

Abstract
The present study investigated the associations between multigenerational continuity in family conflict and current psychopathology symptoms and social impairment experienced by parents and adolescents. We sampled 246 families from a multigenerational, high-risk, longitudinal study of parents (G1s) and their children (G2s), followed from adolescence (age M = 14.3, 57% female, 71% Caucasian, 26% Hispanic/Latino) to adulthood as well as the children of G2 targets (G3s; age M = 12.1 years, 47% female, 51% Caucasian 33% Hispanic/Latino). Family conflict was measured by composite latent variables incorporating mother, father, and adolescent reports in G1–G2 families and incorporating G2 target, G2 target’s spouse, and G3 adolescent report in G2–G3 families. Indicators of G2 and G3 impairment including psychopathology symptoms (e.g., internalizing, externalizing, and substance use symptoms) and social role impairment (e.g., marital satisfaction, parenting behavior) were predicted from G1–G2 family conflict, G2–G3 family conflict, and the interaction between G1–G2 and G2–G3 family conflict. Results indicate that G1–G2 family conflict uniquely predicted indicators of G2 and G3 psychopathology, and G2 social impairment, even after controlling for more temporally proximal G2–G3 family conflict. Results further indicate that for G2 externalizing, internalizing, and marital functioning outcomes, high G2–G3 family conflict was associated with highest G2 impairment when G1–G2 family conflict was also high. It appears for many G2 outcomes, the interactive effects of multigenerational conflict are associated with greater risk for impairment.
Keywords: family conflict, multigenerational, marital, intergenerational, psychopathology
Numerous longitudinal investigations demonstrate that high conflict in families predicts elevations in multiple indicators of psychopathology, including problematic symptoms (e.g., greater internalizing, externalizing, and substance use problems; Jouriles, Rosenfield, McDonald & Mueller, 2014; Formoso, Gonzales, & Aiken, 2000) and social impairment (Cummings & Schatz, 2012) across the life course. Recently, researchers have found that family conflict can persist across generations within families such that high family conflict in homes comprised of G1 (or first generation at baseline) parents and their G2 children prospectively predicts higher conflict 15+ years later in homes comprised of G2 parents and their G3 children (Rothenberg, Hussong, & Chassin, 2016). Multigenerational family conflict (i.e., growing up in a high conflict home as a child and then being in a high conflict home as an adult) may predict greater dysfunction than conflict that occurs within a single generation. Indeed, conflict in G2–G3 homes may be more intense and frequent if G2s have a history of conflict in G1–G2 families, consequently leading to greater G2 and G3 maladaptation. However, the unique and interactive effects of G1–G2 and G2–G3 family conflict on G2 and G3 psychopathology have never been studied. Doing so could add to our understanding of family psychology by evaluating the predictive utility of assessing conflict in one’s family of origin, by identifying which G2–G3 families are most likely to develop psychopathology (i.e., those with a history of high conflict in both generations) and by characterizing the scope of intervention services needed (i.e., identifying components of the family system needing remediation). Addressing this gap in the literature, the present study uses a multigenerational longitudinal sample to test whether the unique and interactive effects of family conflict in multiple generations area associated with greater subsequent G2 and G3 problematic symptoms and impairments in functioning.
Family Conflict and Individual Functioning
In accordance with other investigators (Cummings, Koss, & Davies, 2015; Horwitz et al., 2011) we believe that family conflict cannot be inferred from assessments of individual dyads only but must also be assessed as a broader, family-level construct. Therefore, the present investigation defines family conflict as the experience of aggression, criticism, anger, or arguments within the overall family climate (i.e, across multiple relationships in the family). Single generation studies demonstrate that family conflict is associated with numerous problematic outcomes that span internalizing, externalizing, and substance use symptom clusters and persist from adolescence into adulthood (Cummings & Schatz, 2012). For instance, multiple longitudinal studies demonstrate that high family conflict prospectively predicts elevations in depression and anxiety (Cummings & Schatz, 2012; Jaycox & Repetti, 1993), aggressive and antisocial behavior (e.g., Kimonis, Frick, & McMahon, 2014), and substance misuse (Best et al., 2014) in childhood (Kouros & Garber, 2014) and adulthood (Herrenkohl, Lee, Kosterman & Hawkins, 2012). Consistent with a potential causal role of family conflict, empirically-supported interventions targeting family conflict have reduced externalizing (McMahon & Forehand, 2003), internalizing (Chase & Eyberg, 2008), and substance use (Best et al., 2014) symptoms in children.
Family conflict is also linked with numerous impairments in social role functioning in adulthood (e.g., marital and parental functioning; Rothenberg et al., 2016). For instance, in single generation studies high family conflict portends marital dissatisfaction (Cummings & Schatz, 2012), discord (Horwitz et al, 2011), and stress (Cummings & Schatz, 2012) as well as a wide range of maladaptive parenting behaviors (Horwtiz et al, 2011; El-Sheikh & Erath, 2011). In summary, single generation longitudinal studies indicate that family conflict predicts a variety of problematic symptoms and social impairments in both parents and children (even as they mature into adulthood).
Intriguingly, an emerging body of literature demonstrates that deleterious aspects of the family environment, including maladaptive family climates (Belsky, Jaffee, Silgo, Woodward, & Silva, 2005), lack of parental warmth (Schofield, Conger, & Neppl, 2014), and parental hostility (Conger, Neppl, Kim, & Scaramella, 2003), show modest consistency across multiple generations within families. This includes our own recent work in which family conflict demonstrated moderate continuity across two family generations (Rothenberg et al., 2016). Although, a vast and well-established body of work identifies single-generation family conflict as a risk factor for the development and persistence of psychopathology and social impairments across the life span, the added risk of experiencing high conflict in one’s family of origin, in addition to in one’s current family, has not yet been examined with respect to child and adult symptoms and impairment.
Two mechanisms may explain why G2s and G3s from multigenerational high-conflict families could experience increased risk for impairment. First, growing up in a high-conflict family of origin may lead to persistent experiences of high conflict when interacting with such a family into adulthood (Cowan & Cowan, 2012). If G1–G2 family conflict experienced during G2s’ adolescence continued into G2’s adulthood, families with greater G2–G3 family conflict may experience family conflict in both the immediate family (G2–G3) and the extended family (G1–G2) simultaneously. Greater conflict in the extended family may undermine the extent to which G2–G3 families receive social support from the extended family for coping with stress and conflict in the immediate family environment and overwhelm coping resources available to the immediate family (Cowan & Cowan, 2012). Thus, families with greater G1–G2 and G2–G3 conflict may not only have the stress of conflict in their immediate families but also fewer resources for dealing with that stress. Consequent deleterious effects for G2 marital and parenting behaviors, and G2 and G3 mental health, would be expected to follow (Cummings & Schatz, 2012).
Second, even if G1–G2 family conflict does not continue into G2’s adulthood, multigenerational family conflict may still signal risk for G2 and G3 impairment due to the accumulation of developmental deficits in interpersonal and coping skills in G2s. High conflict G1–G2 families may undermine the normative development of these social competencies. G2’s whose skill deficits continue into adulthood may then be at risk for contributing to greater G2–G3 family conflict through their own conflictual family interactions, potential to select partners with similar family histories (via assortative mating, Rothenberg et al., 2016), and impairments in role functioning (as marital partners or parents). When this occurs, a multigenerational pattern of family conflict will result and this pattern may signal developmentally accumulated risks in G2 social functioning that exceeds that of G2’s without a multigenerational history of family conflict. In turn, multigenerational family conflict may relate to increased risk in G2s for psychopathology and role impairment and so may in turn impact their children.
