

Abstract
High-calorie restaurant foods contribute to childhood overweight. Increased consumer demand for healthier kids’ meals may motivate the restaurant industry to provide additional healthy options. This study pilot-tested a combination of four strategies (toy incentive, placemats, server prompts, signage) designed to increase demand for healthier kids’ meals, which were defined as those eligible for the National Restaurant Association’s Kids LiveWell program. Relative sales of healthier kids’ meals were examined before (n=3,473 total kids’ meal orders) and during Month 1 (n=3,546 total kids’ meal orders) and Month 2 of implementation (n=3,645 total kids’ meal orders) of an 8-week intervention in two locations each of a quick-service (QSR) and full-service (FSR) restaurant chain. Convenience samples of children (n=27) and their parents (n=28) were surveyed regarding parent and child perceptions of intervention components. Findings regarding the effectiveness and feasibility of the intervention were mixed. At the FSRs, the relative percentage of monthly sales from healthier kids’ meals increased from 5.0% of kids’ meal orders at baseline to 8.3% during Month 1, ending at 6.4% during Month 2. At the QSRs, the relative percentage of monthly sales from healthier kids’ entrees decreased from 27.5% at baseline to 25.2% during Month 1, ending at 25.9% during Month 2. Implementation quality tracking showed that consistent implementation of intervention components was a challenge; parent- and child-reported awareness of intervention components supported this finding. Future directions are discussed, aiming to build upon these findings and maximize the feasibility, effectiveness, and sustainability of efforts to promote healthier eating in restaurants.
Keywords: Restaurants, Eating, Children, Pilot, Intervention
INTRODUCTION
Child obesity prevalence has increased over the past three decades (1), alongside an increase in food purchased away from home (FAFH). Data indicate that American households now spend more than 40% of their total food budget on FAFH, up from 25% in 1970 (2). Compared to meals prepared at home, FAFH often contains more calories, saturated fat, sodium and added sugars (3). Specifically, national data indicate that consumption of foods from quick-service restaurants (QSR) is associated with a 126 calorie net increase in US children’s daily total energy intake; consuming full-service restaurant (FSR) food is associated with a net increase of 160 calories (4). Therefore, restaurants may be an important environment for reducing excess calorie consumption among children.
The extant literature highlights several potentially promising avenues for restaurant-based interventions. One technique to promote healthier meals to children is pairing food items with tangible rewards, such as toys. Although such incentives have traditionally promoted less-healthy foods in restaurants (e.g., a toy paired with a kids’ meal containing an entrée, French fries, and soda), studies in laboratories, homes, and schools show that incentives also offer the potential to promote healthy choices (5–7). A second approach is to target parents, given the role they play in children’s meal ordering (8,9). Prompting has increased sales of targeted items among adults (10), with some evidence that verbal prompts, (11,12), signage (13,14), and healthy primes on menus (15) can promote healthier ordering patterns. However, these efforts also traditionally target nutritionally poor options (e.g., adding dessert to a meal). More research is needed to test these strategies as they apply to the promotion of healthier kids’ meals within restaurants. Ecologically-valid studies will aid in understanding the effectiveness of these strategies among families as well as their synchrony with restaurant goals.
In this pilot study, a multi-component intervention (toy incentive, placemat, verbal prompts, signage) was designed to promote healthier kids’ meals and was implemented in two locations each of one QSR and one FSR restaurant chain. The aims of the current study include (1) evaluating the effectiveness of an 8-week pilot intervention by examining sales of healthier kids’ meals before and during the intervention’s implementation, and (2) assessing the fidelity with which each of four individual intervention components was implemented during the pilot study. Examination of these aims can highlight intervention approaches with initial evidence of effectiveness and feasibility, which is important for the development of larger-scale restaurant-based research. We hypothesized that sales of healthier kids’ meals would be higher during the intervention compared to baseline.
METHODS
Overview
Four restaurant locations in Southern California participated in an 8-week pilot intervention promoting healthier kids’ meals through four modifications to the restaurant environment. Two participating restaurants were from a national QSR chain and two were from a regional FSR chain. Comprehensive sales data were obtained from each restaurant before (February 2015) and throughout (March–April 2015) the intervention (n=10,664 children’s entrée orders in total). Convenience samples of families dining at the restaurants were surveyed at week 6 of the intervention in April 2015 to obtain perceptions of the intervention components. Research staff also tracked intervention component implementation.
