

Abstract
Aims
Dexmedetomidine (dexdor®) is approved in the European Union (EU) for sedation of adults in the intensive care unit (ICU). The present observational, retrospective study was requested by the European Medicines Agency to investigate dexmedetomidine use in clinical practice, with a particular focus on off‐label use, including the paediatric population.
Methods
Study countries and sites were chosen from those with highest dexmedetomidine use, based on sales. Site selection (blind) was conducted by a multispecialist, independent group. Anonymized data on demographics, treatment indication, dexmedetomidine dosing, concomitant medications and treatment effectiveness were collected retrospectively from records of all dexmedetomidine‐treated patients at the site during the enrolment period. Informed consent was waived, to avoid influencing the prescribing of dexmedetomidine. Recruitment was completed within 18 months of first site initiation.
Results
Data from 2000 patients were collected from 16 hospitals in four EU countries (Finland 750, Poland 505, Germany 470, Austria 275). The median age was 62 years, with more males (70.2%) than females. Dexmedetomidine was primarily used in the adult ICU (86.0%) for ICU sedation (78.6%) and mostly dosed according the product label. The intended sedative effect was obtained in 84.9% of administrations. Paediatric use (5.9% of patients, mostly in Austria and Finland) occurred mainly in the adult or paediatric ICU (75.6%) for sedation (67.2%).
Conclusions
Overall, most patients were treated with dexmedetomidine according to the product labelling. Use in children was limited but significant and similar in scope to that in adults. Administrations not fully according to the product labelling usually occurred in an ICU environment and reflected extensively investigated clinical uses of dexmedetomidine.
Keywords: chart review, dexmedetomidine, drug utilization, ICU sedation, perioperative sedation, procedural sedation
What is Already Known about this Subject
Dexmedetomidine was approved by the European Medicines Agency in 2011 for the sedation of adults in the intensive care unit (ICU), more than 10 years after its first approval in the USA.
Extensive literature reports of dexmedetomidine use in children, in patients outside the ICU and by alternative routes have raised concerns about widespread off‐label use.
What this Study Adds
Dexmedetomidine was found to be primarily used for the sedation of adults in the ICU with agitation, delirium or difficulty in weaning from the ventilator.
Most patients were treated with dexmedetomidine according to the product label; if not, treatment was almost always in an ICU environment and for a well‐recognized use of dexmedetomidine.
Tables of Links
| TARGETS |
|---|
| G protein‐coupled receptors 2 |
| α2A‐adrenoceptor |
| α2B‐adrenoceptor |
| α2C‐adrenoceptor |
| LIGANDS |
|---|
| Dexmedetomidine |
These Tables list key protein targets and ligands in this article that are hyperlinked to corresponding entries in http://www.guidetopharmacology.org, the common portal for data from the IUPHAR/BPS Guide to PHARMACOLOGY 1, and are permanently archived in the Concise Guide to PHARMACOLOGY 2015/16 2.
Introduction
Dexmedetomidine is a highly selective alpha‐2 adrenoceptor agonist that induces sedation via the activation of adrenoceptors in the locus coeruleus 3, 4, the site physiologically controlling vigilance and the predominantly noradrenergic nucleus in the brain. As a result of its combination of a specific site of action plus a non‐γ‐aminobutyric acid (GABA)‐ergic mode of effect, dexmedetomidine has a unique sedative profile, characterized by a calm but alert state in which patients are sedated but easily rousable to voice stimulation and able to cooperate with nursing and medical staff. This qualitatively distinctive nature of dexmedetomidine sedation has been confirmed in a range of clinical trials 5, 6, 7.
In the European Union (EU), dexmedetomidine (Dexdor®) was approved in 2011 for the sedation of adult intensive care unit (ICU) patients at a maintenance dose of up to 1.4 μg kg–1 h–1 intravenously, without a loading dose or time limit. It should be used in an ICU setting, and use in other environments is not recommended.
However, since its first approval in the USA in 1999, the use of dexmedetomidine in a broad range of clinical situations and patient groups has been documented in the medical literature, including perioperative use 8, procedural sedation 9 and use in children 10, 11. Alternative routes of administration, including intranasal 12, 13, subcutaneous 14, buccal 15 and intrathecal 16, 17 routes, have also been reported. Dexmedetomidine is approved for procedural sedation use in the USA and other countries but not the EU, and is not approved for paediatric use or non‐intravenous administration in any country. The present drug utilization study (DexDUS) was performed at the request of the Committee on Human Medicinal Products (CHMP) of the European Medicines Agency (EMA), at the time of dexmedetomidine approval in the EU, to describe the ways in which this agent is used in the EU, with the purpose of quantifying off‐label use, with particular reference to uses in children, and to record the occurrence of lack of effectiveness of dexmedetomidine.
Methods
General design considerations
DexDUS was a multinational, retrospective, non‐interventional chart review study of dexmedetomidine utilization in clinical practice. It was conducted at 18 study sites (16 institutions) in Austria, Germany, Finland and Poland between 13 June 2013 and 4 December 2014. Site principal investigators are identified in the Appendix.
Suitable countries were in the EU, had established dexmedetomidine use for at least 6 months and had at least two suitable teaching or nonteaching institutions. The steering group defined four regions comprising all EU member states, on predominantly geographical grounds, and selected a single country in each region, where possible, based on the extent of dexmedetomidine sales. Suitable institutions had to provide: access to patients from a broad range of specialities, including adult and paediatric ICU patients alike; projected use of dexmedetomidine in >50 patients during the period of data collection; ethical approval for participation if required; and resources adequate for the technical requirements of electronic data capture. Dexmedetomidine sales data, provided by the manufacturer Orion Pharma, were used to identify the highest users of the drug; however, final selection of sites was performed by the independent steering group (blinded to hospital name and location in order to avoid selection bias), based on extent of use of Dexdor, hospital characteristics and the ability to meet the study demands.
