

Abstract
Background
Blood glucose control in the intensive care unit (ICU) has the potential to save lives. However, maintaining blood glucose concentrations within a chosen target range is difficult in clinical practice and holds risk of potentially harmful hypoglycemia. Clinically validated computer algorithms to guide insulin dosing by nurses have been advocated for better and safer blood glucose control.
Methods
We conducted an international, multicenter, randomized controlled trial involving 1550 adult, medical and surgical critically ill patients, requiring blood glucose control. Patients were randomly assigned to algorithm-guided blood glucose control (LOGIC-C, n = 777) or blood glucose control by trained nurses (Nurse-C, n = 773) during ICU stay, according to the local target range (80–110 mg/dL or 90–145 mg/dL). The primary outcome measure was the quality of blood glucose control, assessed by the glycemic penalty index (GPI), a measure that penalizes hypoglycemic and hyperglycemic deviations from the chosen target range. Incidence of severe hypoglycemia (<40 mg/dL) was the main safety outcome measure. New infections in ICU, duration of hospital stay, landmark 90-day mortality and quality of life were clinical safety outcome measures.
Results
The median GPI was lower in the LOGIC-C (10.8 IQR 6.2–16.1) than in the Nurse-C group (17.1 IQR 10.6–26.2) (P < 0.001). Mean blood glucose was 111 mg/dL (SD 15) in LOCIC-C versus 119 mg/dL (SD 21) in Nurse-C, whereas the median time-in-target range was 67.0% (IQR 52.1–80.1) in LOGIC-C versus 47.1% (IQR 28.1–65.0) in the Nurse-C group (both P < 0.001). The fraction of patients with severe hypoglycemia did not differ between LOGIC-C (0.9%) and Nurse-C (1.2%) (P = 0.6). The clinical safety outcomes did not differ between groups. The sampling interval was 2.3 h (SD 0.5) in the LOGIC-C group versus 3.0 h (SD 0.8) in the Nurse-C group (P < 0.001).
Conclusions
In a randomized controlled trial of a mixed critically ill patient population, the use of the LOGIC-Insulin blood glucose control algorithm, compared with blood glucose control by expert nurses, improved the quality of blood glucose control without increasing hypoglycemia.
Trial registration
ClinicalTrials.gov, NCT02056353. Registered on 4 February 2014.
Electronic supplementary material
The online version of this article (doi:10.1186/s13054-017-1799-6) contains supplementary material, which is available to authorized users.
Keywords: Blood glucose control, Computer algorithm, Quality of blood glucose control, Glycemic penalty index, Time-in-target, Sepsis, Infection
Background
Elevated blood glucose levels are very common in critically ill patients, independent of pre-existing diabetes mellitus. This hyperglycemia has been associated with an increased risk of morbidity and mortality [1]. Tight blood glucose control (BGC), targeting blood glucose levels below 110 mg/dL, improved the outcome of critically ill patients only in well-controlled single-center trials and in implementation studies [2–6]. In large multicenter trials, however, this beneficial effect was not reproduced and in the NICE-SUGAR trial mortality even increased in the intensive BGC group [7–9]. While excessive hyperglycemia above 180 mg/dL is no longer accepted, the target range for BGC is still controversial and variable [10]. The American Diabetes Association recommends targeting blood glucose levels below 180 mg/dL, while in Europe most centers use stricter target ranges (below 145 mg/dL), despite a lack of evidence [11, 12].
Excess mortality in patients undergoing BGC has been attributed to the increased incidence of hypoglycemia and unnecessary blood glucose variability [13, 14]. Inaccurate blood glucose measurements and the use of insulin dosing protocols that have not been clinically validated play an important role herein [15]. BGC requires not only frequent measurements of blood glucose, but also difficult calculations of the insulin doses, depending on the protocol. Moreover, BGC has to be done in severely ill patients, who may undergo rapid changes in their insulin sensitivity due to the underlying illness and medication such as parenteral nutrition and steroids. To obtain better (less hyperglycemia) and safer (less hypoglycemia) BGC it has been advocated to use computerized protocols for insulin dosing and timing of blood glucose measurements [16, 17]. However, the current evidence for these computer algorithms consists primarily of implementation studies or small randomized controlled studies [18–22]. Therefore, their use has not yet been widely adopted in general clinical practice although a growing number of ICUs are starting to use validated computer algorithms with a beneficial effect on blood glucose control, such as EndoTool and STAR [23, 24].