Each study restaurant offered healthier kids’ meal options, defined as those that met the nutritional criteria of the National Restaurant Association’s Kids LiveWell (KLW) program (16). A KLW meal (entrée, side dish and beverage) must meet the following nutritional criteria: ≤600 total calories, ≤35% calories from total fat, ≤10% of calories from saturated fat, <0.5 grams of trans fat, ≤35% of calories from total sugars, ≤770 mg of sodium; the meal must include two of the following food groups: fruit, vegetables, lean protein, whole grains, and lower-fat dairy. Kids’ meals were pre-bundled (entrees plus side dishes) on the FSR menu; at the QSR, entrees and side items were listed separately because customers select these items individually. Two of 14 kids’ meals available at the FSR were KLW meals. At the QSRs, two of seven kids’ entrees were KLW eligible when ordered with KLW side items. Institutional Review Board approval for all research methodology was obtained through Tufts University.
Sales Data
All four restaurant locations provided the total quantity of each kids’ meal item sold during the month prior to the intervention (February 2015, baseline), as well as during March and April 2015, referred to herein as Months 1 and 2 of the 8-week intervention. The organization of these data corresponded with the way kids’ meals were offered on each restaurant’s menu: for FSRs sales data were provided for bundled meals, while for QSRs individual kids’ meal components (i.e., entrees and side dishes) were listed (and ordered) individually. Due to the format of sales data provided by the restaurants, bundled meals were analyzed for the FSRs and individual entrees were analyzed for the QSRs.
Intervention
Intervention components were based upon strategies from other contexts (6,17) and the results of focus groups conducted with 18 children at two community centers in the Boston area. The four participating restaurants each hosted a training session for servers to implement the following intervention components:
Super Crew® character toys (“Andy” and “Kira”) to be given to children ordering KLW meals;
Placemats featuring the Super Crew® characters, which included descriptions of the two KLW meals as well as fun activities, to be handed out to all children prior to placement of food orders;
Servers were trained to prompt families with children who appeared to be aged 12 or younger to try a KLW meal before taking their orders; and,
Signs (18″ × 24″) to be displayed in the restaurant, showing images of the Super Crew® and advertising the toy promotion with KLW meals.
The Super Crew® characters have been featured on 5,000 school websites in 45 U.S. states and in a public health campaign promoted by the American Institute for Cancer Research (http://www.aicr.org/healthykids/healthy-kids-today-prevent-cancer-tomorrow.html). The characters have special “powers” due to their consumption of healthy foods.
Intervention Measures
Implementation tracking
Implementation fidelity was tracked in two ways. First, implementation staff made weekly unannounced visits to each restaurant location throughout the intervention. Tracking methods included keeping a log of the number and location of signs installed in the restaurants, observing server interactions with customers to note recommendation of the KLW meals, and determining the number of placemats and toys available for the restaurant’s customers. Second, evaluation staff recorded the extent to which intervention components were implemented throughout each data collection day described below.
Parent and child perception of intervention components
Data were collected from convenience samples of parents (n=28) and their children (n=27) during week 6 of the 8-week intervention. Families were approached by trained researchers after they were seated at a table. Eligibility for family participation included: 1) having a child in 1st–4th grade who intended to order a meal, 2) the presence of the child’s parent or legal guardian, 3) speaking English, and 4) having no position of major influence in the restaurant industry (e.g., parent not a restaurant executive). Signed informed consent and permission for child participation were obtained from parents. All but one child provided assent; thus 27 children participated. Parent/child data were collected during dinner time across weekdays and weekend days, with the exception of one family participating during lunch. Demographic data are presented in Table 1.
Table 1.