The current study expands the multigenerational family conflict literature by investigating whether experiencing high conflict in both the G1–G2 family and G2–G3 family is associated with more maladaptive G2 and G3 outcomes. We consider these effects by highlighting two specific associations in our investigation. First, we predict current G2 and G3 impairment from models including both distal G1–G2 family conflict (when G2s were adolescents) and proximal G2–G3 family conflict (when G2s are adults and G3s are adolescents) to determine the unique effects of G1–G2 family conflict after controlling for G2–G3 family conflict. In so doing, we evaluate whether it is useful to assess G1–G2 family conflict history to predict current G2 or G3 impairment even when current G2–G3 family conflict is already known. Second, to examine our hypothesis about the synergistic combined effects of G1–G2 and G2–G3 family conflict, we examine whether G1–G2 and G2–G3 family conflict interact to predict G2 and G3 impairment. This interaction term allows us to compare G2 and G3 outcomes across families who exhibit high conflict in both the G1–G2 and G2–G3 family environments in comparison to families who exhibit high conflict in only the G2–G3 family environment. We expect that families who experience conflict in both generations will demonstrate greater G2 and G3 dysfunction than families who only have conflict in the proximal G2–G3 family environment. Taken together, these comparisons examine whether knowing about patterns of family conflict that recur across generations adds value in predicting G2 and G3 outcomes above and beyond knowing about conflict in the proximal G2–G3 family environment.
The Current Study
Family conflict has been repeatedly demonstrated to be a risk factor that predicts a range of problematic symptoms and social impairments in both adolescence and adulthood. Family conflict has also been characterized as a multigenerational phenomenon (e.g., Rothenberg et al., 2016), yet no studies have investigated whether multigenerational high family contributes to increased risk of psychopathology beyond family conflict experienced in a single generation. In beginning to answer these questions, the current study had two objectives. First, we tested whether distal G1–G2 family conflict measured in G2s’ adolescence significantly predicted high adult G2 and adolescent G3 externalizing, internalizing and substance use symptoms, and G2 social functioning impairments, even after accounting for more temporally proximal G2–G3 family conflict. Second, we tested whether G1–G2 family conflict and G2–G3 family conflict interacted to predict G2 and G3 symptoms and social impairment. Specifically, we predicted that G2s and G3s from families who exhibit higher conflict in both the G1–G2 and G2–G3 family environments will experience the greatest impairments.
Methods
Data from the Adolescent & Family Development Project (AFDP; Chassin, Pitts, DeLucia, & Todd, 1999) were used for this study. AFDP is an ongoing longitudinal study of children of alcoholic parents (COAs) and matched controls assessed from adolescence into adulthood. AFDP used a multi-generational design involving assessments of parents (G1s), target adolescents who were followed over time (G2s), and the children of these targets (G3s). AFDP presently consists of 6 waves of data collected annually for waves 1 through 3 (where data were collected on G1s and G2s) and then at 5 year-intervals through wave 6 (where data were collected on G2s, G2 spouses, and G3s).
Participants
At wave 1, the AFDP sample consisted of 246 adolescents with at least one alcoholic parent and 208 matched adolescents with no biological or custodial alcoholic parent for a total of 454 G2 adolescents and their parents in G1–G2 families. COA families were recruited using court arrest records for driving under the influence, health maintenance organization wellness questionnaires and community telephone screenings (see Chassin et al., 1999). COA families had to meet the following criteria: parents reported being either Hispanic or non-Hispanic Caucasian, Arizona residency, a child aged 10.5–15.5 years at wave 1, English-speaking, and parents and children with no cognitive limitations that would preclude interview. Further, direct interview data had to confirm that at least one parent met Diagnostic and Statistical Manual for Mental Disorders, third edition (DSM-III) criteria for alcohol abuse or dependence.
Matched controls were recruited using telephone interviews. Controls were screened to match COA participants in ethnicity, family structure, target child’s age and gender, and socioeconomic status. Direct parent interview data were used to confirm that neither biological nor custodial parents of controls met DSM-III criteria. Attrition biases were minimal as 409 of the original 454 families were retained at wave 6 (90.1% of original sample). To be included in the current analysis, G2’s needed to have at least one child by wave 6 (N = 273 of 409 interviewed at wave 6) and complete data on the family conflict measure at waves 1 and 6 (N = 246 of 273 G2s with children, with 27 missing data because they contacted their child less than once a week). Therefore, our final sample consisted of 246 G2s. Notably, 7.69% of G1 mothers (N = 18) and 1.05% of G1 fathers (N = 2) reported being separated or divorced at wave 1, and 23.34% of G2s (N = 56) reported being unmarried, single, separated, or divorced at wave 6.
In wave 6 of data collection, only G2 targets were required to complete interviews. However G2 partners and any G3s who were 8 years old or older were also invited to complete interviews if they were available at the time the G2 was interviewed. Thus, though G2 targets reported on all study measures, G2 reports of family conflict were supplemented by reports from the G2 parenting partner (N = 102) and the oldest G3 child (N = 123) when available to create a single G2–G3 family conflict variable (see Measures section for further detail). Only the oldest G3 was included in study analyses to provide comparability in measurement across families with different numbers of children. Importantly, no significant differences on any study outcome variables were observed when comparing families with and without missingness on family conflict as reported by G2 parenting partners (F(23, 39) = 1.01, p = .48) and G3 children (F(23, 40) = 1.23, p = .28). Missing data was addressed using full information maximum likelihood procedures such that all 246 G2–G3 families were retained in study analyses (see Data Analytic Strategy). Demographic characteristics of G2s, G2 partners, and G3s can be found in Table 1.
Table 1.
Demographic Characteristics of G2s, G2 Parenting Partners, and G3s
| Demographic Variable | G2 % or M (SD) (N= 246) |
G2 Partner % or M (SD) (N= 102) |
G3 % or M (SD) (N = 123) |
|---|---|---|---|
| Gender | 57% female | 43% female | 47% female |
| Ethnicity | |||
| Caucasian | 71% | 61% | 51% |
| Hispanic | 26% | 33% | 33% |
| Other | 3% | 6% | 12% |
| Age (Wave 6) | 31.8 (1.76) | 33.2 (1.70) | 12.14 (2.39) |
| Age (Wave 1) | 13.4 (1.40) | – | – |
| Highest Level of Education Obtained in G2–G3 Family | |||
| GED | 30% | – | – |
| Completed Some College | 31% | – | – |
| Associates, Bachelor’s, or beyond | 32% | – | – |
| G2 Child of Alcoholic (COA) Status | 53% COA | – | – |
Procedure
At each wave, data were primarily collected via in-person computer-assisted interviews (Chassin et al., 1999). Family members were typically interviewed in separate rooms to avoid contamination and to increase privacy. In waves 1–3 of data collection, at least one G1 caregiver (Mage = 39.60, SD = 5.67) and one G2 adolescent completed interviews. In wave 6 of data collection, G2 targets and available G2 spouses and G3 children ages 8 and older completed interviews. Importantly, adolescents in G1–G2 families (Mage = 13.39, SD = 1.40) and G2–G3 families (Mage = 12.14, SD = 2.39) were similar in age. This unique design feature is often recommended in the multigenerational literature because it captures multigenerational processes at similar points in family development (e.g., Conger, Belsky, & Capaldi, 2009), but is rarely actually used in empirical work for practical reasons. Interviews typically lasted from 1 to 3 hours and participants were paid up to $70 per wave. Study procedures were approved by the Arizona State University Institutional Review Board (Protocol #: 0506000017; Title of Study: Adult and Family Development Project)
Measures
Demographic variables
Because prediction of G2 and G3 symptoms and impairment were the focus of analyses, several G2 and G3 demographic variables were controlled. Specifically, G2 marital status and socioeconomic status, as well as G2 and G3 gender, age, and ethnicity were controlled for in the present analyses. G2s at wave 6 reported their marital status (i.e., married, separated, divorced, widowed, never married). Additionally, G2s and G3s self-reported their age, gender and ethnicity at wave 6. G2–G3 family wave 6 socioeconomic status was indexed by the highest education level obtained by either parent in the G2–G3 family.
G1 psychopathology
G1 mother and G1 father antisocial behavior, affective disorders and alcoholism were measured via self-reported lifetime DSM-III diagnoses of antisocial personality disorder, major depressive disorder, dysthymia and alcohol abuse or dependence. These diagnoses were obtained using a computerized version of the DIS interview (Version 3; Robins, Helzer, Ratcliff, & Seyfried, 1982). Although all reports of antisocial personality disorder and affective disorders were based solely on self-report by mother or father and missing otherwise, alcoholism diagnoses were based on self-report as well as spousal report for non-participating parents. In current analyses, family-level diagnoses were dichotomized as either present (at least one G1 parent meet lifetime criteria) or absent.
