

Abstract
Life-space is a promising method for estimating older adults’ functional status. However, traditional life-space measures are costly and time consuming because they often rely on active subject participation. This study assesses the feasibility of using the global positioning system (GPS) function of smart phones to generate life-space indicators. We first evaluated the location accuracy of smart phone collected GPS points versus those acquired by a commercial GPS unit. We then assessed the specificity of the smart phone processed life-space information against the traditional diary method. Our results suggested comparable location accuracy between the smart phone and the standard GPS unit in most outdoor situations. In addition, the smart phone method revealed more comprehensive life-space information than the diary method, which leads to higher and more consistent life-space scores. We conclude that the smart phone method is more reliable than traditional methods for measuring life-space. Further improvements will be required to develop a robust application of this method that is suitable for health-related practices.
Keywords: life-space, GPS, smart phone, activity space, functional status, mobility, GIS
Introduction
The proportion of older adults in the developed and developing world continues to increase, which has raised growing concerns about maintaining or improving individual health status while simultaneously minimizing health-related expenditures (Deaton, 2008). Public health and medical professionals will need high-quality health indicators to accomplish both of these tasks. Functional limitations or abilities to perform activities of daily living (ADLs) and/or instrumental activities of daily living (IADLs) represent an important dimension of older adults’ health status (Ferrucci et al, 2004; Katz and Stroud, 1989). While many survey instruments adequately measure ADLs and IADLs, most instruments do not provide continuous and objective measures of walking, shopping or other activities that correspond to older persons’ physical activities. More precise measures of these functional tasks will have a great impact on the development of therapies and interventions to improve older individuals’ health. For example, as health practitioners move from providing patients with general instructions promoting physical activities to providing patients with precise prescriptions to improve functional status, more objective and continuous measures that profile older persons’ daily activities are needed (e.g., Boyle et al, 2010; Peel et al, 2005). One promising measure that has these desirable properties is life-space.
Life-space refers to individuals’ general spatial ranges of activities during a specific period (May et al, 1985). While the concept of activity space can be traced back to retail geography (Huff, 1960), the life-space concept was developed in the context of older adults (May, 1985; Peel et al, 2005). Life-space characteristics have been proved effective in depicting individual functional status (May, 1985; Peel et al, 2005) and have been associated with health problems such as mobility (Baker et al, 2003; Peel et al, 2005) and mortality (Boyle et al, 2010). However, providing an accurate portrait of life-space can be taxing, as it requires complete and detailed data about people’s daily activities. Researchers have relied primarily on activity questionnaires and diaries for data collection. Typically, an activity questionnaire asks individuals about time, type, and geographic locations of their activities during a predefined period of time (e.g., two weeks). Likewise, activity diaries require participants to take a notebook with them and write down any activity of interest during the study period. Space-time information gathered from these methods is then used to generate single or multiple indicators reflecting life-space.
Although the survey and diary methods are straightforward, they both have a number of limitations. First, both methods require active individual participation that may be perceived as intrusive. For example, writing activity diaries is time consuming and attention intensive, and may present extra burden to participants’ regular lives (Stalvey et al, 1999). Recruiting subjects to receive questionnaires can be costly. Second, both methods can pose accuracy problems as they document only a limited number of activities for a continuum of daily activities over geographic space. Participants may pick and choose what to write in the diary method, while the accuracy of the questionnaire method depends on the memory of participants and the mode of questionnaires (Craik and McDowd 1987; Bowling 2005). Third, both methods have a time lag that makes it unrealistic for clinicians to monitor patients’ life-space activities and to design interventions in a timely manner.
Noticing these limitations, Schenk et al. (2011) and Tung et al. (2011) independently proposed using smart phones to measure activity and life-space of community-dwelling adults. Specifically, they used the embedded accelerometers and global positioning system (GPS) chips of cell phones to monitor individual physical activities and corresponding geographic locations. Cell phone based data acquisition can overcome limitations associated with collecting life-space data by recording people’s locations within the community in a nonintrusive, continuous, near real time manner. Running one or more applications on a subject’s own smart phone allows them to forgo carrying extra devices for data collection. In addition, using the subject’s smart phone (or providing a subsidy for an inexpensive smart phone) costs much less than traditional data collection approaches. While both studies indicated that this approach is technologically capable of capturing important spatial-temporal characteristics of life-space and physical activities, most location-based questions such as location accuracy and spatial zone visiting frequency have not been assessed. In order to be used for clinical intervention, it is necessary to further assess the feasibility of cell phone deployment in two key aspects: (1) how accurate are cell phone locations compared to locations captured by commonly used GPS devices, and (2) what are the relative advantages and shortcomings of the cell phone method compared to traditional data collection instruments in life-space measurement. Answering these questions will enhance measurements of individual activity and location for ultimate classification into highly textured representations of individual functional status.