Parent-reported demographic characteristics of participants recruited from two full-service restaurants and two quick-service restaurants participating in a pilot intervention promoting healthier* kids’ meals (n=28 families)
| Child sex | 57.1% male, 42.9% female |
| Child grade | 39.3% 1st, 14.3% 2nd, 32.1% 3rd, 14.3% 4th |
| Child ethnicity | 14.3% Hispanic/Latino, 82.1% non-Hispanic, 3.6% preferred not to answer |
| Child race | 78.6% White, 3.6% Black/African-American, 3.6% Asian, 3.6% American Indian/Alaskan Native, 3.6% Native Hawaiian/Pacific Islander, 3.6% multiracial |
| Child eligibility for free- or reduced-price school meals | 17.9% eligible, 78.6% ineligible, 3.6% did not know or preferred not to answer |
| Primary language spoken at home | 100% English |
| How often does child eat at any restaurant? | 10.7% a few times/year or less, 17.9% once/month, 46.4% a few times/month, 17.9% 1–3 times/week, 7.1% 4+ times/week |
| How often does child eat at this restaurant? | 78.6% a few times/year or less, 21.4% once/month, 10.7% a few times/month, 0% 1–3 times/week, 0% 4+ times/week |
| Parent relationship to child | 64.3% mother, 35.7% father; 89.2% primary caregivers |
| Parent age M (SD) | 40.0 (5.5) |
| Parent marital status | 92.9% married |
| Parent education level | 10.7% high school, 35.7% some college or Associate’s degree, 39.3% Bachelor’s degree, 14.3% graduate degree 14.3% Hispanic/Latino, 85.7% non-Hispanic |
| Parent ethnicity | 82.1% White, 0% African-American, 10.7% Asian, 0% American Indian/Alaskan Native, 3.6% Native |
| Parent race | Hawaiian/Pacific Islander, 0% multiracial |
According to the National Restaurant Association’s Kids LiveWell program
Surveys were designed to take less than 10 minutes and were administered on electronic tablets, with parent surveys self-administered and child surveys verbally administered by researchers. Survey questions presented herein appear in Figure 1. Additional questions administered to families as part of the overarching study are available in Anzman-Frasca et al. (18) and were used to describe parents’ and children’s perspectives on children’s meals in restaurants generally (as opposed to the specific intervention-focused questions described herein). In the former analyses, parents and children were interviewed at two time points (baseline and during the intervention), and any potential differences between time points were assessed before aggregating across them. In the present analysis, parent/child data are from one time point only (during the intervention), given the focus on families’ perceptions of the pilot intervention.
Figure 1.

Child Survey Questions
Data Analysis
Restaurant sales data were analyzed using Statistical Package for the Social Sciences (SPSS) Version 21.0 (19). Relative sales of healthier meals were calculated for the FSRs by summing the quantity of KLW bundled meals and dividing by total kids’ meals sold. For the QSRs, relative sales of healthier entrees were used as a proxy for healthier kids’ meals and were calculated by summing individual KLW entrees and dividing by total kids’ entrees sold. An aggregate indicator of healthier kids’ meal orders across restaurants was calculated by summing the quantity of bundled KLW meals (in the FSR) and KLW entrees (in the QSR) and dividing by total kids’ meals and entrees sold. McNemar tests of paired proportions were used to examine differences in the percentages of these healthier kids’ options sold at baseline versus Month 1 of implementation and baseline versus Month 2, by restaurant segment and for all four restaurants combined.
Frequencies were calculated to summarize results from the parent and child survey questions using Statistical Analysis System (SAS) 9.4 (20). Additionally, implementation quality data were summarized.
RESULTS
Analysis of effectiveness: Sales data
Across all four participating restaurants, healthier KLW meals made up 10.7% of kids’ meal orders at baseline, 13.2% at Month 1 (asymptotic p=0.16), and 12.2% at Month 2 (asymptotic p=0.77). At the FSRs, sales of healthier KLW meals increased significantly from 5.0% of kids’ meal sales at baseline to 8.3% in Month 1 (asymptotic p<0.05). Sales fell to 6.4% in Month 2, and were no longer significantly different from baseline (asymptotic p=0.18). In contrast, the relative percentage of KLW entrees sold at the QSRs significantly decreased over the two time periods (asymptotic p<.05) (Table 2).
Table 2.
Relative1 sales of healthier2 kids’ meals sold for two full-service restaurants and two quick-service restaurants implementing a pilot intervention promoting healthier kids’ meals3
| Restaurant | Baseline | Month 1 | Month 2 | |
|---|---|---|---|---|
| Full Service | FSR1 | 5.0% | 9.2% | 6.9% |
| Restaurant (FSR) | FSR2 | 4.9% | 7.0% | 5.5% |
| Total (FSR1 & FSR2) | 5.0% | 8.3%* | 6.4% | |
| Quick Service Restaurant (QSR): Entrees | QSR1 | 28.2% | 26.1% | 26.0% |
| QSR2 | 26.8% | 24.1% | 25.9% | |
| Total (QSR1 & QSR2) | 27.5% | 25.2%* | 25.9%* |
Relative sales are shown as percentages representing the number of healthier kids’ meals sold divided by the total number of kids’ meals sold at each time point. For FSRs, these percentages are over a total of 2,593, 2,532, and 2,568 kids’ meal orders at baseline, Month 1, and Month 2, respectively. For QSRs, these percentages are over a total of 880, 1,014, and 1,077 kids’ meals orders at baseline, Month 1, and Month 2, respectively.