Family conflict
Family conflict was measured using adolescent and adult reports on the same 5-item family conflict subscale derived from Bloom’s Family Processes Scale, which has demonstrated adequate reliability (α = .76 to α = .85) and validity in previous studies (Bloom, 1985). Participants rated the extent to which they agreed that a statement (e.g. “we fought a lot in our family”, “family members sometimes go so angry they threw things”) reflected their family life in the past 3 months using a five-point response scale ranging from 1 = strongly agree to 5 = strongly disagree. G1 mothers, G1 fathers, and adolescent G2s completed the family conflict scale at wave 2 in reference to G1–G2 families. G2 targets, G2 partners and the oldest G3 child completed the family conflict subscale at wave 6 in reference to G2–G3 families. Scale score means and internal reliability estimates were as follows: wave 1 G1 father-reports (α = .69, M = 2.70, SD = 0.76), G1 mother-reports (α = .65, M = 2.61, SD = 0.78) and G2 reports (α = .73, M = 2.64, SD = 0.79); and wave 6 G2 reports (α = .70, M = 2.19, SD = 0.72), G2 partner reports (α = .67, M = 2.50, SD = 0.69), and G3 reports (α = .65, M = 2.53, SD = 0.75). Each of these scale mean scores fell between the “Disagree” and “Neither Agree nor Disagree” options, meaning that, on average, reporters in both G1–G2 and G2–G3 families rated their conflict as moderate to slightly low. Reporter responses at the item level were combined to estimate both G1–G2 family conflict and G2–G3 family conflict latent variables.
As reported in Rothenberg et al. (2016), these G1–G2 family conflict and G2–G3 family conflict latent variables were created in a several step process. Initially, parceling procedures (Kishton & Widaman, 1994) were used to integrate G1 mother, G1 father and G2 target reports of G1–G2 family conflict as well as G2 target, G2 partner and all available G3 child reports of G2–G3 family conflict. For this step, family members’ responses to the family conflict scale were averaged at the item level for both G1–G2 and G2–G3 families (i.e., G1 mother, G1 father and G2 adolescent responses to item 1 of the family conflict scale were averaged to create a single indicator of G1–G2 family conflict for item 1). Then, maximum likelihood confirmatory factor analyses using Mplus Version 7 (Muthen & Muthen, 2015) were conducted to estimate latent variables representing underlying conflict in the family environment. Skewness and kurtosis estimates for all indicators fell in acceptable ranges (skew < 2.0, kurtosis < 3.0), suggesting no violation of the assumption of normally distributed indicators. Additionally, no problematic heteroscedasticity of residuals in indicators was observed. All indicators loaded satisfactorily on their respective latent factors (λ > .45 for all indicators), and G1–G2 and G2–G3 family conflict latent variables were found to demonstrate strong invariance across both genders (Rothenberg et al., 2016). Fit indices showed that that both the G1–G2 family conflict (χ2 (3) = 4.11, p = 0.25, CFI = 0.99, TLI = 0.99, RMSEA = 0.04, SRMR =0.02), and G2–G3 family conflict (χ2 (3) = 2.18, p = 0.53, CFI = 1.00, TLI = 1.00, RMSEA = 0.00, SRMR = 0.01) latent variables fit the data well, indicating that it was appropriate to estimate latent variables for both G1–G2 family conflict and G2–G3 family conflict.
G2 & G3 externalizing behavior
G2 and G3 externalizing behaviors at wave 6 was measured using 12 items from the aggression and delinquent behavior subscales of the parent report version of the Child Behavior Checklist (CBCL; Achenbach & Edelbrock, 1981). G2 adults were asked to rate these items in relation to their own and their G3 adolescents’ behaviors on a 1 = “almost always” to 5 = “almost never” scale; items were averaged to create summary scores such that higher scores indicated greater externalizing behavior. Summary scores for G2 self-reported externalizing behavior at wave 6 (α = .74), and G2 report of G3 externalizing behavior at wave 6 (α = .92) were generated such that higher scores indicated greater externalizing behavior.
G2 & G3 internalizing behavior
G2 behaviors at wave 6 were measured using 10 items from the self-report version of the CBCL (Achenbach & Edelbrock, 1981) with a response scale from 1 = “almost always” to 5 = “almost never”. Items were averaged to create summary scores for G2 (α = .86) self-reported internalizing behavior at wave 6, where higher scores indicated greater internalizing behavior. G2 parent-report of G3 internalizing behavior at wave 6 was measured using 19 items which comprised the anxious/depressed, withdrawn/depressed and somatic complaints subscales from the parent-reported version of the CBCL. G2 parents reported on G3 behavior using the same 5-point response scale as used for self-report, and items were averaged to generate a summary score (α = .80) where higher scores indicated greater internalizing behavior.
G2 and G3 past year problematic alcohol & drug use
The same 19 items were used to assess past year alcohol consequences and dependence symptoms in G2s and G3s at wave 6 (Lee, Chassin, & MacKinnon, 2015). Participants were asked whether they had experienced each consequence or dependence symptom in the past year (1 = “no”, 2 = “yes”). Items were then averaged to create past year problematic G2 (α = .91) and G3 (α = .83) alcohol use and G2 (α = .95) and G3 (α = .83) drug use scores representing the total percentage of items endorsed.
G2 and G3 highest lifetime alcohol use
At wave 6, G2 and G3 participants answered one item asking about the most they have ever used alcohol a 7-point response scale ranging from 0 = “not at all” to 7 = “every day”.
G2 social role impairment
Three indices of social role impairment focused on G2 parenting at wave 6. G2 self-reported support of G3s was measured using a 7 item scale adapted from the Network of Relationships Inventory (Furman & Buhrmester, 1985) with a 5-point response scale ranging from “little or none” to “the most possible” (α = .85). G2 parenting consistency was measured using ten items from the Children’s Report of Parental Behavior Inventory (Schaefer, 1965) that were measured with a 5-point response scale ranging from “strongly agree” to “strongly disagree” (α = .89). G2s’ parent monitoring was measured using a 5-item monitoring scale (Lamborn, Mounts, Steinberg & Dornbusch, 1991) that has a 5-point response scale ranging from “didn’t know at all” to “knew all the time” (α = .89). For all three scales, items were averaged and reverse-scored to create a summary score where higher scores indicated less support of G3s, less parenting consistency and less parental monitoring.
Three indices of social role impairment focused on G2’s marital relationship at wave 6. G2 perceptions of social support were measured by asking G2s about their perceptions of their romantic partners’ provision of social support on a six item (e.g., “Your partner treats you like you are admired and respected”) scale adapted from the Network of Relationships Inventory (Furman & Buhrmester, 1985). Responses could range from 1 = “little or none” to 5 = “the most possible support” (α = .99). G2 marital satisfaction was measured by three items created by project staff (e.g., “How satisfied are you in your relationship within the past year?”). Responses ranged on a 1 = “very dissatisfied” to 5 = “very satisfied” scale (α = .99). G2s marital stress was measured with three items (e.g., “How stressful is your marriage/relationship?”) on a 1 = “not at all” to 5 = “a great deal” scale (α = .99; Todd, Chassin, Presson & Sherman, 1996). For all three scales, items were averaged and, where necessary, reverse-scored to create summary scores where higher scores indicated less social support, less marital satisfaction, and more marital stress.
Data Analytic Strategy
Data analysis proceeded using Full-Information Maximum Likelihood estimation in Mplus (Muthen & Muthen, 2015), resulting in the inclusion of all 246 families in study analyses. Notably, we conducted a series of sensitivity analyses wherein only families with observed (i.e., non-missing) data on each variable of interest were included. Study results were not substantively different when only those families with observed data were analyzed.