The primary aim of this study was to evaluate the feasibility of cell phone GPS data in measuring life-space. Specifically, we first assessed the location accuracy of cell phone GPS points by comparing them to those captured by a commercial, “gold standard” GPS unit. We then evaluated the completeness and specificity of cell-phone collected life-space data against diary documented life-space data.
Materials and Methods
Equipment
We used Nokia N79 cell phones to collect life-space data. Using custom-written PyS60 code running in the background of the Symbian S60 operating system, this phone was set to record information of longitude and latitude at a 1-minute interval with the built-in GPS chipset. Assisted-GPS services (i.e., location determination based on both GPS satellite and cell-phone tower information) were not used.
Positional Accuracy Validation
In order to obtain valid life-space information, the accuracy of cell phone obtained points must be high enough to determine an individual’s approximate location, such as at home, in the neighborhood, in town, and out of town. Generally, previous studies used commercial GPS units instead of cell-phone GPS to collect location information (e.g. Garmin 60 series GPS to measure physical activities in subjects with peripheral artery disease, Le Faucheur et al, 2008). To evaluate if cell-phone GPS could attain comparable location accuracy to commercial GPS units, we assessed the accuracy of the Nokia N79 phone head-to-head against a “gold standard” Garmin 60 series GPS unit. The measurement was implemented within a 2-week period in September 2011. Four investigators were first trained together so that they would all follow the same procedure: (1) recording descriptive information (in shade, against a wall, in open space, etc.) about a location while holding both the GPS unit and the cell phone in their hands, (2) letting the GPS unit settle for at least 2 minutes to stabilize GPS signals (which also allowed the investigator to document descriptive information), (3) recording the readings of coordinates and timestamp for both devices. The time settings of all devices were calibrated before measurement.
Three of the four investigators visited multiple outdoor locations around the Omaha-Lincoln metropolitan area of Nebraska and its outlying rural areas. One investigator visited multiple outdoor locations around the Evanston-Chicago metropolitan area of Illinois. We included the Evanston-Chicago area because it has one of the world’s densest concentrations of skyscrapers and infrastructure, and thus provides a better test of system performance in a highly shaded region than would be possible in the Omaha-Lincoln area. At each location, photographs were taken to provide landmarks required to replicate the measurement if necessary. Location accuracy was measured in Euclidean distance between cell phone points and Garmin points. Figure 1 shows all visited points of the two areas.
Figure 1. Point locations of the accuracy assessment.
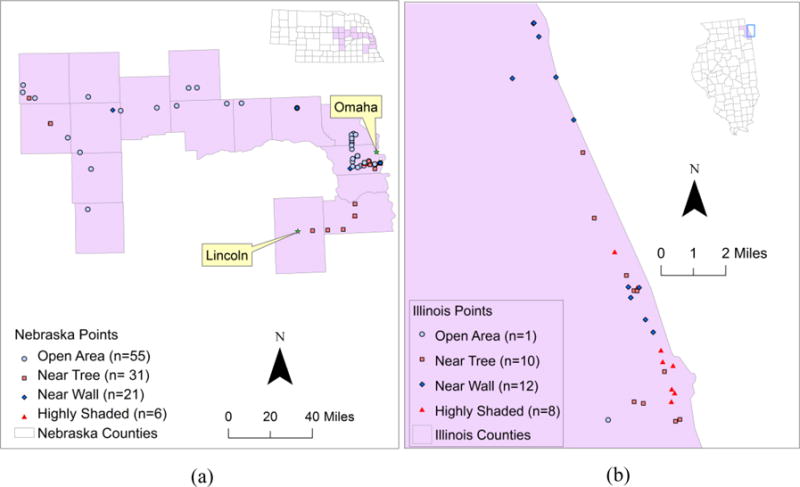
(a). Omaha-Lincoln metropolitan and surrounding rural areas. Data collected by three investigators over a two-week period. (b). Evanston-Chicago metropolitan area. Data collected by a single investigator over the same two-week period as (a). Note the significant difference in scale between (a) and (b).