Data collection
All patients treated with dexmedetomidine at each participating site during the data‐capture period were to be included in the study unless they were participating in a clinical trial involving dexmedetomidine (the number of such patients was not recorded). Individual sites could not contribute >300 patients, or countries >750 patients in order to avoid having undue influence on the results. The database was closed when the recruitment target of 2000 patients was reached.
All relevant approvals (including local and/or national ethical approval) for participation were obtained for all sites. All patient data were collected retrospectively and fully anonymized at the time of entry by the investigator, allowing the requirement for informed consent to be waived.
For each patient, data were collected for the duration of the hospital stay or visit, and subsequent hospital visits were counted separately.
Data collection for each patient included demographics (age, gender), clinical reason for using dexmedetomidine (ICU sedation, perioperative use, procedural sedation including diagnostic procedures, or other), details of the dexmedetomidine administration (time, duration, dose, use of loading dose), concomitant medications and responses to questions regarding therapeutic effectiveness. ICU sedation was further categorized by reason for administration (protocol amendment after inclusion of 668 patients). As dexmedetomidine is titrated to effect and regularly adjusted as need changes, the ‘typical’ and maximum doses administered were recorded in the ranges <0.7 μg kg–1 h–1; 0.7–1.4 μg kg–1 h–1; and >1.4 μg kg–1 h–1, based on Summary of Product Characteristics (SmPC) dose recommendations. The duration of treatment was recorded in completed 24‐h periods, with treatment breaks <48 h disregarded, and readministrations of dexmedetomidine after a break of >48 h recorded as separate administrations.
The clinical location of dexmedetomidine administration was documented as reported (adult ICU, paediatric ICU, operating room, radiology/imaging, cardiac care/cardiology or other). It was also analysed using the post hoc simplified concept of ‘ICU environment’, defined by the steering group. That term acknowledged locations where the level of patient monitoring could be considered comparable to that of the ICU and included: paediatric ICU, operating rooms, postoperative anaesthesia care, and coronary care units. Endoscopy and radiology suites and similar locations were not considered as ICU environments.
Therapeutic effectiveness was addressed by the response to the following hierarchical questions: (i) Was dexmedetomidine discontinued owing to a lack of efficacy?; (ii) Was another sedative started owing to a lack of dexmedetomidine efficacy?; and (iii) Was the intended sedative effect achieved by dexmedetomidine? Dexmedetomidine treatment was classified as ‘effective’ if the intended sedative effect was achieved and the answer to questions (i) and (ii) was ‘no’.
A hierarchical analysis was developed to characterize uses of dexmedetomidine at variance with the manufacturer SmPC recommendations, collating the administrations in the order: adult or paediatric patient; reason for dexmedetomidine use; ICU environment (Yes/No); maximum dose >1.4 μg kg–1 h–1 (Yes/No).
Sample size and other statistical considerations
Data are presented using descriptive summary statistics: mean, median, interquartile range (IQR), standard deviation, minimum and maximum for continuous variables, counts and percentages for categorical variables.
The study was not designed to test any predefined hypothesis, and no statistical hypothesis testing was performed.
In the absence of a predetermined hypothesis, the target sample size was set empirically at 2000 patients. With this number of patients, it was estimated that: (i) the probability of observing at least one rare event would be 95% when the probability of event was 0.15%; (ii) a two‐sided 95% confidence interval for single proportion would extend between 1% and 2.2% from the observed proportion for an expected proportion that was between 5% and 95%.
Quality control and good practice
The study was performed according to the principles of good pharmacoepidemiology practice 18, 19 and published EMA guidance on good pharmacovigilance 20. Data quality checks were built into the electronic case report form to identify obvious data entry errors, although the use of anonymization largely precluded patient verification or data queries after submission of each patient's data.
Regular reviews of data capture compliance and data quality were undertaken throughout the study. These reviews of data quality included checks for possible duplicate subject information by searching the study database for subjects with identical data elements.
Study organization
An independent steering group, comprising pharmacoepidemiologists and intensive care physicians (also experienced in paediatric intensive care and anaesthesia), was responsible for scientific direction and key decisions during the study and operated according to a mutually agreed written charter. The steering group made decisions by consensus following discussion with the study team and exercised ‘closed’ sessions without sponsor or Clinical Research Organisation representatives. The charter defined a process to be followed in the event of conflict with sponsor representatives; this was not invoked. The steering group selected sites (see methods section), approved the protocol and reviewed emerging data. Steering group members are identified in the Appendix. The study was sponsored by Orion Corporation, Orion Pharma.
Results
A total of 2159 administrations of dexmedetomidine were recorded in 2000 patients during the 18 months of study conduct (13 June 2013 to 4 December 2014), in Finland (n = 750), Poland (n = 505), Germany (n = 470) and Austria (n = 275) (Table 1). The country enrolment limit of 750 patients was reached in Finland, and one Polish site included the maximum 300 patients; further patient accrual at these sites was prohibited. Thirteen of the 16 participating sites were university hospitals, and three were general hospitals located in Finland (n = 2) and Poland (n = 1). All sites had an adult ICU. Only four sites had a separate paediatric ICU but all sites reported the capacity to treat paediatric ICU patients.
Table 1.