Hypothesis testing occurred separately for each individual G2 and G3 outcome in an iterative model-building process that proceeded in several steps. First, a given G2 or G3 outcome was regressed on a series of control variables (See Table 2 for associations among controls, G1–G2, and G2–G3 family conflict). These controls included five demographic variables that have been found to predict differences in psychopathology symptoms and social impairment (e.g., Kouros & Garber, 2014), including G2–G3 household socioeconomic status, G2 parent marital status and G2 parent and G3 child age, ethnicity, and gender. Furthermore, measures of parent psychopathology were included among these controls. Specifically, each specific G2 or G3 outcome was regressed on the related G1 or G2 control. Thus, G2 measures of externalizing, internalizing, and substance use symptoms were predicted from G1 antisocial personality disorder, major depression/dysthymia, and alcoholism diagnoses, respectively. Additionally, G3 measures of externalizing, internalizing, and substance use symptoms were predicted from the measures of G2 externalizing, internalizing, and substance use symptoms, respectively. Then, these baseline models predicting G2 and G3 outcomes from demographics and parent psychopathology were estimated, and variables that were not significant at p < .05 were trimmed from further analyses. Our purpose in trimming these models was to retain pertinent demographic and parent psychopathology covariates for further analyses without over-controlling for such covariates, and thus partialling out meaningful variance that may actually be accounted for by G1–G2 or G2–G3 family conflict.
Table 2.
Correlation Matrix of Key Predictor Variables
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. G1–G2 Family Conflict | 1.00 | |||||||||
| 2. G2–G3 Family Conflict | 0.30* | 1.00 | ||||||||
| 3. G2–G3 Education | −0.20* | 0.11 | 1.00 | |||||||
| 4. G2 Marital Status | 0.19* | 0.10 | 0.02 | 1.00 | ||||||
| 5. G2 Ethnicity | 0.14* | 0.22* | −0.05 | −0.04 | 1.00 | |||||
| 6. G3 Ethnicity | −0.08 | 0.18* | −0.06 | −0.05 | 0.15* | 1.00 | ||||
| 7. G2 Gender | −0.14* | −0.01 | −0.09 | −0.13* | −0.08 | 0.13* | 1.00 | |||
| 8. G3 Gender | −0.33* | −0.22* | 0.20* | −0.05 | 0.24* | 0.08 | −0.05 | 1.00 | ||
| 9. G2 Age | −0.11 | 0.12 | 0.08 | 0.02 | 0.15* | −0.08 | −0.09 | 0.04 | 1.00 | |
| 10. G3 Age | 0.14* | 0.39* | −0.14* | 0.13* | 0.38* | −0.05 | 0.18* | −0.12 | 0.30* | 1.00 |
Note.
p < .05
Next, we entered the G1–G2 and G2–G3 family conflict latent variables into each of the models predicting G2 and G3 outcomes to investigate the extent to which G1–G2 family conflict predicted changes in G2 and G3 outcomes, even after G2–G3 family conflict and significant covariates were controlled for. Then, in a final step, the G1–G2 and G2–G3 family conflict interaction term was entered into the models using the XWITH procedure in Mplus. Significant interactions were probed and plotted in Mplus by examining associations between G2–G3 family conflict and the G2 or G3 outcome of interest at 1 standard deviation above mean, mean, and 1 standard deviation below mean levels of G1–G2 family conflict. All non-categorical predictor and outcome variables were standardized (M = 0, SD =1) to facilitate probing of interactions and ease of interpretation. Importantly, for all models where a significant interaction was reported, omnibus measures of model fit indicated that adding the interaction term significantly improved model fit. Specifically, in all models probing significant interaction terms, AIC & sample-adjusted BIC values were smaller with the addition of the interaction term. These improvements in fit support the argument that G1–G2 and G2–G3 family conflict interact to predict G2 psychopathology symptoms and social impairment. Final models for each G2 and G3 outcome are reported in Tables 3, 4, and 5. Notably, if an interaction was not significant, it was trimmed from the final model to avoid erroneous interpretation of the main effects of G1–G2 and G2–G3 family conflict in the presence of a non-significant interaction.
Table 3.
Regression Analysis Predicting G2 Psychopathology Symptoms from G1–G2 and G2–G3 Family Conflict
| Externalizing Behavior | Internalizing Behavior | Lifetime Drinking | Problem Alcohol Use | Problem Drug Use | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||
| Predictor | B | SE B | B | SE B | B | SE B | B | SE B | B | SE B |
| G1–G2 Family Conflict | 0.31** | 0.12** | 0.19* | 0.08* | 0.06 | 0.08 | 0.10 | 0.08 | 0.04 | 0.05 |
| G2–G3 Family Conflict | 0.51** | 0.08** | 0.33** | 0.08** | 0.10 | 0.08 | 0.21** | 0.08** | 0.16* | 0.06* |
| G1–G2 × G2–G3 Family Conflict Interaction | 0.45** | 0.15** | 0.24* | 0.10* | 0.14* | 0.07* | ||||
| G2–G3 Education | ||||||||||
| G2 Ethnicity | ||||||||||
| G2 Gender | −0.26* | 0.12* | 0.32* | 0.13* | ||||||
| G2 Age | ||||||||||
| G2 Marital Status | ||||||||||
| G2 COA Status | 0.48** | 0.13** | ||||||||
| G1 Psychopathology | ||||||||||
Note. Empty cells depict covariates that were found non-significant in covariate-only baseline models and thus trimmed from final models.
p < .05,
p<.01, bold indicates significant effect at p < .05.
Table 4.
Regression Analysis Predicting G2 Social Role Impairments from G1–G2 and G2–G3 Family Conflict
| Marital Satisfaction | Marital Stress | Romantic Partner Social Support | Parent Support of G3s | Parental Consistency | Parental Monitoring | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Predictor | B | SE B | B | SE B | B | SE B | B | SE B | B | SE B | B | SE B |
| G1–G2 Family Conflict | 0.41** | 0.01** | 0.25** | 0.07** | 0.13 | 0.08 | 0.18* | 0.09* | 0.18** | 0.07** | 0.13 | 0.12 |
| G2–G3 Family Conflict | 0.35** | 0.01** | 0.44** | 0.07** | 0.40** | 0.08** | 0.13 | 0.08 | 0.44** | 0.08** | 0.09 | 0.09 |
| G1–G2 × G2–G3 Family Conflict Interaction | 0.51** | 0.01** | 0.27** | 0.06** | 0.24** | 0.08** | ||||||
| G2–G3 Education | ||||||||||||
| G2 Ethnicity | 0.16** | 0.06** | 0.21** | 0.06** | ||||||||
| G2Gender | 0.01 | 0.01 | −0.17 | 0.11 | ||||||||
| G2 Age | ||||||||||||
| G2 Marital Status | ||||||||||||
| G2 COA Status | 0.00 | 0.01 | 0.36** | 0.12** | ||||||||
Note. Empty cells depict covariates that were found non-significant in covariate-only baseline models and thus trimmed from final models. All G2 outcomes are scored such that higher scores indicate greater impairment.
p < .05,
p<.01, bold indicates significant effect at p < .05.
Table 5.
Regression Analysis Predicting G3 Problematic Symptoms from G1–G2 and G2–G3 Family Conflict
| Externalizing Behavior | Internalizing Behavior | Lifetime Drinking | Problem Alcohol Use | Problem Drug Use | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||
| Predictor | B | SE B | B | SE B | B | SE B | B | SE B | B | SE B |
| G1–G2 Family Conflict | 0.20** | 0.07** | 0.14* | 0.06* | 0.21* | 0.03* | 0.16 | 0.10 | 0.07 | 0.09 |
| G2–G3 Family Conflict | −0.03 | 0.09 | 0.03 | 0.08 | −0.33** | 0.10** | −0.17 | 0.10 | −0.17* | 0.08* |
| G1–G2 × G2–G3 Family Conflict Interaction | ||||||||||
| G2–G3 Education | ||||||||||
| G3 Ethnicity | −0.06* | 0.03* | −0.11** | 0.02** | −0.09** | 0.03** | ||||
| G3Gender | −0.35** | 0.11** | −0.55** | 0.12** | −0.44** | 0.15** | ||||
| G3 Age | 0.12** | 0.03** | 0.25** | 0.05** | 0.11** | 0.03** | 0.19** | 0.05** | ||
| G2 Marital Status | ||||||||||
| G2 Psychopathology | 0.27** | 0.09** | 0.25** | 0.06** | ||||||
Note. Empty cells depict covariates that were found non-significant in covariate-only baseline models and thus trimmed from final models.
p < .05,
p<.01, bold indicates significant effect at p < .05.