We first attempted to group Garmin GPS versus cell-phone GPS location comparisons into rural, suburban, and urban areas, and found the differences in mean distances were not significant. We found that the main contributor to location differences was contextual or surrounding environment. Therefore, the contextual information was classified into four categories: open (i.e., no wall, tree, or other shading within 10 meters), wall shaded (i.e., wall within 10 meters), tree shaded (i.e., tree within 10 meters), and highly shaded (i.e., shaded by high buildings or dense canopies). As shown in Table 1, the average distance between Garmin and cell-phone GPS points was 16.1 meters (standard deviation (SD): 26.4). Relative to Garmin points, cell phone points are close in distance in open and tree-shaded areas but highly deviated in areas with a high level of shading (mean distance: 59.5, SD: 65.7). Since most points from Chicago were in highly shaded areas, the mean distance would be about 10 meters rather than 16 meters if the Chicago points were excluded.
Table 1.
Differences (in meters) of point locations measured by cell phone GPS and the Garmin GPS
| Min | Max | Mean | Standard deviation | |
|---|---|---|---|---|
| All points (n=144) | 0.5 | 266.6 | 16.1 | 26.4 |
| Open (n=56) | 0.5 | 47.3 | 9.7 | 9.6 |
| Tree shaded (n=41) | 0.6 | 34.3 | 9.5 | 7.8 |
| Wall shaded (n=33) | 0.8 | 56.6 | 16.7 | 14.3 |
| Highly shaded (n=14) | 9.4 | 266.6 | 59.5 | 65.7 |
Data Collection
In order to evaluate the effectiveness of cell phone collected GPS data in capturing life-space characteristics, we enrolled 10 persons 75 years of age or older who were seen for primary care or enrolled in the Engage Wellness program at the Home Instead Center for Successful Aging at the University of Nebraska Medical Center. Exclusion criteria of subjects included cognitive impairment, major uncontrolled psychiatric or medical disease, significant functional limitations in ADL or IADL, and living in assisted living or higher-need housing. Participants were instructed on how to use and charge the cell phone and were able to demonstrate this knowledge to the investigator. Subjects were also given a small notepad and were instructed to jot down details describing all excursions from their home, including time and destination information. All subjects were asked to keep the phone and diary for a month and then return study materials to the investigators. The average number of days for subject observation was 25. All study data were collected under appropriate institutional review board approval and supervision.
After the subjects returned their cell phones and notepads, we converted the diary-recorded excursions into digital data and the GPS coordinates into 2-dimensional points in a geographic information system (GIS). Diary data were decoded into location specific information by 1) scanning all notepads, 2) converting notepad data into texts by one investigator, and being validated by another investigator, 3) verifying confusing hand written words by the attending physician, and 4) determining activity location based on GIS data. For excursions whose locations were indiscernible or not written, we used other written information (e.g., names of grocery stores), excursion history, and a land-use map to determine the exact locations. For GPS data, incorrect points due to the device limits and weak reception were excluded using a “cleaning” approach (Auld et al, 2009). Specifically, we first calculated subject speed by dividing the distance between two consecutive GPS points by their time difference. Then, points with a speed greater than 160km/hr were deemed invalid and deleted from subsequent analyses. The speed of the next point was recalculated accordingly. The cleaning process identified five invalid points (out of the total of 111,464 points collected by the ten subjects).
Life-space Validation Protocol
According to the literature, life-space can be calculated by dividing the space into six contingent zones, (i.e., bedroom, porch/patio, parking lot/yard, within the neighborhood, within town, and out of town) and assigning each zone a score ranging from 1 (bedroom zone) to 6 (outside-of-town zone; Barnes et al, 2007; Boyle et al, 2010). In this study, we combined the first three zones into a “home” zone because neither the GPS data (due to location accuracy) nor the notepad information (due to IRB restrictions) could effectively distinguish them. The home area was defined as a 50-meter buffer around the centroid of the subject’s house, and the neighborhood area was defined as between 50 meters and 805 meters (0.5 mile) from the house centroid (Taylor et al, 2012). The within the town zone was defined as between 805 meters and 8,047 meters (5 miles) from home, and the out of town zone was defined as further than 5 miles from home (Baker et al, 2003). The four zones were assigned a score of 1, 2, 3, and 4, respectively.
