retrieved from http://factfinder.census.gov/faces/tableservices/jsf/pages/productview.xhtml?src=CF.
- United States Census Bureau. State median family income by family size. 2010 Retrieved from http://www.census.gov/hhes/www/income/statemedfaminc.html.
- United States Census Bureau. U.S. Census Bureau Projections Show a Slower Growing, Older, More Diverse Nation a Half Century from Now. 2013 Retrieved from http://www.census.gov/newsroom/releases/archives/population/cb12-243.html.
- United States Department of Agriculture. ChooseMyPlate.gov. 2016 Retrieved from http://www.choosemyplate.gov/printpages/MyPlateFoodGroups/Fruits/food-groups.fruits-amount.pdf.
- Whittaker R, Borland R, Bullen C, Lin RB, McRobbie H, Rodgers A. Mobile phone-based interventions for smoking cessation. Cochrane Database of Systematic Reviews. 2009;(4) doi: 10.1002/14651858.CD006611.pub2. [DOI] [PubMed] [Google Scholar]
- Williams GC, Ryan RM, Deci EL. Health-Care, Self-Determination Theory Questionnaire Packet. 2015 Retrieved on March 1, 2015 from: http://www.selfdeterminationtheory.org/health-care-self-determination-theory/