Results
G2 Psychopathology Symptoms
Analyses partially supported the hypothesis that distal G1–G2 family conflict would predict current G2 psychopathology symptoms, even after accounting for proximal G2–G3 family conflict (see Table 3 for complete final model results). Specifically, after controlling for proximal G2–G3 family conflict and covariates, distal G1–G2 family conflict predicted current G2 externalizing behavior (B = 0.31, p < .01), and internalizing behavior (B = 0.19, p < .05), but not current G2 problematic alcohol or drug use, or G2 lifetime drinking.
Analyses also partially supported the hypothesis that the highest G2 psychopathology would be associated with high conflict experienced in both G1–G2 and G2–G3 family environments. Specifically, G1–G2 family conflict was found to significantly moderate the effect of G2–G3 family conflict on G2 externalizing (B = 0.45, p < .01) and G2 internalizing (B = 0.24, p < .05) behavior. Probing these significant interactions (Figure 1, top and middle) revealed that, starting at 0.1 standard deviations above the mean of G2–G3 family conflict, higher G2–G3 family conflict was associated with significantly higher G2 externalizing and internalizing symptoms if G1–G2 family conflict was also one standard deviation above average.
Figure 1.
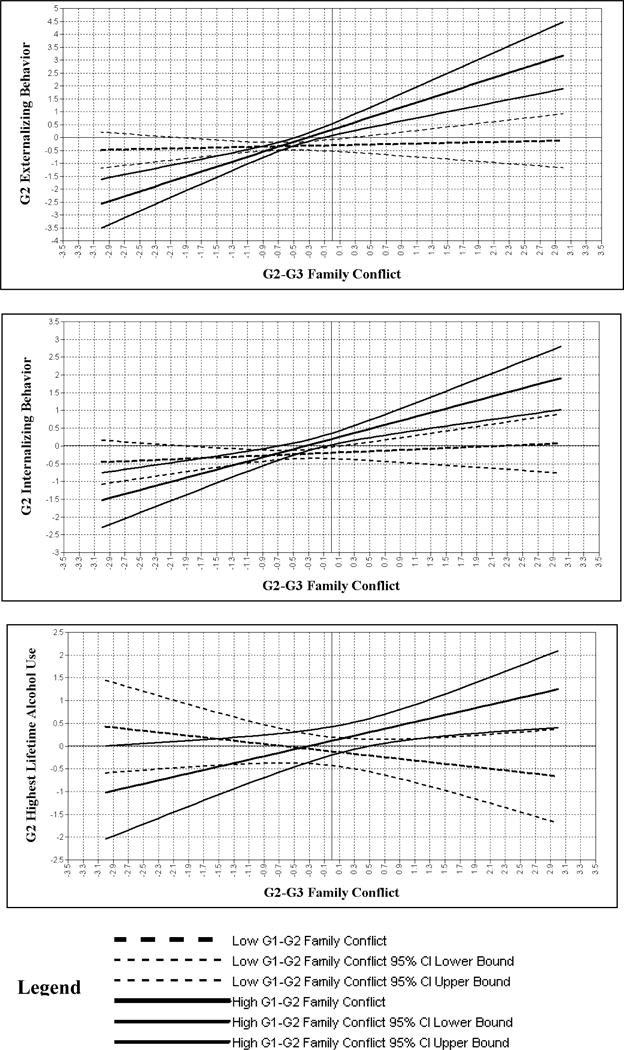
Plots depicting significant interactions between G1–G2 and G2–G3 Family Conflict in predicting G2 psychopathology symptoms. Plots depict association between G2–G3 family conflict and G2 psychopathology outcome at low (−1 SD, dotted lines) and high (+1 SD, solid lines) levels of G1–G2 family conflict, with the exception of G2 Highest Lifetime Alcohol Use, where plots are at +/−2 SD. In each plot, middle dotted and solid lines depict simple slopes. Top and bottom dotted and solid lines depict 95% confidence intervals.
Similarly, G1–G2 family conflict was found to significantly moderate the effect of G2–G3 family conflict on G2 lifetime alcohol use (B = 0.14, p < .05). Probing this significant interaction (Figure 1, bottom) revealed that, starting at 1.5 standard deviations above the mean of G2–G3 family conflict, higher G2–G3 family conflict was associated with significantly higher G2 lifetime alcohol use if G1–G2 family conflict was also two standard deviations above average. Notably, for this interaction, simple slopes were non-significant when probed at 1 standard deviation above and below the mean for G1–G2 family conflict, but significant at +/− 2 standard deviations. Thus, simple slopes at +/−2 standard deviations were plotted. We proceeded in using this plotting strategy because the AFDP study followed G2 COAs and matched controls longitudinally, and is therefore uniquely positioned to investigate interactive processes in predicting such extremely high levels of substance use. Additionally, interaction terms did not significantly predict G2 problematic alcohol or drug use.
G2 Social Role Impairments
Analyses partially supported the hypothesis that distal G1–G2 family conflict would predict current G2 social impairments, even after accounting for proximal G2–G3 family conflict (see Table 4 for complete final model results). Specifically, after controlling for proximal G2–G3 family conflict and covariates, distal G1–G2 family conflict predicted more G2 marital stress (B = 0.25, p < .01), and G2 marital dissatisfaction (B = 0.41, p < .01), and less G2 parental support of G3s (B = 0.18, p < .05), and G2 parental consistency (B = 0.18, p < .01), but did not significantly predict differences in romantic partner social support or parent monitoring.
Analyses also partially supported the hypothesis that the greatest G2 social impairment would be associated with high conflict experienced in both G1–G2 and G2–G3 family environments. Specifically, G1–G2 family conflict was found to significantly moderate the effect of G2–G3 family conflict on G2 marital satisfaction (starting at 0.7 SD below mean G2–G3 family conflict; B = 0.51, p < .01), marital stress (starting at 0.3 SD below mean G2–G3 family conflict; B = 0.27, p < .01) and romantic partner social support (starting at 0.5 SD above mean G2–G3 family conflict; B = 0.24, p < .01). Probing these significant interactions (Figure 2) revealed that higher G2–G3 family conflict was associated with greater marital stress and marital dissatisfaction, and less romantic partner social support, if G1–G2 family conflict was also one standard deviation above average. Notably, interaction terms did not significantly predict G2 parent support of G3s, G2 parent consistency, or G2 parenting monitoring.
Figure 2.