Both diary-based and GPS-based data were decoded into three indicators according to Baker et al. (2003): the maximum life-space (LS-M, defined as the score of the outmost zone the subject has reached), the simple life-space (LS-S, defined as the sum of scores of all zones the subject has reached), and the composite indicator (LS-C, defined as the sum of the multiplications of the zone score and the visiting frequency of the four zones). Although these indicators represent different aspects of life-space, the LS-C is more reflective of an individual’s life-space activities because it involves both visiting frequency and zone information. For the purpose of comparing cell phone data collection against diary methods, we used these traditional life-space indicators instead of developing new GPS based indicators. In addition, since the comparison was based on diary data, which does not have activity duration information, we opted not to calculate such information from GPS data.
For both GPS and diary data, Euclidean distance from home was used to allocate activities to life-space zones. For either method, if there was no entry for a specific day, all four zones were labeled “no data” for that day. If, on the other hand, at least one zone had some entries in a day, zone specific information was decoded into either a person-day (e.g., a person-day means this person has visited this zone on this day) or “not found” (e.g., the data does not indicate that the person has visited this zone) for that day. For the diary method, if there is a zone-specific entry for a day, then one person-day for that zone was confirmed; otherwise, a zone-specific person-day was labeled “not found”. For the GPS method, if two or more consecutive points in a zone were recorded, a zone specific person-day was registered; otherwise, a zone-specific person-day was labeled “not found”. Then, for each method, the visiting frequency for a zone was calculated as the sum of person-days for that zone.
After deriving LS-M, LS-S, and LS-C indicators from both methods, we compared the consistency of these indicators between the two methods. Since GPS location accuracy may influence the accuracy of zone-visiting counts and life-space indicators, we performed a sensitivity analysis by constructing a 20-meter buffer area around each zone boundary. We set the buffer width to 20 meters because, according to a previous assessment (Wing et al, 1995), the location accuracy of consumer GPS units could attain under 10 meters in open or tree-shaded areas (e.g., neighborhood and town boundary). We removed the points within these buffers and recalculated the zone-visit numbers and life-space indicators. There were no differences in life-space metrics calculated with or without the 20-meter buffer zone, suggesting that our approach was robust.
Results
Comparison of zone-visiting information
Table 2 shows zone-specific person-days by the two methods. For each zone-specific cross-tabulation, the number in each cell represents the number of person-days that fulfill the categories of the two methods. For example, in the upper-left home zone cross-tabulation, the cell intersected the “Home” row and the “Home” column had 151 person-days by both methods. Moving one cell down, 43 is the number of person-days that subject was found in the home zone by cell phone GPS but not by diary. Moving down further, 18 person-days without home zone diary entries (no data) were signaled by cell phones for the home zone. One can similarly move column wise to identify missing zone specific (not found) and entire-day information (no data) by GPS. If we combine the person-days of all zones, the cell phone method revealed 615 (212+178+154+71) person-days among all zones, while the diary method revealed 432 (172+27+163+70) person-days.
Table 2.
Zone-specific visiting cross-tabulations between the diary and cell phone methods
| Phone | Home* | Not found | No data | Sum | Phone | Neighborhood* | Not found | No data | Sum |
|---|---|---|---|---|---|---|---|---|---|
| Diary | Diary | ||||||||
| Home | 151 | 2 | 19 | 172 | Neighborhood | 19 | 6 | 2 | 27 |
| Not found | 43 | 3 | 3 | 49 | Not found | 140 | 34 | 20 | 194 |
| No data | 18 | 1 | 8 | 27 | No data | 19 | 0 | 8 | 27 |
| Sum | 212 | 6 | 30 | 248 | Sum | 178 | 40 | 30 | 248 |
| Phone | Within Town* | Not found | No data | Sum | Phone | Out of Town* | Not found | No data | Sum |
|---|---|---|---|---|---|---|---|---|---|
| Diary | Diary | ||||||||
| Within Town | 116 | 28 | 19 | 163 | Out of Town | 46 | 20 | 4 | 70 |
| Not found | 24 | 31 | 3 | 58 | Not found | 19 | 114 | 18 | 151 |
| No data | 14 | 5 | 8 | 27 | No data | 6 | 13 | 8 | 27 |
| Sum | 154 | 64 | 30 | 248 | Sum | 71 | 147 | 30 | 248 |
Home zone was defined as the buffer area of 50 meters from the house centroid; neighborhood zone was defined as between 50 meters and 805 meters from the house centroid; town zone was defined as between 805 and 8,047 meters (5 miles) from the house centroid; and out-of-town zone was defined as the area more than 8,047 meters from the house
Several patterns can be observed in the zone-specific cross-tabulation. First, both cell phone and diary methods show high frequencies of home-zone (212 person-days for cell phone versus 172 for diary). If we use the diary as the reference, 151 (or 88%) of 172 person-days can be found in cell phone records. In addition, cell phone records added 61 more home-zone person-days when there were no diary records either because they were not found (n=43) or there was no data (n=18).