Demographic characteristics of patients
| Finland n = 750 | Poland n = 505 | Germany n = 470 | Austria n = 275 | Total n = 2000 | |
|---|---|---|---|---|---|
| Gender, n ( % ) | |||||
| Female | 168 (22.4) | 167 (33.1) | 125 (26.6) | 96 (34.9) | 556 (27.8) |
| Male | 582 (77.6) | 338 (66.9) | 345 (73.4) | 179 (65.1) | 1444 (72.2) |
| Age, median (range) | 61 (0–102) | 63 (15–92) | 63 (15–93) | 57 (0–88) | 62 (0–102) |
| Age by category, n (%) | |||||
| ≤ 27 days | 3 (0.4) | – | – | 2 (0.7) | 5 (0.3) |
| >27 days to <2 years | 14 (1.9) | – | – | 11 (4.0) | 25 (1.3) |
| 2–11 years | 25 (3.3) | – | – | 11 (4.0) | 36 (1.8) |
| 12–17 years | 40 (5.3) | 3 (0.6) | 1 (0.2) | 8 (2.9) | 52 (2.6) |
| 19–65 years | 375 (50.0) | 307 (60.8) | 260 (55.3) | 154 (56.0) | 1096 (54.8) |
| >65 years | 293 (39.1) | 195 (38.6) | 209 (44.5) | 89 (32.4) | 786 (39.3) |
n, number of patients
Patient characteristics
The demographic features of the 2000 patients who contributed data to DexDUS are shown in Table 1, stratified by country.
Patients were predominantly male (72.2%), with a median age of 62 years, of whom 39.3% were >65 years. Children accounted for 118 patients (5.9% overall; Austria 11.6%, Finland 11.2%, Poland 0.6%, Germany 0.2%) at seven sites, while in Germany and Poland there were no children <12 years treated with dexmedetomidine.
Primary indication
The most frequently recorded primary indication was ICU sedation (78.6%; 1696/2159 administrations), followed by perioperative use (15.5%, 335 administrations) and procedural sedation (5.0%, 108 administrations) (Figure 1 and Table 2). Other indications accounted for 20 administrations (<1%).
Figure 1.
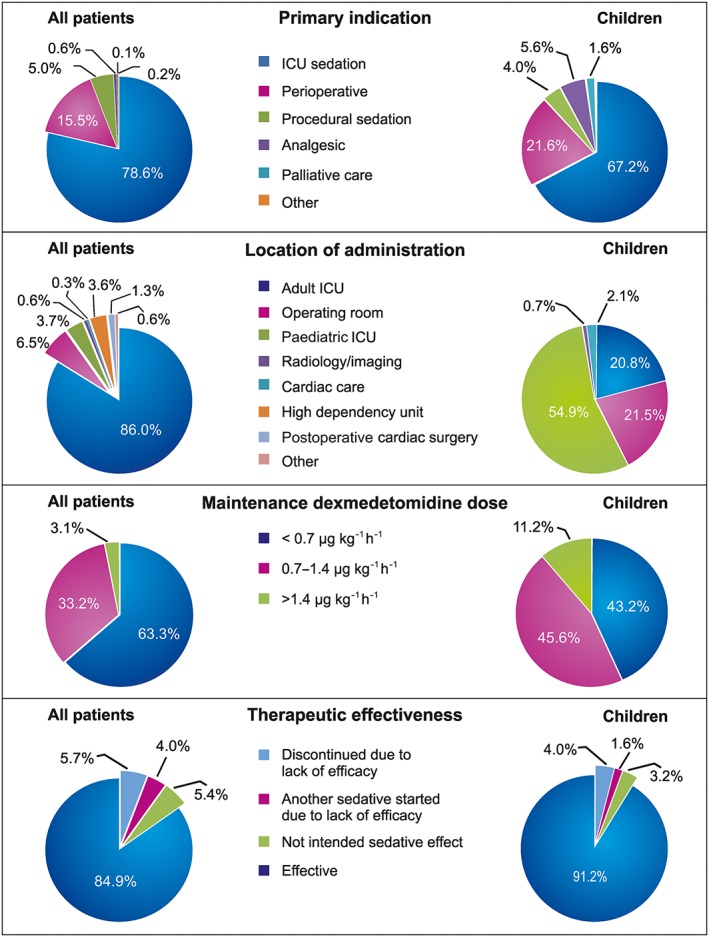
Summary of dexmedetomidine administrations in all patients and in children. ICU, intensive care unit
Table 2.
Use of dexmedetomidine by primary indication and location [number of administrationsa (%)]
| Finland n = 840 | Poland n = 516 | Germany n = 484 | Austria n = 319 | Total n = 2159 | |
|---|---|---|---|---|---|
| Primary indication | |||||
| ICU sedation b | 767 (91.3) | 167 (32.4) | 448 (92.6) | 314 (98.4) | 1696 (78.6) |
| Perioperative b | 44 (5.2) | 289 (56.0) | 2 (0.4) | – | 335 (15.5) |
| Procedural sedation b | 16 (1.9) | 59 (11.4) | 31 (6.4) | 2 (0.6) | 108 (5.0) |
| Analgesic b | 10 (1.2) | 1 (0.2) | 2 (0.4) | 1 (0.3) | 14 (0.6) |
| Palliative care b | 2 (0.2) | – | – | – | 2 (0.1) |
| Other | 1 (0.1) | – | 1 (0.2) | 2 (0.6) | 4 (0.2) |
| Location | |||||
| Adult ICU b | 674 (80.2) | 484 (100) | 413 (80.0) | 286 (89.7) | 1857 (86.0) |
| Paediatric ICU b | 46 (5.5) | 1 (0.2) | 33 (10.3) | 80 (3.7) | |
| Operating room b | 48 (5.7) | 93 (18.0) | 141 (6.5) | ||
| Radiology/imaging b | 8 (1.0) | 6 (1.2) | 14 (0.6) | ||
| Hospital ward b | 0 | ||||
| Cardiac care/cardiology | 4 (0.5) | 2 (0.4) | 6 (0.3) | ||
| high dependency unit | 77 (9.2) | 77 (9.2) | |||
| Postoperative cardiac surgery department | 28 (5.4) | 28 (5.4) | |||
| Other | 5 (0.6) | 7 (1.4) | 12 (0.6) | ||
| ICU environment | 828 (98.6) | 484 (100) | 507 (98.3) | 319 (100) | 2138 (99.0) |
ICU, intensive care unit
Patients may receive dexmedetomidine more than once
Prespecified category
ICU sedation accounted for 91–98% of recorded primary indications in Finland, Germany and Austria but only 32.4% in Poland, where perioperative use was recorded in 56.0% of administrations (for improving emergence from anaesthesia and to provide sedation during regional anaesthesia for surgery). In total, 422 adult administrations were for reasons other than ICU sedation, mostly at the Polish sites.