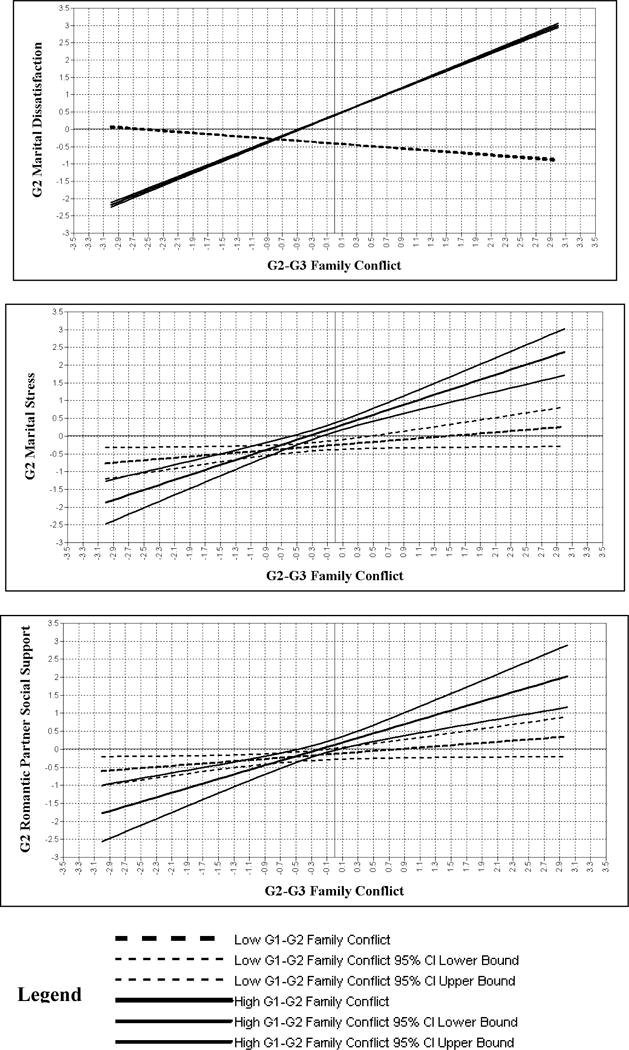
Plots depicting significant interactions between G1–G2 and G2–G3 Family Conflict in predicting G2 social role impairments. Plots depict association between G2–G3 family conflict and G2 social impairment outcome at low (−1 SD, dotted lines) and high (+1 SD, solid lines) levels of G1–G2 family conflict. In each plot, middle dotted and solid lines depict simple slopes. Top and bottom dotted and solid lines depict 95% confidence intervals. For G2 Romantic partner social support, higher scores indicate less support.
G3 Psychopathology Symptoms
Analyses partially supported the hypothesis that distal G1–G2 family conflict would predict current G3 psychopathology symptoms, even after accounting for proximal G2–G3 family conflict (see Table 5 for complete final model results). Specifically, after controlling for proximal G2–G3 family conflict and covariates, distal G1–G2 family conflict predicted current G3 externalizing behavior (B = 0.20, p < .01), internalizing behavior (B = 0.14, p < .05), and lifetime drinking (B = 0.21, p < .05) but not current G3 problematic alcohol or drug use. Analyses did not support the hypothesis that the highest G3 psychopathology would result from high conflict experienced in both G1–G2 and G2–G3 family environments, as no G1–G2 family conflict-by-G2–G3 family conflict interaction terms were found significant.
Additionally, it is important to note that, unexpectedly, higher G2–G3 family conflict predicted lower G3 lifetime drinking and problematic drug use. It appears that these unexpected findings can be accounted for by the strong association between G2–G3 family conflict and G3 age. Specifically, in simple correlation analyses, G2–G3 family conflict was not associated with G3 lifetime drinking (r = −0.06, p = .51), or problematic drug use (r = 0.06, p = .46), nor was it associated with G3 lifetime drinking (B = −0.13, p = .21) or problematic drug use (B = 0.02, p = .89) when both G1–G2 and G2–G3 family conflict, but not covariates, are used to predict these G3 outcomes. While G2–G3 family conflict is correlated with G1–G2 family conflict (r = 0.30, p < .05), it also strongly correlated with G3 age (r = 0.39, p < .05), which is a significant predictor of both G3 lifetime drinking and problematic drug use (see Table 5). Thus, taken together, it seems that these unexpected findings result from the association between G2–G3 family conflict and G3 age, as opposed to colinearity between G1–G2 and G2–G3 family conflict. To maintain consistency across analyses, we present our results when including G3 age as a covariate in Table 5, but we believe that the unexpected findings that higher G2–G3 family conflict predicts lower G3 lifetime drinking and problematic drug use is spurious and the result of overcontrolling for G3 age (Lieberson, 1985).
Discussion
Building on a robust literature that identifies family conflict as a risk factor for a variety of maladaptive outcomes via single generation studies, we investigated whether multigenerational family conflict experienced in consecutive family generations represented additional risk for deleterious outcomes beyond conflict seen within a single family generation. Findings provided some evidence (in 9 of 16 tests) that conflict experienced in one’s family of origin is a unique predictor of current impairment, as higher G1–G2 family conflict predicted higher G3 lifetime alcohol use, greater G2 and G3 internalizing and externalizing behavior, greater G2 marital dissatisfaction and marital stress, less G2 parent support of G3s, and less G2 parental consistency even after controlling for current G2–G3 family conflict. Moreover, findings partially support (in 6 of 11 tests) the hypothesis that G2s from families who exhibit high conflict in both a G2’s family of origin and a G2’s adult family of destination experience the greatest impairments. Specifically, high G2–G3 family conflict was associated with higher G2 externalizing behavior, internalizing behavior, lifetime drinking, marital stress, and marital dissatisfaction, and lower romantic partner support if G1–G2 family conflict was also high. No such interactive effects emerged for G3 outcomes. Importantly, the present study controlled for G1 psychopathology when assessing G2 outcomes, and G2 psychopathology when assessing G3 outcomes, revealing that multigenerational family conflict predicted deleterious G2 and G3 outcomes above and beyond multigenerational continuities in psychopathology.
Importantly, these results support the notion that assessing distal family conflict that occurred in a parent’s childhood family of origin may be just as important as assessing proximal conflict that occurs in a parent’s current adult family of destination when evaluating parent and child impairment. Indeed, study results indicate three out of five indicators of current G2 psychopathology, five out of six indicators of G2 social role impairment, and three out of five indicators of G3 psychopathology were either uniquely predicted by G1–G2 family conflict, or predicted by the interactive effects of G1–G2 and G2–G3 family conflict. Among these results, perhaps the most surprising finding was that greater G3 psychopathology was predicted by the distal G1–G2 family conflict environment, even though G3s were never directly exposed to that conflict environment (because measures of G1–G2 family conflict were taken when G2s were adolescents). Taken as a whole, the current findings indicate that assessment of G1–G2 family conflict could reveal which G2–G3 families are at elevated risk for a range of maladaptive outcomes, even after considering the effects of G2–G3 family conflict.
Additionally, results provide evidence for one process that might explain how conflict in one’s family of origin may predict functional impairments in one’s current family of destination. Specifically, it appears that the synergistic effects of high conflict in both G1–G2 and G2–G3 families leads to greater G2 impairment. Evidence for this process comes from the significant interaction terms that predict G2 psychopathology (e.g., externalizing and internalizing behavior) and social role impairment (e.g., marital satisfaction and stress). These significant interaction terms indicate that high G1–G2 family conflict leads to greater G2 impairment if G2–G3 family conflict is also higher. We suspect these synergistic effects on G2s may emerge due to both to the developmentally accrued interpersonal skill deficits in G2s that exacerbate conflict in the G2–G3 family and to the lack of social support in the extended G2–G3 family to address conflict and reduce overloading of coping resources in the immediate family environment.
Specifically, persistent family conflict may be more likely to result in maladapatation in G2s and G3s because these individuals lack social support and problem solving strategies from a larger family network that would otherwise mitigate the effects of family conflict. For instance, G2s and G3s cannot turn to G1s for support during times of conflict because G1s themselves engaged in high conflict behaviors in G1–G2 homes and are thus not seen as reliable supports (Cummings & Schatz, 2012). Additionally, intergenerational high family conflict could pose increased risk for G2 and G3 impairment because persistent re-experiencing of high conflict with a G2’s family of origin could overwhelm a family’s ability to cope if conflict is also high in the G2–G3 family environment. If high conflict interactions with G1–G2 families occur in G2–G3 families who are already “stretched to the breaking point” by high conflict in the G2–G3 family environment, the combined effects of such conflict could overwhelm G2–G3 families’ coping resources (Cowan & Cowan, 2012; Rothenberg et al., 2016). Therefore, due to the degradation of social support systems and overwhelming of coping resources, the combination of G1–G2 and G2–G3 high conflict family environments could have synergistic effects on G2 and G3s, above and beyond those seen as a result of conflict in just G1–G2 or G2–G3 family environments.