Second, the neighborhood zone, which covers 50 to 805 meters from the house centroid, showed the largest discrepancy between the two methods. There were only 27 person-days in the neighborhood zone noted by the diary method, whereas the GPS method indicated 178 person-days in this zone. In contrast, there were 194 “not found” neighborhood entries from diary data even though there were some other entries on the day, which suggests subjects tend to ignore or forget to record neighborhood activities in the diary. This finding implies the increased behavioral cost of logging frequently performed, relatively trivial activities, such as picking up newspapers for a neighbor across the street (Elliott and Clark, 1978).
Finally, the two methods were comparable in terms of zone-specific encounters for zones 3 (within town) and 4 (out of town). The within-town zone had similar numbers between the two methods in zone activities (154 person-days for cell phones versus 163 for diary). It should also be noted that 151 missing (i.e., not found) zone-specific diary entries suggests that people may have ignored grocery shopping trips in the within-town zone, as they are seen as routine or inconsequential. Although the out-of-town zone had similar numbers of activities recorded by the two methods (71 person-days from cell phones versus 70 from diaries), only 46 were matched. Most of the inconsistencies were caused by “not found” or no zone-specific entry for a diary or no GPS signal reception for a part of a day, while having other zone-specific entries and GPS signals for other parts of the day.
Comparison of Life-space Indicators
The results of life-space indicators were broadly consistent between the two methods (Table 3). For these healthy older adult participants, both cell phone and diary methods consistently registered high life-space scores. Scores derived from cell phones for LS-Ms and LS-Ss were either equivalent or greater than those from diary records. In addition, GPS data revealed higher LS-Cs than diary data for most subjects. This difference is attributed to the higher frequency scores (i.e., the number of days a subject had visited a specific zone) from the GPS data. Three subjects had lower GPS LS-Cs than diary LS-Cs. Further examination of the GPS data indicates that their lower LS-Cs were due to the number of entire days without data rather than to lack of zone-specific information for a day.
Table 3.
Life-space indicators derived from diary data and GPS
| Subject # | LS-M* | LS-S* | LS-C* | |||
|---|---|---|---|---|---|---|
| Diary | GPS | Diary | GPS | Diary | GPS | |
| 1 | 4 | 4 | 10 | 10 | 135 | 108 |
| 2 | 3 | 4 | 6 | 10 | 48 | 126 |
| 3 | 4 | 4 | 8 | 10 | 70 | 111 |
| 4 | 4 | 4 | 8 | 10 | 108 | 129 |
| 5 | 4 | 4 | 10 | 10 | 78 | 66 |
| 6 | 4 | 4 | 10 | 10 | 26 | 26 |
| 7 | 4 | 4 | 8 | 10 | 110 | 182 |
| 8 | 4 | 4 | 10 | 10 | 192 | 253 |
| 9 | 4 | 4 | 10 | 10 | 227 | 222 |
| 10 | 4 | 4 | 10 | 10 | 54 | 86 |
LS-M: maximum life-space; LS-S: simple life-space score; LS-C: composite life-space score
Discussion
This paper assessed an inexpensive smart phone for generating life-space indicators for potential clinical interventions. The assessment was implemented in two aspects: (1) location accuracy compared to a common GPS device and (2) reliability and specificity of cell phone-generated life-space indicators compared to diary-generated indicators. Our assessment suggests that geographic locations measured by a cell phone deviate from those measured by the commercial GPS by about 15 meters without any locating support from the phone carrier. Since life-space is generally measured in zones that include home, neighborhood, in town, and out of town, 15 meter uncertainty in spatial resolution had almost no empirical effect on our assessment. In addition, cell phone data revealed more comprehensive life-space information than diary-recorded life-space zone incidence, especially in the neighborhood zone where older adult subjects tend to forget or ignore their activities.