The most common specified reasons for ICU sedation were agitation despite existing sedation (32.2%), delirium (28.3%) and difficulty weaning from the ventilator (16.4%) (Table S1). Other reasons for use in ICU sedation included drug/alcohol withdrawal (3.6%), non‐invasive ventilation (4.8%) and initial postoperative sedation (3.8%). No specific category was selected for 20.1% of ICU sedation administrations.
Almost all administrations (adults 99.2%, children 96.8%) took place in an ICU environment (as defined for study purposes) in all countries (Table 1 ). Eighty‐six per cent of administrations occurred in the adult ICU, while at 11 of the 16 sites >95% of all administrations were given in that setting. Dexmedetomidine was given in the operating room at six sites (6.5% of administrations), the paediatric ICU at four sites (3.7% of administrations), radiology/imaging units at four sites (0.6% of administrations) and cardiac care/cardiology location at three sites (0.3% of administrations).
Frequency of administration and dosages
All recorded administrations were intravenous (data missing n = 10). Most patients (93.7%, n = 1874) received dexmedetomidine once only. In total, 103, 15, 7 and 1 patients were administered dexmedetomidine two, three, four and six times, respectively.
Loading doses of dexmedetomidine were used in fewer than 2% of administrations (n = 41: 3.9% of perioperative and 5.6% of procedural sedation administrations), and exceeded 1.0 μg kg–1 for eight administrations.
The median duration of treatment was 1 day but varied across sites and countries, as shown in Figure 2, being longest in Germany (3 days). The duration of treatment exceeded 14 days in 2.6% of administrations; the maximum treatment period was 74 days. Otherwise, the extent of exposure was similar between countries (Table 3).
Figure 2.
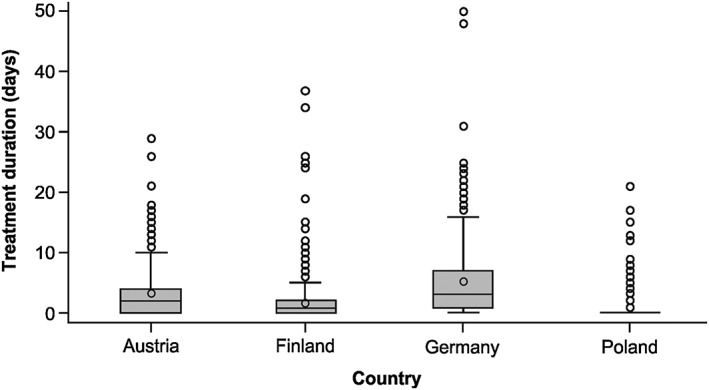
Duration of dexmedetomidine treatment (median, interquartile range and 95% confidence interval)
Table 3.
Dose and duration of treatment with dexmedetomidine [number of administrations (%)]
| Finland n = 840 | Poland n = 516 | Germany n = 484 | Austria n = 319 | Total n = 2159 | |
|---|---|---|---|---|---|
| Most common maintenance dose a | |||||
| <0.7 μg kg –1 h –1 | 542 (64.5) | 392 (74.0) | 278 (57.4) | 165 (74.0) | 1367 (63.3) |
| 0.7–1.4 μg kg –1 h –1 | 266 (31.7) | 130 (25.2) | 171 (35.3) | 150 (47.0) | 717 (33.2) |
| >1.4 μg kg –1 h –1 | 29 (3.5) | 1 (0.2) | 33 (6.8) | 4 (1.3) | 67 (3.1) |
| Maximum dose a | |||||
| <0.7 μg kg –1 h –1 | 315 (37.5) | 151 (29.3) | 210 (43.4) | 94 (29.5) | 770 (35.7) |
| 0.7–1.4 μg kg –1 h –1 | 433 (51.5) | 345 (66.9) | 207 (42.8) | 196 (61.4) | 1181 (54.7) |
| >1.4 μg kg –1 h –1 | 89 (10.6) | 17 (3.3) | 65 (13.4) | 29 (9.1) | 200 (9.3) |
| Duration of treatment a | |||||
| N | 840 | 513 | 480 | 318 | 2151 |
| Mean (SD) | 1.7 (3.9) | 1.0 (3.9) | 5.2 (5.8) | 3.3 (4.5) | 2.6 (4.7) |
| Median (range) | 1.0 (0–65) | 0 (0–74) | 3.0 (0–50) | 2.0 (0–29) | 1 (0–74) |
SD, standard deviation
Dose information is missing for eight adult administrations (0.4%)
The maximum approved dose of 1.4 μg kg–1 h–1 was exceeded at some point in 9.3% of patients (3.3% in Poland, where non‐ICU sedation indications predominated), although only 3.1% had a typical maintenance dose above this limit (Figure 1). In 35.7% of administrations, the maximum dose was below 0.7 μg kg–1 h–1 (the approved limit in most non‐EU countries). Only two of 17 administrations to adults outside the ICU environment involved doses exceeding 1.4 μg kg–1 h–1 (Table 4).
Table 4.