According to the National Restaurant Association’s Kids LiveWell program
FSR sales include bundled kids’ meals (entrees with side dishes); QSR sales include entrees as proxies for kids’ meal sales.
Asterisks indicate that relative percentages are significantly different from baseline (p<.05). These comparisons were conducted for each segment (FSRs overall, QSRs overall).
Examining feasibility of specific intervention components: Fidelity data
Implementation tracking showed that intervention components were not implemented consistently across restaurant segments or over time (Figure 2), a finding corroborated by the parent and child surveys conducted during week 6 of the intervention. Data recorded by implementation staff indicated signage featuring the Super Crew® characters was present more often than not at the FSRs (88.9% of the time) and QSRs (77.8% of the time). However, during data collection, when asked whether they noticed the sign advertising a toy prize with kids’ meals, 89.3% of parents surveyed responded no, 3.6% (1 parent) responded yes, and 7.1% did not know.
Figure 2.
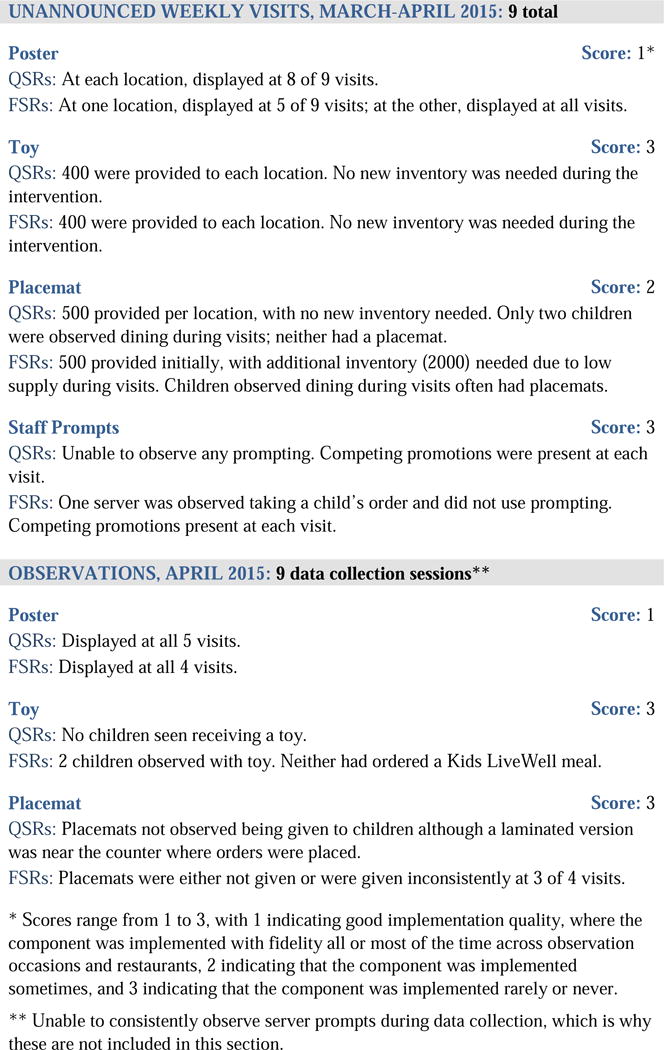
Implementation quality of four intervention components at two full-service and two quick-service restaurant chains
Servers were trained to provide a placemat featuring the Super Crew® characters to all children who dined at the FSRs and QSRs. This was to occur at the table in the FSRs and at the counter prior to ordering in the QSRs. However, when children were asked if they noticed the Super Crew® characters in the restaurant (while being shown a visual), only 48.2% responded that they had, most commonly on a poster/sign (46.2%) or placemat (30.8%). Servers were also trained to provide a Super Crew® toy to all children who ordered a KLW meal. Children who did not receive a Super Crew® toy (96.3%) were asked (while being shown a visual), if they wished they had received one; 61% said yes, 34.6% said no, and 1 child said “I don’t know”. Implementation staff recorded three deliveries of 500 placemats to replace those given away at one of the FSRs, with one delivery at the other FSR. No replacement deliveries were requested from either of the QSRs. Correspondingly, data from weekly random observations indicated that children received placemats more frequently at the FSRs compared to the QSRs (Figure 2). When asked if they had seen the placemat (while being shown a visual), 70.4% of children surveyed said no.