Since the cell phone method provides more frequent and persistent location information, it is likely to reflect greater life-space variation in a short period of time than the diary method. However, as the data collection period gets longer, a person is more likely to hit outer life-space, which explains why the two methods generated similar LS-Ms and LS-Ss during the study period.
This work suggests that cell phone measured life-space is both accurate and valid and may be particularly well-suited for future studies measuring life-space in independent, community-dwelling individuals. Smart phones are popular, ubiquitous, and well suited for downloading simple applications. In addition, smart phones offer many ways for health care providers to directly communicate with patients, including voice calls, message texting, video presentations, and games (Burns et al, 2011, Favela et al, 2004). They are thus feasible and viable devices for clinical interventions based on life-space properties.
However, two concerns will need to be addressed in real-world deployments. First, people may forget to carry a dedicated research-only cell phone. Using the subject’s own smart phone will improve adherence but will not fully eliminate “missing data” problems. However, the potential to collect data over prolonged observational periods (e.g., six months) makes the missing data problem more tractable. Second, power consumption associated with location coordinate sampling leads to missing data, both from poorer adherence (e.g., failed to charge the phone daily) and from running out of power at inopportune moments. We suspect that much of the zone location information that was reported as “data missing” or “not indicated” was due to the smart phone’s battery depletion. Advances in signal dynamic sampling, battery technology, and ubiquitous charging approaches have the potential to significantly ameliorate, but not completely eliminate this issue.
Another issue that was not directly addressed in this study is the decoding of cell phone location information. Under the assumption that a 2-minute duration is sufficient for a person to show physical presence, we used the presence of a 2-minute or more duration in each zone as an excursion indicator. However, cell phone-collected locations are without a qualifier, such as an excursion to a drug store or supermarket. We decoded location information into zone-related activities by location inference from diaries or spatial inference from GPS. If cell phone location accuracy were within 10 meters, we would be able to tag the location to a store or facility. Since the accuracy level was greater than 15 meters, the GIS-based tagging strategy may not work. For this reason, future work is needed to develop algorithms that combine duration-based zone information with facility location information so that one can reasonably qualify a subject’s activity as being shopping, visiting a doctor, etc. This qualified activity information can then be used to judge individual functional status in the context of life-space in a manner similar to the trip purpose qualifiers used in survey and diary methods (Allman et al, 2004; Brown et al, 2009). If the above procedure cannot determine the excursion purpose, additional location queries such as the web-prompted survey could be used (Auld et al, 2009).
Although the cell phone method has obvious advantages in collecting life-space information, some issues need to be considered in its future applications. First, the classification of life-space zones could be more flexible. In this study, we used a simple zone boundary according to previous studies (Baker et al, 2003; Taylor et al, 2011). Obviously this scheme cannot be applied in all situations. In addition to distance from home, zone boundaries are also influenced by other place-dependent characteristics such as rural/urban status, population density, built infrastructure, economic status, etc. For example, the town zone could be larger for urban dwellers than for rural residents; since GPS accuracy is lower in high shielding areas, the home zone of urban residents may also be set to be greater than 50 meters. These factors should be fully considered when defining life-space boundaries which can directly influence the calculation of life-space indicators. A second issue involves how to transform activity frequency information collected by the cell-phone method into a representation of space activeness. Generally, the outer physical boundary defines life-space, but the frequencies of activity in each zone define space or zone activeness (Newsome et al, 1998). Compared to life-space, space activeness can eliminate “data noises” (e.g., rare visits to far-away locations) and derive more stable and smoothed spatial boundaries (Sherman et al, 2005). Presenting space activeness requires adjusting (or rescaling) the sharp contrast of point density between frequent locations (e.g., home, work place) and infrequent locations (e.g., peripheral areas of the space). Third, it is even more challenging to qualify space activeness, because there has not been a mature classification algorithm which can use point location, collection time, and land use information to differentiate whether a point indicates driving, walking, jogging, or other activities (Vazquez-Prokopec et al, 2009). Although combining GPS data with accelerometer data is promising in revealing individual activities (Schenk et al, 2011; Tung et al, 2011), more algorithms are needed to effectively integrate the two data streams. Finally, since smart-phones are usually not user-friendly to older people, our deployment strategy needs to be further refined to avoid data missing, a major problem of the current study.