Summary of adherence to Summary of Product Characteristics (SmPC) (‘labelling’ recommendations)
| Number of administrations | SmPC element | ||||
|---|---|---|---|---|---|
| Indication | Location | Maintenance dose <1.4 μg kg–1 h–1 a | |||
| ICU sedation | ICU environment | ICU environment | Non‐ICU environment | ||
| Total | 2159 | 1696 (78.6%) | 2138 (99.0%) | 1933/2138 (90.4%) | 18/21 (85.7%) |
| Adults | 2034 | 1612 (79.3%) | 2017 (99.2%) | 1839/2017 (91.2%) | 15/17 (88.2%) |
| Children b | 125 | 84 (67.2%) | 121 (96.8%) | 94/121 (77.7%) | 3/4 (75.0%) |
ICU, intensive care unit
Dose information missing in eight adult administrations (0.4%)
All uses in patients <18 years of age are outside SmPC recommendations and thus ‘off‐label’
Paediatric use
The most recorded primary indication in paediatric patients was ICU sedation (67.2%, 84/125 administrations), followed by perioperative use (21.6%, 27/125 administrations) (Figure 1). Among patients less than 12 years of age, most administrations took place in the paediatric or adult ICU (56/74; 75.6%); other administration locations were the operating room (9.5%, 7/74), cardiac care/cardiology (4.1%, 3/74) and radiology/imaging (1.4%, 1/74). Among older children (12–17 years), administrations were numerically equally divided between the paediatric ICU, adult ICU and operating rooms (each, 23–24 episodes). All but four administrations occurred in an ICU environment.
A loading dose (0.5–1.0 μg kg–1) was given to a paediatric patient only once, (aged ≤27 days) and there were only five paediatric readministrations of dexmedetomidine. Doses of >1.4 μg kg–1 h–1 as either a maintenance (11.2%) or maximum (22.4%) dose appeared proportionately more frequent in paediatric than adult patients.
Treatment duration in neonates (≤27 days) was numerically longer than in the 12–17‐year age group (mean 7.0 ± 10.5 days vs. 1.8 ± 3.7 days), although the number of patients was low.
One of four administrations to children outside the ICU environment involved doses exceeding 1.4 μg kg–1 h–1 (Table 4).
Effectiveness of dexmedetomidine
Dexmedetomidine was effective in 84.9% of administrations (range 77.3–95% between countries) (Figure 1). It was discontinued owing to a lack of efficacy in 5.7% of administrations, and another sedative was started owing to a lack of efficacy in a further 4.0% of administrations. In an additional 5.4% of administrations, dexmedetomidine was judged not to provide the intended effect, although no other actions were identified. In patients recorded as receiving >1.4 μg kg–1 as their most common maintenance dose, discontinuations for lack of efficacy were higher (19.4%), although dexmedetomidine was considered effective in 64.2% of patients.
Dexmedetomidine was assessed as effective in all patients under the age of 2 years (n = 31) and 92.3% of children aged 2–11 years (36 of 39 patients). In all older age groups, the level of therapeutic effectiveness was similar (~85%) for all indications.
Discussion
The DexDUS study, performed at the request of the EMA at the time of approval in Europe, was the first known attempt to perform a formal drug utilization study of intravenous sedation in intensive care patients, and with 2000 patients was one of the largest patient series recorded for dexmedetomidine to date. The study characterized the way that dexmedetomidine was used in a sample of EU institutions and identifies the extent to which those users complied with the SmPC in terms of indication for use, dose, location of use and use in children.
In 14 of the 16 institutions, dexmedetomidine was predominantly used for the sedation of adults in the ICU, to manage agitation, delirium, difficult weaning and drug/alcohol withdrawal, and alternative uses were infrequent (<10% of administrations). In two institutions, it appeared to be used routinely for perioperative and procedural sedation in the operating room and ICU. Use in environments with potentially less intensive monitoring (non‐ICU environments, defined for this study), such as the endoscopy room or radiology suite, was rare and no use in a regular ward was identified. The study identified only intravenous use, normally without loading or bolus doses.
A small (5.8%) but relevant proportion of dexmedetomidine administrations occurred in children, in all age groups, most of which (88%) occurred in three sites. The identified reasons for using dexmedetomidine in children were somewhat similar to those in adults. There remains a high unmet need for alternative agents for ICU sedation in children 21 and, while many have reported their experience with dexmedetomidine in this population 22, 23, this remains an off‐label use.
A loading dose was used rarely (1.9% overall), consistent with EU prescribing recommendations as well as ICU sedation studies performed outside the EU 7, indicating that a loading dose is not normally needed when starting dexmedetomidine as a second‐line agent. Indeed, only 5.6% of administrations for procedural sedation involved a loading dose, even though one is conventionally used in published studies for both dexmedetomidine 24, 25 and other sedatives 26, 27 when used in this way. The study supported previous reports that patients commonly require a dose >0.7 μg kg–1 h–1 (the maximum approved dose in the USA and elsewhere) for maintenance of sedation with dexmedetomidine 28; indeed, 9.3% of adult and 22.4% of paediatric patients exceeded 1.4 μg kg–1 h–1 at some point during treatment. Without measured sedation levels, it could not be judged whether lower effectiveness, different therapeutic objectives or individual clinical practice explained the more frequent use of high doses in children but it is of note that higher clearance of dexmedetomidine has been reported in young children 29, 30.
The incidence of apparent lack of efficacy is comparable to existing data 5. Study withdrawal due to a lack of efficacy occurred in 9% and 14% of dexmedetomidine patients in the Midex and Prodex phase III studies, respectively. In those studies, continuous concomitant sedatives were not permitted, whereas in clinical practice, as in the present study, supplementing dexmedetomidine with a low dose of another sedative is a common way to manage inadequate response.
There were relevant differences between sites and countries. In Germany, dexmedetomidine was only used in the ICU; In Poland, perioperative and procedural sedation predominated; Austria had the highest rate of ICU sedation (98.4%), while Finland had a similar profile to Germany in reasons for use, but had greater use in children. In Finland, access to dexmedetomidine through a special access scheme prior to regulatory approval might be relevant to the broader use of this agent in children. Indeed, it is possible that data from Finland might predict future dexmedetomidine use as experience matures elsewhere in Europe. It may also be that preferences of individual prescribers are of greater impact than geographical factors in explaining the variation seen. With diversity in the type of hospitals included in the study, the results should be considered descriptive only and do not predict how dexmedetomidine is used at other specific institutions.