Observational data recorded during weekly visits indicated that servers were not heard consistently promoting KLW meals to families while taking orders. During data collection, when asked if the server recommended KLW meals, 92.9% of parents surveyed indicated that the server did not, and the others responded “I don’t know”.
DISCUSSION
The aims of this study were to pilot test the effectiveness of an intervention to promote healthier kids’ meals and to examine the feasibility of implementing four specific in-restaurant intervention components in QSRs and FSRs. Results showed an increase in sales of healthier kids’ meals from baseline to Month 1 of the intervention in FSRs but not across all four restaurants combined. Of the four intervention components, in-store signs were implemented with the highest fidelity in both the FSRs and QSRs, followed by the placemats in the FSR. Placemats were challenging to implement in the QSRs, where orders were placed at the counter. Fidelity data, combined with survey responses from parents and children, offer additional insights into the study’s results.
Increases in sales of KLW meals observed during this pilot intervention are consistent with previous research (21,22); however, the current study’s findings differed by restaurant segment. Sales of KLW meals at the FSRs increased significantly from baseline to Month 1 before falling in Month 2, at which point their magnitude remained higher, though not significant, compared to baseline. The peak in sales data at Month 1 suggests that implementation and effectiveness may have been better in the short term, a result corroborated by implementation questions administered to parents and children during Month 2. In contrast to the findings in the FSRs, relative sales of KLW entrees at the QSRs decreased over the 8-week study period. There are a number of possible explanations for the difference in findings between the QSRs vs. FSRs. One of the QSR managers explicitly commented that servers’ compliance with the intervention was impacted by corporate-level directives (data not shown). During the current study, there was a competing national-level promotion through which multiple adult meals could be purchased at a discounted price at the QSRs. Because the servers at the QSRs needed to prioritize this promotion, managerial staff indicated verbal prompts for KLW menu items were used less frequently, potentially impeding the promotion and sales of these items. Intervention approaches requiring active participation by restaurant staff (e.g., verbal prompts) may be more successful if restaurant leadership is involved with, and supportive of, the research project. Either way, approaches requiring less engagement (e.g., signs, placemats, defaults, menu changes) may be more sustainable.
Additionally, QSR managerial staff informed the research team that many senior citizens order from the children’s menu at this particular chain, a phenomenon that would be expected to affect kids’ meal sales data and potentially skew the current results, given that the interventions promoting KLW meals were not targeting this population. Our research with restaurant executives reiterated that senior citizens frequently order from children’s menus at some chains (18) suggesting that objective examinations of kids’ meal sales, while comprehensive, may be best understood when coupled with other, direct measures of ordering patterns, particularly when there are no age restrictions for ordering from the children’s menu.
Sales data from the FSRs reflect the entrees and side items ordered together and thus more accurately assess the extent to which KLW meals were ordered. Since it is not possible from the current QSR data to examine whether the KLW entrees were ordered alongside the specific side items that are required in order for the full meal to meet KLW criteria, the side item data were excluded from analysis. As a result, the data depicting KLW sales are less precise and are likely overestimated in the QSR compared to the FSR. For these reasons, the FSR sales data may be a better metric against which to evaluate initial effectiveness of the current intervention, versus the sales data from these QSRs.
In terms of intervention implementation, placemats that promoted the KLW meals were not consistently distributed to families prior to their meal selections; this appeared to be particularly challenging in the QSRs. The sign was the intervention component implemented with the highest fidelity across restaurants, possibly because it was the easiest component for restaurants to implement. However, the sign was smaller than other promotional signage in the restaurants; in future work, a larger sign with the restaurant’s branding should be considered to increase visibility of the intervention. Few participants reported being aware of the KLW meal options or the associated Super Crew® toy prize featured on the sign, highlighting the need to clearly and consistently communicate the nature of interventions and to complement signs with other feasible intervention components. Similarly, few families reported receiving verbal prompting by servers to purchase the KLW meals that came with the SuperCrew® toy, although data indicate that the toys were appealing to a substantial percentage of the children. Future research could examine the extent to which the familiarity of selected characters affects participants’ attention to these types of interventions, given mixed results regarding the role of character familiarity in related experimental studies (23–25). Data collectors noted that the distribution of the toy incentive was infrequent, although it was difficult to assess fidelity given the low frequency of KLW meal orders among the sample of families completing the surveys (one out of 28). One related problem was that the restaurants were expected to indicate on their menus and menu boards which of their kids’ meals qualified for KLW, but we observed that this was not done at either restaurant chain. While some research suggests that highlighting options as healthy may inhibit selection (26), in this case, failing to label the healthy options resulted in a disconnect between the KLW terminology used in the intervention materials and the descriptions of KLW meals on restaurant menus.