The LOGIC-Insulin algorithm, developed and based on the Leuven guideline and practice, had already been clinically validated in a single-center randomized trial, showing improved and safer BGC (below 110 mg/dL), compared to that performed by nurses who were highly experienced in BGC [25]. However, performance of the algorithm in a setting of different blood glucose target ranges, in a wide-ranging patient population, by nurses with less experience in BGC has not yet been evaluated in a pragmatic, multicenter setting. Therefore, we hypothesized that the LOGIC-Insulin algorithm improves the quality of BGC, in comparison with nurse-directed BGC, using two different glucose target ranges (80–110 mg/dL or 90–145 mg/dL) in a heterogeneous population of critically ill adults and in the setting of a nursing staff with variable levels of expertise.
Methods
Study design
We conducted a pragmatic, parallel-group, observer-blinded, randomized controlled trial, involving medical and surgical patients admitted to the ICUs of three hospitals: two tertiary referral academic centers (University Hospitals of the KU Leuven, Leuven, Belgium and Academic Medical Center at the University of Amsterdam, Amsterdam, The Netherlands) and one non-academic, teaching hospital (Jessa Hospital, Hasselt, Belgium). All ICUs involved have a closed organization, staffed by full-time intensivists, and represent, respectively, 98, 50, and 36 ICU beds.
The study protocol and informed consent documents were approved by the Belgian Federal Agency for Medicines and Health Products (80 M0563) and the institutional review boards of each participating center. The trial was registered on ClinicalTrials.gov (NCT02056353) on 4 February 2014. No design changes occurred during the trial. Whenever possible, informed consent was asked for from the decision-competent patient before study inclusion. In the case of emergency ICU admissions, deferred proxy consent from the legal representative was obtained. The data and safety monitoring board (DSMB) reviewed the data twice according to the charter and advised continuation according to the initial protocol.
Participants
Patients were recruited from 24 February 2014 to 17 December 2014. All patients admitted to the ICU with an expected stay of at least 2 days and already receiving or potentially needing insulin for blood glucose control were screened for eligibility (Fig. 1). Exclusion criteria were: not critically ill (monitoring only, not requiring vital organ support), moribund on admission, younger than 18 years of age, enrolled in another intervention trial, no arterial line, pregnant or breast feeding, diabetic ketoacidosis or hyperosmolar state on admission, previously included in the LOGIC-2 trial, or declined participation.
Fig. 1.
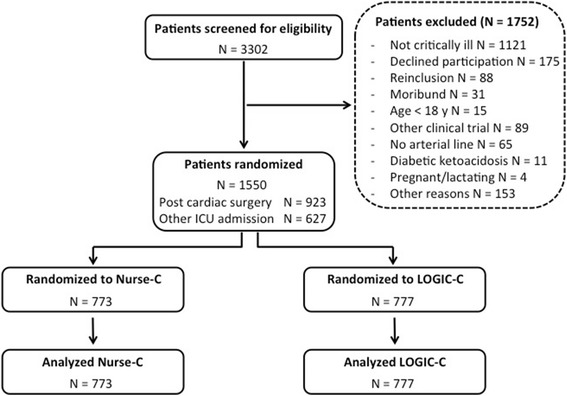
Recruitment of patients into the study. All patients admitted to the ICU in the three participating centers from 24 February 2014 until 17 December 2014, in whom blood glucose control needed to be initiated, were screened for eligibility. This resulted in 1550 patients who were randomized and analyzed (923 patients after cardiac surgery and 627 patients for other reasons as predefined). All patients were included in the primary analysis. LOGIC-C patients randomized to algorithm-guided blood glucose control, Nurse-C patients randomized to blood glucose control by trained nurses
Randomization
Consecutive patients were randomly allocated into either the nurse-directed (Nurse-C) or the LOGIC-Insulin-guided (LOGIC-C) group by a central computerized system on a 1:1 ratio with permuted blocks of 10 per stratum. Block size was unknown to all collaborators. Randomization was stratified according to type of admission (post-cardiac surgery or other) and study center. Randomization of cardiac surgery patients was stopped after reaching 60% of the total study population across all centers. Outcome assessors, but not clinical staff, were blinded to treatment allocation.
Intervention
Patients received blood glucose control according to the assigned group: Nurse-C or LOGIC-C. An intravenous infusion of insulin was started on admission in both groups to aim for glycemia in the target range, which in the Leuven and Hasselt ICUs was glycemia 80–110 mg/dL, and in the Amsterdam ICU was glycemia 90–145 mg/dL. Blood glucose targets were identical for both diabetic and non-diabetic patients. In all centers and in both randomization groups insulin treatment was initiated when glycemia exceeded the upper limit of the target range.