Intriguingly, the interactive effects of G1–G2 and G2–G3 family conflict predicted differences in some measures of G2 social role functioning but not others. Specifically, G1–G2-by-G2–G3 family conflict interactions predicted greater impairments in G2s’ marital domain of functioning (e.g., marital satisfaction, distress, romantic partner social support), as opposed to the parenting domain of functioning (where main effects of G1–G2 family conflict, but not its interaction with G2–G3 family conflict, predicted G2 parental support and consistency). Cross-sectional evidence from the marital therapy literature indicates that retrospective recall of family of origin conflict is a prominent predictor of current family conflict and associated marital functioning (e.g., Epstein & Baucom, 2002). Moreover, the extensive body of research supporting the Emotional Security Hypothesis indicates that marital dysfunction is especially likely to spill over to affect the broader family environment, parenting practices and subsequent child development (Cummings et al., 2015; Cummings & Schatz, 2012; Rothenberg, Hussong, & Chassin, 2016, though also see Ackerman et al., 2013 for contradictory findings). Therefore, it is possible that the interactive effects of multigenerational family conflict increase risk for marital dysfunction (as demonstrated in the current findings), and that such marital dysfunction subsequently predicts the emergence of parenting deficits. Such hypothesized mediated moderation could explain current findings that G1–G2 family conflict (but not the interaction term) is associated with G2 parenting deficits in the G2–G3 family environment. However, due to space constraints and the post-hoc nature of this hypothesis, it will not be tested in the current manuscript (though it will be among the first hypotheses our group will test in the future).
Similar processes may account for the current G3 results. Specifically, for G3s it does not appear that the synergistic effects of multigenerational conflict accounts for why G1–G2 family conflict predicts G3 psychopathology symptoms, because none of the interaction terms that index such synergistic family conflict were significant in predicting G3 outcomes. Alternatively, G3 psychopathology may be indirectly affected by G1–G2 family conflict through the degradation of parental support systems that result from G2 exposure to G1–G2 family conflict. Specifically, experiencing high family conflict in their family of origin may rob G2s of adaptive models for providing the support their children need to thrive in their family of destination (even if G2s successfully avoid recreating high family conflict in their family of destination). This explanation enjoys ample support from single-generation literature examining the Emotional Security Hypothesis, which demonstrates that marital and family conflict affects parental support of child emotional security, which consequently leads to numerous child psychopathology outcomes (Cummings et al., 2015; Cummings & Schatz, 2012).
Additionally, neither G1–G2 family conflict nor the G1–G2-by-G2–G3 family conflict interaction predicted G2 or G3 problematic alcohol and drug use. However, longitudinal research indicates that associations between family conflict and serious problematic substance use in adolescents and adults are often mediated and moderated by a complex constellation of variables not captured in the current study including child polygenic risk and impulsivity (Elam et al., 2016), parental negative emotionality (Bailey et al., 2013), and combinations of parent traits and substance use behaviors (Gottfredson, Hussong, Ennett, & Rothenberg, 2016). Future investigations of the multigenerational effects of family conflict on substance use would do well to include such mediating and moderating mechanisms.
Strengths and Limitations
The present study has numerous strengths. The study utilized a multigenerational data set that allowed for the rare opportunity to obtain prospective reports of family conflict in each generation. Moreover, the present study controlled for G1 psychopathology when assessing G2 outcomes, and G2 psychopathology when assessing G3 outcomes. Controlling for parent psychopathology in this way revealed that multigenerational family conflict was associated with deleterious G2 and G3 outcomes above and beyond multigenerational continuities in psychopathology. Additionally, the study captured both G1–G2 and G2–G3 families at similar points in child development. Comparison of families at similar points in child development is both recommended and uncommon in multigenerational research (Conger et al., 2009). Finally, the present study measured family conflict using multiple reporters in each family generation, and captured a range of psychopathology and functional impairment in the assessments used.
However, the present study also had limitations. Family conflict in each generation was self-reported, as opposed to observed, making it possible that reporter bias affected estimates of conflict. Additionally, the use of parceling techniques in aggregating reports of family conflict means that each family member’s report of family conflict was weighted equally in estimation of latent family conflict variables. Equal weighting of reports may not account for the outsized significance one family members’ perspective has on shaping family conflict. Furthermore, G2 partner and G3 adolescent reports of family conflict were not available for all families. Consequently, some estimates of G2–G3 family conflict incorporated fewer perspectives than others. Furthermore, the large number of analyses conducted as part of the current study increases risk of Type I error. However, some analytic methodologists (e.g., Nakagawa, 2004) discourage applying common multiple-comparison corrections for Type I error (e.g., a Bonferroni correction), especially in investigating novel phenomena (like the effects of intergenerational family conflict), deeming them too conservative and therefore likely to increase Type II error. Consequently, we decided to publish our present results in full while acknowledging the risk of Type I error inflation, with the hope that future scientists can replicate and build on our work. Finally, although we controlled for parent psychopathology in study analyses, we were unable to directly measure genetic effects that may increase risk for multigenerational continuities in alcoholism, externalizing behavior, or internalizing behavior.
Future work addressing these limitations is warranted as are studies that permit disentangling underlying mechanisms. For example, the current study was unable to determine whether multigenerational family conflict is a cause of G2 and G3 psychopathology and social impairment or whether continuity in G2 psychopathology and social impairment over the early lifespan fosters G2–G3 family conflict as well as G3 psychopathology. Future investigations could parse apart effects by studying the development of family conflict and G2 psychopathology simultaneously over time to understand how these different processes mutually influence one another.
Summary
The current study demonstrated that distal G1–G2 family conflict is a unique predictor of current G2 and G3 impairment, even after considering G2–G3 family conflict and continuities in G2 pychopathology. In G2s, G1–G2 family conflict may convey its risk on functioning by exacerbating the effects of G2–G3 family conflict. Taken together, study results suggest that adults and adolescents from families who experience multigenerational family conflict are at greater risk for psychopathology and social impairment than are those who experience family conflict in only the most recent family generation. Therefore, conflict in parents’ family of origin may be a useful risk factor for identifying high-risk families in need of treatment and prevention programming.
Acknowledgments
This research study was supported by an institutional National Research Service Award (NRSA) and predoctoral fellowship provided by the National Institute of Child Health and Human Development (T32-HD07376) through the Center for Developmental Science, University of North Carolina at Chapel Hill to the first author (W.R.) and by Grant AA016213 from the National Institute of Alcohol Abuse and Alcoholism (to L.C.). We gratefully acknowledge the contribution of our study participants and the Developmental Risk and Resilience Lab at UNC-Chapel Hill.
Footnotes
Some ideas presented in this manuscript were disseminated in the form of a poster presentation at the 2015 Biennial Meeting of the Society for Research in Child Development. However, most ideas presented in this manuscript, and all analyses presented in this manuscript, have never been disseminated elsewhere.