In conclusion, we have shown that GPS-enabled cell phones provide accurate and valid life-space measurements. The study not only develops several protocols for spatial data acquisition and classification, but also demonstrates the viability and feasibility of using cell phones to measure an individual’s functional status in a continuous, noninvasive, and potentially scalable manner. Future studies should focus on the effective processing, classifying, and integrating of cell phone-based GPS data with other location-based service and activity data, so that the GPS-generated information not only captures life-space boundary, but also describes life-space activity.
Acknowledgments
Sponsors: SJB supported by NIH/NIA AG-031158, the Vada Kinman Oldfield Alzheimer’s Research Foundation, a technology innovation award from the UNeMed Corporation (a University of Nebraska technology transfer concern), and startup funds from the University of Nebraska. EHG supported by startup funds from Northwestern University. AKS supported by startup funds from Randolph College. Ge Lin supported by NSF SES-07-52019 and a subcontract from The Highway Traffic Safety Administration Award 408-11-14.
Other: We thank Carrie A. Hoarty, M.D., Nicole Vanosdel, M.S., and Janelle Jacobson, MPH., for assistance with data collection. We greatly thank all the research subjects who participated in this study.
Footnotes
Conflicts of interest: The authors identify no conflicts of interest in this work.
Author contributions: Mobile monitoring technology developed by SJB, AKS, EHG. Mobile monitoring technical support provided by BCW and MPH. Life-space subject enrollment and data collection performed by JW, SJB. GPS validation by GL, NW, SJB, EHG. Data analysis and interpretation by GL, NW, WQ, SJB. Manuscript preparation by NW, GL, SJB, AKS.
References
- Allman R, Baker P, Maisiak R, Sims R, Roseman J. Racial similarities and differences in predictors of mobility change over eighteen months. Journal of General Internal Medicine. 2004;19:1118–1126. doi: 10.1111/j.1525-1497.2004.30239.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Auld J, Williams C, Mohammadian K, Nelson P. An automated GPS-based prompted recall survey with learning algorithms. Transportation Letters: the International Journal of Transportation Research. 2009;1:59–79. [Google Scholar]
- Baker S, Bodner V, Allman M. Measuring life-space mobility in community-dwelling older adults. Journal of the American Geriatric Society. 2003;51:1610–1614. doi: 10.1046/j.1532-5415.2003.51512.x. [DOI] [PubMed] [Google Scholar]
- Barnes L, Bienias L, Mendes de Leon F, Kim N. Correlates of life-space in a volunteer cohort of older adults. Experimental Aging Research. 2007;33:77–93. doi: 10.1080/03610730601006420. [DOI] [PubMed] [Google Scholar]
- Bowling A. Mode of questionnaire administration can have serious effects on data quality. Journal of Public Health. 2005;27:281–291. doi: 10.1093/pubmed/fdi031. [DOI] [PubMed] [Google Scholar]
- Boyle A, Buchman S, Barnes L, James D, Bennett A. Association between life-space and risk of mortality in advanced age. Journal of the American Geriatric Society. 2010;58:1925–1930. doi: 10.1111/j.1532-5415.2010.03058.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown C, Roth D, Allman R, Sawye P, Ritchie C, Roseman J. Trajectories of life-space mobility after hospitalization. Annals of Internal Medicine. 2009;150:372–378. doi: 10.7326/0003-4819-150-6-200903170-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burns N, Begale M, Duffecy J, Gergle D, Karr J, Giangrande E, Mohr C. Harnessing context sensing to develop a mobile intervention for depression. Journal of Medical Internet Research. 2011;13:e55. doi: 10.2196/jmir.1838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Craik I, McDowd M. Age differences in recall and recognition. Journal of Experimental Psychology: Learning, Memory, and Cognition. 1987;13:474–479. [Google Scholar]