BGC was discontinued in both groups when the patients started oral intake of carbohydrates, when the arterial and/or central line was removed, when the patient was discharged to the general ward or to an external ICU, when palliative care was initiated, or when recurrent severe hypoglycemic episodes (glycemia <40 mg/dL) or refractory hyperglycemia (>180 mg/dL and insulin at the aforementioned maximum rate) were observed. Blood glucose concentrations were measured in undiluted arterial blood by an on-site blood gas analyzer, which differed between study sites. Insulin at a concentration of 50 IU in 50 mL of saline was infused through a central venous catheter, preferably via a dedicated lumen, using a syringe pump.
BGC in the Nurse-C group was based on the existing local documented guidelines. All bedside nurses had undergone training in blood glucose management during their schooling as an ICU nurse in the different units. No specific training in BGC was given to nurses performing BGC in the Nurse-C group for the purpose of this study. Hence there was a range of experience in dealing with insulin in the context of BGC. The bedside nurse decided on the timing of blood glucose sampling and the adjustment of the insulin infusion rate according to the best clinical practice.
The LOGIC-insulin algorithm guided BGC in the LOGIC-C group. The LOGIC-Insulin software is an open loop system that advises the nurse on the dose of insulin administration, or on dextrose in the case of hypoglycemia, and on the timing of the subsequent blood glucose measurement. It also entails visual warnings about sampling time, hypoglycemia and potential user entry errors, such as nutrition. All LOGIC-Insulin advices have to be confirmed by the bedside nurse and, if appropriate, can be overruled. The heart of the LOGIC-Insulin algorithm itself is a robust, biphasic, and adaptive patient model. The first phase consists of two main parameters: patient profile on the one hand and admission variables, such as diabetes mellitus and the severity of illness, on the other hand. The second phase comprises five variables: patient profile, blood glucose, insulin dose sequence, the administration of steroids, and nutrition.
Further, the algorithm includes both feedback and predictive mechanisms allowing estimation of the effect of future disturbance factors [25, 26]. The combination of both feedback and predictive mechanisms distinguishes the LOGIC-Insulin algorithm from other computerized protocols such as EndoTool since these are mainly based on feedback mechanisms [23]. The LOGIC-Insulin algorithm can be compared to STAR, a computer algorithm that is also based on feedback and predictive mechanisms and which has already been evaluated in two different ICUs [24].
The LOGIC-Insulin algorithm was designed and configured in the pre-study phase to deal with varying blood glucose target ranges. Since there was a 1:2 to 1:3 nurse-patient ratio in the participating hospitals, nurses may have had to treat patients in the two different groups: Nurse-C and LOGIC-C.
Outcomes and measures
The primary outcome measure of the LOGIC-2 trial was quality of blood glucose control, assessed by the glycemic penalty index (GPI) per patient, during the intervention period, censored at 14 days. This index gives a penalty to all glucose values falling in the hypoglycemic and hyperglycemic zones with a higher penalty value for larger deviations from normoglycemia [27]. The average of all penalties is summarized as the GPI, ranging from 0 to 100.
The other outcome measures of BGC were in line with the recent consensus recommendations on reporting of glycemia in critically ill patients [28]. The most important safety outcome measure was the incidence of severe hypoglycemia (<40 mg/dL). The incidence per patient and the incidence as a proportion of all blood glucose measurements were reported. The incidence of extended hyperglycemia, defined as three consecutive blood glucose measures >180 mg/dL, was added by the DSMB as a safety outcome measure.
Other secondary endpoints were the incidence of mild hypoglycemia (<70 mg/dL), mean arterial blood glucose concentration, hyperglycemic index (area under the curve in the hyperglycemic zone), time-in-target range, time-to-reach-target range, maximal blood glucose difference (marker of blood glucose variability) and the interval between blood glucose measurements (marker of workload), all reported as per-patient metrics with the exception of the incidence of mild hypoglycemia, which is presented both as the incidence per patient and the incidence per proportion of measurements. In the intervention group protocol compliance (patients in whom the LOGIC-insulin software was not followed for a period of at least 8 h) and overrules (recommendations that were not followed by the bedside nurse) of the software were assessed. A distinction was made between minor (absolute insulin dose difference of > 0.1 IU/h and <1 IU/h) and major (≥1 IU/h) overrules.