References
- Achenbach T, Edelbrock C. Behavioral problems and competencies reported by parents of normal and disturbed children aged four through sixteen. Chicago: University of Chicago Press; 1981. (Monograph of the Society for Research in Child Development). [PubMed] [Google Scholar]
- Ackerman RA, Kashy DA, Donnellan MB, Neppl T, Lorenz FO, Conger RD. The interpersonal legacy of a positive family climate in adolescence. Psychological Science. 2013;24(3):243–250. doi: 10.1177/0956797612447818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bailey JA, Hill KG, Guttmannova K, Oesterle S, Hawkins JD, Catalano RF, McMahon RJ. The association between parent early adult drug use disorder and later observed parenting practices and child behavior problems: Testing alternate models. Developmental Psychology. 2013;49(5):887–899. doi: 10.1037/a0029235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Best DW, Wilson AS, MacLean S, Savic M, Reed M, Bruun A, Lubman DI. Patterns of family conflict and their impact on substance use and psychosocial outcomes in a sample of young people in treatment. Vulnerable Children and Youth Studies. 2014;9(2):114–122. [Google Scholar]
- Belsky J, Jaffee SR, Sligo J, Woodward L, Silva PA. Multigenerational transmission of warm-sensitive-stimulating parenting: A prospective study of mothers and fathers of 3-year-olds. Child Development. 2005;76(2):384–396. doi: 10.1111/j.1467-8624.2005.00852.x. [DOI] [PubMed] [Google Scholar]
- Bloom BL. A factor analysis of self-report measures of family functioning. Family Process. 1985;24(2):225–239. doi: 10.1111/j.1545-5300.1985.00225.x. [DOI] [PubMed] [Google Scholar]
- Chase RM, Eyberg SM. Clinical presentation and treatment outcome for children with comorbid externalizing and internalizing symptoms. Journal of Anxiety Disorders. 2008;22(2):273–282. doi: 10.1016/j.janxdis.2007.03.006. [DOI] [PubMed] [Google Scholar]
- Chassin L, Pitts SC, DeLucia C, Todd M. A longitudinal study of children of alcoholics: Predicting young adult substance use disorders, anxiety, and depression. Journal of Abnormal Psychology. 1999;108(1):106–119. doi: 10.1037//0021-843x.108.1.106. [DOI] [PubMed] [Google Scholar]
- Conger RD, Belsky J, Capaldi DM. The multigenerational transmission of parenting: Closing comments for the special section. Developmental Psychology. 2009;45(5):1276–1283. doi: 10.1037/a0016911. [DOI] [PubMed] [Google Scholar]
- Conger RD, Neppl T, Kim K, Scaramella L. Angry and aggressive behavior across three generations: A prospective, longitudinal study of parents and children. Journal of Abnormal Child Psychology. 2003;31(2):143–160. doi: 10.1023/A:1022570107457. [DOI] [PubMed] [Google Scholar]
- Cowan PA, Cowan CP. Normative family transitions, couple relationship quality, and healthy child development. In: Walsh F, Walsh F, editors. Normal family processes: Growing diversity and complexity. 4th. New York, NY, US: Guilford Press; 2012. pp. 428–451. [Google Scholar]
- Cummings EM, Koss KJ, Davies PT. Prospective relations between family conflict and adolescent maladjustment: Security in the family system as a mediating process. Journal of Abnormal Child Psychology. 2015;43(3):503–515. doi: 10.1007/s10802-014-9926-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cummings E, Schatz JN. Family conflict, emotional security, and child development: Translating research findings into a prevention program for community families. Clinical Child and Family Psychology Review. 2012;15(1):14–27. doi: 10.1007/s10567-012-0112-0. [DOI] [PubMed] [Google Scholar]
- Elam KK, Wang FL, Bountress K, Chassin L, Pandika D, Lemery-Chalfant K. Predicting substance use in emerging adulthood: A genetically informed study of developmental transactions between impulsivity and family conflict. Development And Psychopathology. 2016;28(3):673–688. doi: 10.1017/S0954579416000249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- El-Sheikh M, Erath SA. Family conflict, autonomic nervous system functioning, and child adaptation: State of the science and future directions. Development and Psychopathology. 2011;23(2):703–721. doi: 10.1017/S0954579411000034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Epstein NB, Baucom DH. Enhanced cognitive-behavioral therapy for couples: A contextual approach. Washington, DC, US: American Psychological Association; 2002. [Google Scholar]
- Formoso D, Gonzales NA, Aiken LS. Family conflict and children’s internalizing and externalizing behavior: Protective factors. American Journal of Community Psychology. 2000;28(2):175–199. doi: 10.1023/A:1005135217449. [DOI] [PubMed] [Google Scholar]
- Furman W, Buhrmester D. Children’s perceptions of the personal relationships in their social networks. Developmental Psychology. 1985;21(6):1016–1024. [Google Scholar]
- Gottfredson NC, Hussong AM, Ennett ST, Rothenberg WA. The role of parental engagement in multigenerational transmission of smoking behavior and identity. Journal of Adolescent Health. 2016 doi: 10.1016/j.jadohealth.2016.11.004. Advanced online publication. to be published in print later in 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herrenkohl TI, Lee JO, Kosterman R, Hawkins JD. Family influences related to adult substance use and mental health problems: A developmental analysis of child and adolescent predictors. Journal of Adolescent Health. 2012;51(2):129–135. doi: 10.1016/j.jadohealth.2011.11.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horwitz BN, Ganiban JM, Spotts EL, Lichtenstein P, Reiss D, Neiderhiser JM. The role of aggressive personality and family relationships in explaining family conflict. Journal of Family Psychology. 2011;25(2):174–183. doi: 10.1037/a0023049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jaycox LH, Repetti RL. Conflict in families and the psychological adjustment of preadolescent children. Journal of Family Psychology. 1993;7(3):344–355. [Google Scholar]
- Jouriles EN, Rosenfield D, McDonald R, Mueller V. Child involvement in interparental conflict and child adjustment problems: A longitudinal study of violent families. Journal of Abnormal Child Psychology. 2014;42(5):693–704. doi: 10.1007/s10802-013-9821-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimonis ER, Frick PJ, McMahon RJ. Conduct and oppositional defiant disorders. In: Mash EJ, Barkley RA, Mash EJ, Barkley RA, editors. Child psychopathology. 3rd. New York, NY, US: Guilford Press; 2014. pp. 145–179. [Google Scholar]
- Kishton JM, Widaman KF. Unidimensional versus domain representative parceling of questionnaire items: An empirical example. Educational and Psychological Measurement. 1994;54:757–765. [Google Scholar]
- Kouros CD, Garber J. Trajectories of individual depressive symptoms in adolescents: Gender and family relationships as predictors. Developmental Psychology. 2014;50(12):2633–2643. doi: 10.1037/a0038190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ladd GW, Profilet SM. The Child Behavior Scale: A teacher-report measure of young children’s aggressive, withdrawn, and prosocial behaviors. Developmental Psychology. 1996;32(6):1008–1024. doi: 10.1037/0012-1649.32.6.1008. [DOI] [Google Scholar]
- Lamborn SD, Mounts NS, Steinberg L, Dornbusch SM. Patterns of competence and adjustment among adolescents from authoritative, authoritarian, indulgent, and neglectful families. Child Development. 1991;62(5):1049–1065. doi: 10.1111/j.1467-8624.1991.tb01588.x. [DOI] [PubMed] [Google Scholar]
- Lee MR, Chassin L, MacKinnon DP. Role transitions and young adult maturing out of heavy drinking: Evidence for larger effects of marriage among more severe premarriage problem drinkers. Alcoholism: Clinical And Experimental Research. 2015;39(6):1064–1074. doi: 10.1111/acer.12715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lieberson S. Making it count: The Improvement of social research and theory. Berkeley, CA: University of California Press; 1985. [Google Scholar]
- McMahon RJ, Forehand RL. Helping the noncompliant child: Family-based treatment for oppositional behavior. 2nd. New York, NY, US: Guilford Press; 2003. [Google Scholar]
- Muthén LK, Muthén BO. Mplus User’s Guide. 7th. Los Angeles, CA: 1998–2015. [Google Scholar]
- Nakagawa S. A farewell to Bonferroni: The problems of low statistical power and publication bias. Behavioral Ecology. 2004;15(6):1044–1045. doi: 10.1093/beheco/arh107. [DOI] [Google Scholar]
- Robins LN, Helzer JE, Ratcliff KS, Seyfried W. Validity of the Diagnostic Interview Schedule, Version II: DSM-III diagnoses. Psychological Medicine. 1982;12:855–870. doi: 10.1017/s0033291700049151. [DOI] [PubMed] [Google Scholar]
- Rothenberg WA, Hussong AM, Chassin L. Modeling trajectories of adolescent-perceived family conflict: Effects of marital dissatisfaction and parental alcoholism. Journal of Research on Adolescence. 2016 doi: 10.1111/jora.12259. Advanced online publication, to be published in print later in 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rothenberg WA, Hussong AM, Chassin L. Multigenerational transmission of high conflict family environments. Development and Psychopathology. 2016;28(1):293–308. doi: 10.1017/S0954579415000450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schofield TJ, Conger RD, Neppl TK. Positive parenting, beliefs about parental efficacy, and active coping: Three sources of multigenerational resilience. Journal Of Family Psychology. 2014;28(6):973–978. doi: 10.1037/fam0000024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Todd M, Chassin L, Presson CC, Sherman SJ. Role stress, role socialization, and cigarette smoking: Examining multiple roles and moderating variables. Psychology of Addictive Behaviors. 1996;10(4):211–221. [Google Scholar]