Of necessity, the study was performed while dexmedetomidine use was still relatively immature in most EU countries and institutions, with the exception of Finland, and countries requiring national formulary agreements or extensive local approval (e.g. France, Spain, Italy, the UK) did not establish use of this agent rapidly enough to be included in the study, which may have influenced the findings. Selecting sites based on high Dexdor sales may introduce a bias compared with institutions with more restricted use, while some were deterred from participating owing to concerns related to recording off‐label drug use.
Retrospective, anonymized data collection avoided interference with how dexmedetomidine was used (the Hawthorne effect) but made it not possible to confirm the completeness of patient inclusion and, of necessity, relies on information already collected in the patient record, which may not always be clear or complete. This limits the robustness of those variables needing some degree of interpretation by the data abstractor (e.g. reasons for starting dexmedetomidine and lack of efficacy). The systematic and blinded site selection process minimized selection bias but, still, the use of different sites might have led to alternative study conclusions and so the generalizability of the results is unclear.
The definition of an ICU environment was developed specifically for this study and was intended to reflect that the SmPC describes that dexmedetomidine should be used in an ‘ICU environment’. This broader definition describes more completely the on‐label use of this agent. It is not a standard definition, although it makes an important contribution to the number of administrations considered on‐label.
Recent reviews of regulatory‐driven studies to evaluate risk minimization measures, including labelling adherence, have focused on timelines of implementation, designs, etc. 31, 32 Individual studies are starting to be published. Based on the studies posted in the EU PAS registry 33, data are frequently extracted from automated healthcare databases or obtained from patient and healthcare professional surveys, or, as in our case, extracted from clinical records. In the last two options, the selection of study subjects is based on gathering diverse settings representative of various healthcare delivery systems owing to the lack of a defined sampling frame that would allow for random selection. Owing to the specific population of our study (including paediatric patients, and those in the ICU or a related setting), we encountered often‐fragmented hospital information systems. Variable population catchment areas, based on the different specialties of care, further complicated the selection of patients even when paediatric and adult patients alike were seen in a single hospital.
The study did not provide an endorsement or otherwise of any of the uses of dexmedetomidine recorded as neither treatment nor safety outcomes were recorded, and in that sense did not provide a basis to change clinical practice. Despite the potential limitations described above, we consider that DexDUS represents the best feasible attempt to address the questions raised by CHMP, without disrupting the essential naturalistic nature of the study.
This drug utilization study of dexmedetomidine performed early after the introduction of the product found that most patients were treated according to the product labelling, although there were important differences between countries and sites. Use in children was limited but significant and followed a similar pattern to that in adults. Administrations not fully according to the product labelling normally occurred in an ICU environment and reflected extensively investigated clinical uses of dexmedetomidine.
Competing Interests
The study was funded by Orion Corporation Orion Pharma, Espoo, Finland. M.W., P.P. and C.G. were employees of Orion Pharma during the study. S.P.G. is an employee of RTI International, a nonprofit research institute conducting research funded by public, private and commercial organizations, including pharmaceutical companies. R.A. was a paid consultant for Orion Corporation (Espoo, Finland) and Abbott Laboratories (Abbott Park, IL, USA), the original co‐developers of dexmedetomidine, and also for Hospira (Lake Forest, IL, USA). He was also one of the three original patent holders of ‘Use of dexmedetomidine for sedative effect in patients in an intensive care unit’ (WO/1999/049854). G.C. has received speaker fees from Orion Pharma and the Catholic University of Rome, and received research support for another study from Orion Pharma. M.L. is Director of EPES Epidemiology GmbH, a company working on issues of epidemiology and pharmacoepidemiology for various companies. N.M. declares no other relevant conflict of interest. S.P.G., R.A., G.C., M.L. and N.M. or their institutions received compensation from Orion Pharma for participation in the steering group for this study.
In remembrance of our dear colleague Riku Aantaa, investigator and steering group member, who passed away before publication of this manuscript. Professor Corinne de‐Vries contributed to study design and oversight as Chair of the steering group until joining the EMA in 2012. Peter Hughes (Peter Hughes Associates) assisted with the first version of the manuscript on behalf of Orion Pharma. The results presented in this article were previously presented at the ISPOR 18th Annual European Congress 34 , at the 31st International Conference on Pharmacoepidemiology and Therapeutic Risk Management 35 , and at the 28th ESICM (European Society of Intensive Care Medicine) Lives Congress, Berlin, October 2015 .
Contributors
C.G. drafted the manuscript, and contributed to study design and coordination, and interpretation of the results. M.W. contributed to study design and coordination, and interpretation of the results. P.P. contributed to study design and performed data analysis. R.A., G.C., N.M. and S.P.‐G. contributed to study design and oversight, and interpretation of the results. M.L. contributed to study oversight and interpretation of the results. All authors reviewed and approved the final manuscript.
Supporting information
Figure S1 Administration of dexmedetomidine by month and by country
Figure S2 Hierarchical analysis of off‐label administrations of dexmedetomidine
Table S1 Reasons for initiating dexmedetomidine sedation in the intensive care unit
Table S2 Summary of dexmedetomidine use that deviates from the Summary of Product Characteristics recommendations
Steering group members
Dr Susana Perez‐Gutthann (Barcelona, Spain) (Chair); Prof Riku Aantaa (Turku, Finland); Prof Giorgio Conti (Rome, Italy); Prof Nicholas Moore (Bordeaux, France); Dr Michael Lewis (Berlin, Germany).