Implications of the current study’s findings are that feasible intervention components should take the onus off restaurant staff, given competing priorities. Of the components tested, signs and placemats appear to best fit this need. Placemats could include appealing characters and engaging activities and should be aesthetically pleasing and clearly depict any promotions of healthier options. Future efforts should ensure exposure to the placemat prior to placement of orders. For example, placemats could be stacked on a table or counter near the entrance of the restaurant, or a visual of the placemat, such as a large, attractive sign hung at the child’s eye level, could be displayed prominently for the child to view prior to being seated with a copy. In addition to future tests of these components, past research also supports the implementation of healthy “defaults” (e.g., fruit served as an automatic side dish with entrees) as a promising strategy to promote healthier ordering among children (27–29). Combining the feasible intervention components from the present study with such previously-successful approaches could offer the potential for increased effectiveness in future studies.
Strengths of the present study include evaluating comprehensive restaurant sales data to objectively assess all kids’ meal orders for a three-month period, including before and throughout the intervention. Furthermore, this study piloted a healthy kids’ meal promotion intervention in QSRs and FSRs to assess feasibility in each type of restaurant. This study, however, has limitations, including the use of a quasi-experimental design without randomization or a control group and the inabilities to generalize our results beyond the restaurants studied or test the differential effects of individual intervention components. While restaurants agreed to limit additional promotions during the 8-week intervention period, there was evidence suggesting that this did not occur, particularly in the QSRs. Additionally, the sales data, while comprehensive, do not include individual-level measures of families dining at the restaurants, precluding the ability to examine the extent to which the same families visited the restaurant during baseline and the intervention period; how often KLW entrees and side dishes were ordered together in the QSRs; or the number of kids’ meals ordered by adults, a limitation noted most explicitly in the QSRs. We also cannot determine the extent to which shifts in ordering patterns reflect seasonality (i.e., expected shifts in ordering during the study time period based on orders during the same period in previous years). Future studies could build upon this work by utilizing randomized study designs and collecting detailed individual-level data from a substantial sample of subjects.
Despite study limitations, the sales data showed some evidence supporting the intervention’s initial effectiveness, specifically in FSRs. Because many of the limitations mentioned above were less problematic in the FSRs, this suggests that efforts to build upon lessons learned and address implementation challenges could result in greater effectiveness and sustainability in future studies. The relatively low rates of healthier kids’ meal orders overall support the need for continued interventions aiming to bolster the availability and consumption of healthier choices among children in restaurants.
CONCLUSIONS
To our knowledge, this pilot study is one of the first to evaluate sales of healthier kids’ meals while also assessing the feasibility of implementing modifications to the QSR and FSR environments. Indications of initial intervention effectiveness in FSRs and findings about barriers to implementation of particular intervention components in each restaurant segment highlight opportunities for future research. Future efforts to promote healthy options in restaurants are needed, and the results of this pilot study indicate that interventions with the greatest potential success may be those that place minimal burden on restaurant staff. Rigorously testing intervention components that work within the context of restaurants’ realities and priorities may increase the likelihood of sustained fidelity and success of these interventions.