- Deaton A. Income, health and wellbeing around the world: evidence from the Gallup World Poll. Journal of Economic Perspectives. 2008;22:53–72. doi: 10.1257/jep.22.2.53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elliott H, Clark S. The spatial context of urban activities: Some theoretical, methodological and policy considerations. In: Michelson W, editor. Public Policy in Temporal Perspective. The Hague: Mouton; 1978. [Google Scholar]
- Favela J, Rodriguez M, Preciado A, González VM. Integrating context-aware public displays into a mobile hospital information system. IEEE Transactions in Information Technology and Biomedicine. 2004;8:279–86. doi: 10.1109/titb.2004.834391. [DOI] [PubMed] [Google Scholar]
- Ferrucci L, Guralnik JM, Studenski S, Fried LP, Cutler GB, Walston JD. Designing randomized, controlled trials aimed at preventing or delaying functional decline and disability in frail, older persons: A consensus report. Journal of the American Geriatric Society. 2004;52:625–634. doi: 10.1111/j.1532-5415.2004.52174.x. [DOI] [PubMed] [Google Scholar]
- Huff DL. A Topographical Model of Consumer Space Preferences. Papers in Regional Science. 1960;6:159–17. [Google Scholar]
- Katz S, Stroud MW., III Functional assessment in geriatrics: a review of progress and directions. Journal of the American Geriatric Society. 1989;37:267–271. doi: 10.1111/j.1532-5415.1989.tb06820.x. [DOI] [PubMed] [Google Scholar]
- Le Faucheur A, Abraham P, Jaquinandi V, Bouye P, Saumet JL, Noury-Desvaux B. Measurement of walking distance and speed in patients with peripheral arterial disease: a novel method using a global positioning system. Circulation. 2008;117:897–904. doi: 10.1161/CIRCULATIONAHA.107.725994. [DOI] [PubMed] [Google Scholar]
- May D, Nayak US, Isaacs B. The life-space diary: A measure of mobility in old people at home. International Rehabilitation Medicine. 1985;7:182–186. doi: 10.3109/03790798509165993. [DOI] [PubMed] [Google Scholar]
- Newsome T, Walcott W, Smith P. Urban activity spaces: illustrations and application of a conceptual model for integrating the time and space dimensions. Transportation. 1998;25:357–377. [Google Scholar]
- Peel C, Sawyer Baker P, Roth DL, Brown CJ, Brodner EV, Allman RM. Assessing mobility in older adults: The UAB study of aging life-space assessment. Physical Therapy. 2005;85:1008–1119. [PubMed] [Google Scholar]
- Schenk AK, Witbrodt BC, Hoarty CA, Carlson RH, Goulding EH, Potter JF, Bonasera SJ. Cellular telephones measure activity and lifespace in community-dwelling adults: proof of principle. Journal of the American Geriatric Society. 2011;59:345–352. doi: 10.1111/j.1532-5415.2010.03267.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sherman J, Spencer J, Preisser J, Gesler W, Arcury T. A suite of methods for representing activity space in a healthcare accessibility study. International Journal of Health Geographics. 2005;4:e24. doi: 10.1186/1476-072X-4-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stalvey BT, Owsley C, Sloane ME, Ball K. The Life-space Questionnaire: a measure of the extent of mobility of older adults. Journal of Applied Gerontology. 1999;18:460–78. [Google Scholar]
- Taylor WC, Franzini L, Walker SNL, Poston C, Lin G. Walking Environmental Audits of Friendliness toward Physical Activity in Three Income Levels. Journal of Urban Health. 2011 doi: 10.1007/s11524-011-9663-5. (forthcoming) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tung JY, Semple JFL, Woo WX, Hsu WS, Sinn M, Roy EA, Poupart P. VALMA: Voice, Activity and Location Monitoring for Alzheimer’s Disease and Related Dementias. Annual Conference of the Rehabilitation Engineering and Assistive Technology Society of North America (RESNA); Toronto. 2011. [Google Scholar]
- Vazquez-Prokopec G, Stoddard ST, Paz-Soldan V, Morrison AC, Elder JP, Kochel TJ, Scott TW, Kitron U. Usefulness of commercially available GPS data-loggers for tracking human movement and exposure to dengue virus. International Journal of Health Geographics. 2009;8:e68. doi: 10.1186/1476-072X-8-68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wing M, Eklund A, Kellogg L. Consumer-grade global positioning system (GPS) accuracy and reliability. Journal of Forestry. 1995;103:169–173. [Google Scholar]