Site principal investigators
Dr Christopher Adlbrecht, Medical University, Vienna Hospital Association, Vienna (Austria Coordinating Investigator); Dr Michael Joannidis, Medical University, Innsbruck, Austria; Prof Rudolf Likar, LKH Klagenfurt, Austria; Prof Esko Ruokonen, Kuopio University Hospital, Kuopio, Finland (Finland Coordinating Investigator); Dr Seppo Hovilehto, South Karelia Central Hospital Lappeenranta, Finland; Dr Sanna Vilo, Turku University Hospital, Turku, Finland; Dr Pekka Loisa, Päijät‐Häme Central Hospital, Lahti, Finland; Dr Sari Karlsson, Tampere University Hospital, Tampere, Finland; Dr Didier Keh, Prof Andreas Meisel, Dr Oliver Haase, Charité University Hospital, Berlin, Germany; Dr Beate Sedemund‐Adib, Lubeck University Hospital, Lubeck, Germany; Prof Rebecca Von Haken, Heidelberg University Hospital, Heidelberg, Germany; Dr Andreas Koczulla; Marburg University Hospital, Marburg, Germany; Dr Wiktor Sułkowski, General Hospital, Ostrów Mazowiecka, Poland; Dr Maciej Żukowski, Public Clinical Hospital No. 2, Szczecin, Poland; Dr Dariusz Onichimowski, Voivodal Hospital, Olsztyn, Poland; Prof Maria Wujtewicz, University Hospital, Gdansk, Poland.
Weatherall, M. , Aantaa, R. , Conti, G. , Garratt, C. , Pohjanjousi, P. , Lewis, M. A. , Moore, N. , and Perez‐Gutthann, S. (2017) A multinational, drug utilization study to investigate the use of dexmedetomidine (Dexdor®) in clinical practice in the EU. Br J Clin Pharmacol, 83: 2066–2076. doi: 10.1111/bcp.13293.
Trial registration: EU PAS Register (ENCEPP/SDPP/3243)
References
- 1. Southan C, Sharman JL, Benson HE, Faccenda E, Pawson AJ, Alexander SP, et al. The IUPHAR/BPS Guide to PHARMACOLOGY in 2016: towards curated quantitative interactions between 1300 protein targets and 6000 ligands. Nucl Acids Res 2016; 44 (Database Issue): D1054–D1068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Alexander SPH, Davenport AP, Kelly E, Marrion N, Peters JA, Benson HE, et al. The Concise Guide to PHARMACOLOGY 2015/16: G protein‐coupled receptors. Br J Pharmacol 2015; 172: 5744–5869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Flacke JW. Alpha‐2‐adrenergic agonists in cardiovascular anesthesia. J Cardiothorac Vasc Anesth 1992; 6: 344–359. [DOI] [PubMed] [Google Scholar]
- 4. Callado LF, Stamford JA. Alpha‐2A but not alpha‐2B/C adrenoceptors modulate noradrenaline release in rat locus coeruleus: voltammetric data. Eur J Pharmacol 1999; 366: 35–39. [DOI] [PubMed] [Google Scholar]
- 5. Jakob SM, Ruokonen E, Grounds RM, Sarapohja T, Garratt C, Pocock SJ, et al. Dexmedetomidine for Long‐Term Sedation Investigators . Dexmedetomidine vs. midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials. JAMA 2012; 307: 1151–1160. [DOI] [PubMed] [Google Scholar]
- 6. Pandharipande PP, Pun BT, Herr DL, Maze M, Girard TD, Miller RR, et al. Effect of sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically ventilated patients: the MENDS randomized controlled trial. JAMA 2007; 298: 2644–2653. [DOI] [PubMed] [Google Scholar]
- 7. Riker RR, Shehabi Y, Bokesch PM, Ceraso D, Wisemandle W, Koura F, et al. SEDCOM (Safety and Efficacy of Dexmedetomidine Compared With Midazolam) Study Group . Dexmedetomidine vs. midazolam for sedation of critically ill patients: a randomized trial. JAMA 2009; 301: 489–499. [DOI] [PubMed] [Google Scholar]
- 8. Jones CR. Perioperative uses of dexmedetomidine. Int Anesthesiol Clin 2013; 51: 81–96. [DOI] [PubMed] [Google Scholar]
- 9. Piao G, Wu J. Systematic assessment of dexmedetomidine as an anesthetic agent: a meta‐analysis of randomized controlled trials. Arch Med Sci 2014; 10: 19–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Mahmoud M, Mason KP. Dexmedetomidine: review, update, and future considerations of paediatric perioperative and periprocedural applications and limitations. Br J Anaesth 2015; 115: 171–182. [DOI] [PubMed] [Google Scholar]
- 11. Tobias JD. Dexmedetomidine: applications in pediatric critical care and pediatric anesthesiology. Pediatr Crit Care Med 2007; 8: 115–131. [DOI] [PubMed] [Google Scholar]
- 12. Iirola T, Vilo S, Manner T, Aantaa R, Lahtinen M, Scheinin M, et al. Bioavailability of dexmedetomidine after intranasal administration. Eur J Clin Pharmacol 2011; 67: 825–831. [DOI] [PubMed] [Google Scholar]
- 13. Tug A, Hanci A, Turk HS, Avbey F, Isil CT, Savin P, et al. Comparison of two different intranasal doses of dexmedetomidine in children for magnetic resonance imaging sedation. Paediatr Drugs 2015; 17: 479–485. [DOI] [PubMed] [Google Scholar]
- 14. Hilliard N, Brown S, Mitchinson S. A case report of dexmedetomidine used to treat intractable pain and delirium in a tertiary palliative care unit. Palliat Med 2015; 29: 278–281. [DOI] [PubMed] [Google Scholar]
- 15. Cimen ZS, Hanci A, Sivrikaya GU, Kilinc LT, Erol MK. Comparison of buccal and nasal dexmedetomidine premedication for pediatric patients. Paediatr Anaesth 2013; 23: 134–138. [DOI] [PubMed] [Google Scholar]
- 16. Abdallah FW, Brull R. Facilitatory effects of perineural dexmedetomidine on neuraxial and peripheral nerve block: a systematic review and meta‐analysis. Br J Anaesth 2013; 110: 915–925. [DOI] [PubMed] [Google Scholar]
- 17. Naithani U, Meena MS, Gupta S, Meena K, Swain L, Pradeep DS. Dose‐dependent effect of intrathecal dexmedetomidine on isobaric ropivacaine in spinal anesthesia for abdominal hysterectomy: effect on block characteristics and hemodynamics. J Anaesthesiol Clin Pharmacol 2015; 31: 72–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Guidelines for good pharmacoepidemiology practices [GPP]. Pharmacoepidemiol Drug Saf 2008; 17: 200–208. [DOI] [PubMed] [Google Scholar]
- 19. European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP) . Guide on methodological standards in pharmacoepidemiology [online]. Available at http://www.encepp.eu/standards_and_guidances/methodologicalGuide.shtml (last accessed 20 April 2017).