Acknowledgments
This research was funded by a CDC-funded Small Business Innovation Research grant (CDC 1R43HD080501-01A1) awarded to Accents on Health, Inc. (dba Healthy Dining), with Dr. Lopez as acting Principal Investigator on the award at the time the study was completed. Dr. Lopez currently receives funding through the University of Southern California (T32CA009492-31, PI: Mary Ann Pentz). Dr. Anzman-Frasca was Principal Investigator on a subcontract awarded to Tufts University to oversee the research aspects of the overarching study and was employed by ChildObesity180 and the Friedman School of Nutrition Science and Policy at Tufts University when the study was being conducted. The authors would like to thank Ilana Lemberger for her work on implementation and Lisa Tse, Sarah Lange, Emilia Mathews, and Rachel Banner for their contributions to evaluation components of this study, as well as the many other staff at ChildObesity180 at Tufts University who helped to pilot test study instruments. The authors also acknowledge Anita Jones-Mueller, the owner of Healthy Dining and Melissa Halas-Liang, who developed the Super Crew® characters, as well as the study restaurants and their staff.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Nanette V. Lopez, Keck School of Medicine, University of Southern California, Los Angeles, CA.
Sara C. Folta, Friedman School of Nutrition Science and Policy, Tufts University, Boston, MA.
Meaghan E. Glenn, Abt Associates, Cambridge, MA.
Vanessa M. Lynskey, ChildObesity180, Tufts University, Boston, MA.
Anjali A. Patel, Department of Research, Accents on Health, Inc. (dba Healthy Dining).
Stephanie Anzman-Frasca, Department of Pediatrics, University at Buffalo, Buffalo, NY.
References
- 1.Ogden CL, Carroll MD, Fryar CD, Flegal KM. Prevalence of obesity among adults and youth: United States, 2011–2014. Centers for Disease Control and Prevention Web site. 2015 http://www.cdc.gov/nchs/products/databriefs/db219.htm Published November 2015. Accessed March 18, 2016. [PubMed]
- 2.Food Expenditures. United States Department of Agriculture, Economic Research Service Web site. http://www.ers.usda.gov/data-products/food-expenditures.aspx. Published January 2016. Accessed March, 18 2016.
- 3.Todd JE, Mancino L, Lin BH. The impact of food away from home on adult diet quality. United States Department of Agriculture, Economic Research Service Web site. http://www.ers.usda.gov/Publications/ERR90/ERR90.pdf. Published February 2010. Accessed March 18, 2016.
- 4.Powell LM, Nguyen BT. Fast-food and full-service restaurant consumption among children and adolescents: Impact on energy, beverage and nutrient intake. JAMA Pediatr. 2013;167(1):14–20. doi: 10.1001/jamapediatrics.2013.417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cravener TL, Schlechter H, Loeb KL, et al. Feeding strategies derived from behavioral economics and psychology can increase vegetable intake in children as part of a home-based intervention: results of a pilot study. J Acad Nutr Diet. 2015;115(11):1798–1807. doi: 10.1016/j.jand.2015.03.024. [DOI] [PubMed] [Google Scholar]
- 6.McAlister AR, Cornwell TB. Collectible toys as marketing tools: understanding preschool children’s responses to foods paired with premiums. J Public Policy Mark. 2012;31:195–205. [Google Scholar]
- 7.Morrill BA, Madden GJ, Wengreen HJ, et al. A randomized controlled trial of the Food Dudes program: tangible rewards are more effective than social rewards for increasing short-and long-term fruit and vegetable consumption [published online ahead of print August 8, 2015] J Acad Nutr Diet. 2015 doi: 10.1016/j.jand.2015.07.001. [DOI] [PubMed] [Google Scholar]
- 8.Holmes AS, Serrano EL, Machin JE, Duetsch T, Davis GC. Effect of different children’s menu labeling designs on family purchases. Appetite. 2013;62:198–202. doi: 10.1016/j.appet.2012.05.029. [DOI] [PubMed] [Google Scholar]
- 9.Castro IA, Williams CB, Madanat H, Pickrel JL, Jun HJ, Zive M, Gahagan S, Ayala GX. Food ordering for children in restaurants: Multiple sources of influence on decision making. Public Health Nutr. 2016;19(13):2404–9. doi: 10.1017/S1368980016001403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ebster C, Wagner U, Valis S. The effectiveness of verbal prompts on sales. J Retail Consum Services. 2006;13:169–176. [Google Scholar]
- 11.Kleef E, Broek O, Trijp H. Exploiting the spur of the moment to enhance healthy consumption: verbal prompting to increase fruit choices in a self-service restaurant. Appl Psychol Health Well Being. 2015;7:149–66. doi: 10.1111/aphw.12042. [DOI] [PubMed] [Google Scholar]
- 12.Schwartz J, Riis J, Elbel B, Ariely D. Inviting consumers to downsize fast-food portions significantly reduces calorie consumption. Health Aff. 2012;31:399–407. doi: 10.1377/hlthaff.2011.0224. [DOI] [PubMed] [Google Scholar]
- 13.Nothwehr FK, Snetselaar L, Dawson J, Schultz U. Promoting healthy choices in non-chain restaurants: effects of a simple cue to customers. Health Promot Pract. 2013;14:132–8. doi: 10.1177/1524839912437368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wagner JL, Winett RA. Prompting on low-fat, high-fiber selection in a fast-food restaurant. J Appl Behav Anal. 1988;21:179–85. doi: 10.1901/jaba.1988.21-179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Stutts MA, Zank GM, Smith KH, Williams SA. Nutrition information and children’s fast food menu choices. J Consum Aff. 2011;45(1):52–86. [Google Scholar]
- 16.Kids LiveWell Program [Internet] National Restaurant Association. http://www.restaurant.org/Industry-Impact/Food-Healthy-Living/Kids-LiveWell-Program. Accessed March, 18 2016.