- 20. Guideline on good pharmacovigilance practices (GVP) module VIII – post‐authorisation safety studies [online]. Available at: http://www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/news/2012/06/news_detail_001546.jsp&mid=WC0b01ac058004d5c1 (last accessed 20 April 2017).
- 21. Poh YN, Poh PF, Buang SN, Lee JH. Sedation guidelines, protocols, and algorithms in PICUs: a systematic review. Pediatr Crit Care Med 2014; 15: 885–892. [DOI] [PubMed] [Google Scholar]
- 22. Plambech MZ, Afshari A. Dexmedetomidine in the pediatric population: a review. Minerva Anestesiol 2015; 81: 320–332. [PubMed] [Google Scholar]
- 23. Mason KP, Lerman J. Dexmedetomidine in children: current knowledge and future applications. Anesth Analg 2011; 113: 1129–1142. [DOI] [PubMed] [Google Scholar]
- 24. Wu Y, Zhang Y, Hu X, Qian C, Zhou Y, Xie J. A comparison of propofol vs. dexmedetomidine for sedation, haemodynamic control and satisfaction, during esophagogastroduodenoscopy under conscious sedation. J Clin Pharm Ther 2015; 40: 419–425. [DOI] [PubMed] [Google Scholar]
- 25. Arcangeli A, D'Alo C, Gaspari R. Dexmedetomidine use in general anaesthesia. Curr Drug Targets 2009; 10: 687–695. [DOI] [PubMed] [Google Scholar]
- 26. Diprivan 1% summary of product characteristics [online]. Available at https://www.medicines.org.uk/emc/medicine/2275 (last accessed 20 April 2017).
- 27. Hypnovel 10 mg/2 ml solution for injection summary of product characteristics [online]. Available at https://www.medicines.org.uk/emc/medicine/1692 (last accessed 20 April 2017).
- 28. Dasta J, Kane‐Gill S, Durtschi A. Comparing dexmedetomidine prescribing patterns and safety in the naturalistic setting versus published data. Ann Pharmacother 2004; 38: 1130–1135. [DOI] [PubMed] [Google Scholar]
- 29. Vilo S, Rautiainen P, Kaisti K, Aantaa R, Scheinin M, Manner T, et al. Pharmacokinetics of intravenous dexmedetomidine in children under 11 yr of age. Br J Anaesth 2008; 100: 697–700. [DOI] [PubMed] [Google Scholar]
- 30. Potts AL, Anderson BJ, Warman GR, Lerman J, Diaz SM, Vilo S. Dexmedetomidine pharmacokinetics in pediatric intensive care – a pooled analysis. Paediatr Anaesth 2009; 19: 1119–1129. [DOI] [PubMed] [Google Scholar]
- 31. Prieto L, Spooner A, Hidalgo‐Simon A, Rubino A, Kurz X, Arlett P. Evaluation of the effectiveness of risk minimization measures. Pharmacoepidemiol Drug Saf 2012; 21: 896–899. [DOI] [PubMed] [Google Scholar]
- 32. Gridchyna I, Cloutier A‐M, Nkeng L, Craig C, Frise S, Moride Y. Methodological gaps in the assessment of risk minimization interventions: a systematic review. Pharmacoepidemiol Drug Saf 2014; 23: 572–579. [DOI] [PubMed] [Google Scholar]
- 33.ENCePP study search page available at: http://www.encepp.eu/encepp/studySearch.htm;jsessionid=Js1HZ9I0PIXssxqzREjGzH_Y‐LpkwDjCfe_ShRFG3u4RVipv6QEy!1417383149 searched (last accessed 16 Feb 2017).
- 34. Stein D, Weatherall M, Garratt C, Aantaa R, Conti G, Lewis M, et al Methodological considerations for the implementation of a European mandated retrospective drug utilisation study (DUS) to investigate the use of dexmedetomidine (Dexdor®) in clinical practice. Value Health 2015; 18: A723 (Poster presentation at ISPOR 18th Annual European Congress, November 2015.
- 35. Perez‐Gutthann S, Weatherall M, Garratt C, Pohjanjousi P, Aantaa R, Conti G, et al A multinational, drug utilisation study to investigate the use of dexmedetomidine (Dexdor®) in clinical practice in The EU. Pharmacoepidemiol Drug Saf 2015; 24(S1): 95–6. (Poster presentation at 31st International Conference on Pharmacoepidemiology and Therapeutic Risk Management, Boston, MA, USA, August 2015).
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1 Administration of dexmedetomidine by month and by country
Figure S2 Hierarchical analysis of off‐label administrations of dexmedetomidine
Table S1 Reasons for initiating dexmedetomidine sedation in the intensive care unit
Table S2 Summary of dexmedetomidine use that deviates from the Summary of Product Characteristics recommendations