- 17.McAlister AR, Cornwell TB. Children’s brand symbolism understanding: Links to theory of mind and executive functioning. Psychology & Marketing. 2010;27(3):203–28. [Google Scholar]
- 18.Anzman-Frasca S, Folta SC, Glenn ME, et al. Healthier children’s meals in restaurants: An exploratory study to inform approaches that are acceptable across stakeholders. J Nutr Educ and Behav. 2017;49(4):285–95. doi: 10.1016/j.jneb.2016.11.009. [DOI] [PubMed] [Google Scholar]
- 19.IBM SPSS Statistics for Windows [computer program] Version 21.0. Armonk, NY: IBM Corp; 2012. [Google Scholar]
- 20.SAS [computer program] Version 9.4. Cary, NC: SAS Institute Inc; 2014. [Google Scholar]
- 21.Lee-Kwan SH, Bleich SN, Kim H, Colantuoni E, Gittelsohn J. Environmental intervention in carryout restaurants increases sales of healthy menu items in a low-income urban setting. Am J Health Promot. 2015;29(6):357–64. doi: 10.4278/ajhp.130805-QUAN-408. [DOI] [PubMed] [Google Scholar]
- 22.Fitzgerald CM, Kannan S, Sheldon S, Allen Eagle K. Effect of a promotional campaign on heart-healthy menu choices in community restaurants. J Am Diet Assoc. 2004;104:429–32. doi: 10.1016/j.jada.2003.12.019. [DOI] [PubMed] [Google Scholar]
- 23.Wansink B, Shimizu M, Camps G. What would batman eat?: Priming children to make healthier fast food choices. Ped Obes. 2012;7:121–23. doi: 10.1111/j.2047-6310.2011.00003.x. [DOI] [PubMed] [Google Scholar]
- 24.de Droog SM, Valkenburg PM, Buijzen M. Using brand characters to promote young children’s liking of and purchase requests for fruit. J Health Commun. 2010;16:79–89. doi: 10.1080/10810730.2010.529487. [DOI] [PubMed] [Google Scholar]
- 25.Kotler JA, Schiffman JM, Hanson KG. The influence of media characters on children’s food choices. J Health Commun. 2012;17:886–98. doi: 10.1080/10810730.2011.650822. [DOI] [PubMed] [Google Scholar]
- 26.Raghunathan R, Naylor RW, Hoyer WD. The unhealthy = tasty intuition and its effects on taste inferences, enjoyment, and choice of food products. J Mark. 2006;70:170–84. [Google Scholar]
- 27.Anzman-Frasca S, Dawes F, Sliwa S, Dolan PR, Nelson ME, Washburn K, Economos CD. Healthier side dishes at restaurants: An analysis of children’s perspectives, menu content, and energy impacts. Int J Behav Nutr Phys Act. 2014;11:81. doi: 10.1186/1479-5868-11-81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Peters J, Beck J, Lande J, Pan Z, Cardel M, Ayoob K, Hill JO. Using healthy defaults in Walt Disney World restaurants to improve nutritional choices. J Assoc Consum Res. 2016;1(1):92–103. doi: 10.1086/684364. http://dx.doi.org/10.1086/684364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wansink B, Love K. Slim by design: Menu strategies for promoting high-margin, healthy foods. Int J Hosp Manag. 2014;42:137–143. http://dx.doi.org/10.1016/j.ijhm.2014.06.006. [Google Scholar]