Clinical safety endpoints were the incidence of new infections in the ICU (as scored by a blinded infectious disease specialist), ventilator days per patient (censored at 14 days), length of stay in the ICU and in the hospital, mortality in ICU and in hospital, and the landmark 90-day mortality. Quality of life was assessed using the EuroQol 5D-3 L questionnaire at ICU admission, ICU discharge and 90 days post-randomization. Sepsis was diagnosed, using the American College of Chest Physicians-Society of Critical Care Medicine criteria [29].
Statistical analyses
The study was conceived as a superiority trial for improving the quality of blood glucose control, measured by GPI and the time-in-target range, and it was also powered to detect differences in the incidence of mild hypoglycemia (<70 mg/dL) as a safety outcome variable. The sample size calculations were preregistered at the Belgian Federal Agency for Medicines and Health Products. Better performance in BGC in the Nurse-C group was anticipated, as nurses would feel they were to be watched (Hawthorne effect). On the basis of a 5% confidence level (α error) and a 90% statistical power (β error 10%) the study required 458 patients in each arm to detect a decrease in GPI from mean 21 to 18 (sigma 14) in a two-sided test. An increase in the time-in-target range from 45% to 50% with a sigma 29% would require 707 patients per arm. For a decrease in mild hypoglycemia from 27% to 20% (ARR 7%) the study required 769 patients in each arm. To take into account withdrawals, the study was set up for 1550 patients (775 patients in each group).
A subgroup analysis per study center and blood glucose target was preplanned. The following subgroup analyses for specific patient populations were also planned: cardiac surgery, medical, sepsis on admission, infection on admission, and known diabetes mellitus.
Variables were summarized as frequencies and percentages, mean and standard deviation (SD) or median and interquartile range (IQR), as appropriate. Confidence intervals were computed based on the bootstrap percentile method for the primary and secondary endpoints [30].
All analyses were done on an intention-to-treat basis. Data were compared using the chi-square (χ2) (Fisher exact) test, Student t test, or nonparametric (Wilcoxon rank sum) test as appropriate. For all endpoints, differences were considered statistically significant whenever the two-sided P value was <0.05, without correction for multiple testing. For the statistical analyses, JMP Pro 11 (SAS Institute, Cary, NC, USA) and Matlab (MathWorks, Natick, MA, USA) were used.
Results
Study participants
A total of 3302 patients were screened for eligibility, of whom 1550 (47%) gave consent and were randomized to either Nurse-C or LOGIC-C (Fig. 1). None of the patients was lost to follow up. The baseline characteristics of the treatment groups were similar (Table 1). The percentage of admissions after cardiac surgery was 59% and 60% in the Nurse-C and the LOGIC-C group, respectively. On admission, 21.6% of patients had known diabetes mellitus and 28% an infection.
Table 1.
Baseline characteristics
| Nurse-C | LOGIC-C | |
|---|---|---|
| Total | 773 | 777 |
| Age, mean (SD), years | 66 (15) | 66 (14) |
| Male, n (%) | 478 (62) | 495 (64) |
| BMI, mean (SD), kg/m2 | 26.4 (5.2) | 26.3 (4.9) |
| Diabetes, n (%) | 167 (21.6) | 168 (21.6) |
| Chronic dialysis, n (%) | 17 (2) | 11 (1) |
| APACHE-II score, mean (SD) | 20 (9) | 21 (9) |
| Admission type | ||
| Cardiac surgery, n (%) | 458 (59) | 465 (60) |
| Other surgery, n (%) | 164 (21) | 130 (17) |
| Medical, n (%) | 131 (17) | 164 (21) |
| Transplantation, n (%) | 20 (3) | 18 (2) |
| Adm mechanical ventilation, n (%) | 661 (86) | 657 (85) |
| Adm insulin infusion, n (%) | 171 (21) | 164 (22) |
| Adm blood glucose level (mg/dL), median (IQR) | 127 (108–153) | 128 (106–153) |
| Adm hypoglycemia (<40 mg/dL), n (%) | 1 (0.1) | 1 (0.1) |
| Adm blood lactate level (mmol/L), median (IQR) | 1.3 (1.0–1.9) | 1.3 (1.0–2.0) |
| Adm infection, n (%) | 219 (28) | 217 (28) |
| Adm sepsis, n (%) | 102 (13) | 129 (17) |
| Adm EQ-5D value index (%), median (IQR) | 0.72 (0.35–1) | 0.71 (0.33–0.90) |
| Adm EQ-5D VAS score (%), median (IQR) | 0.65 (0.50–0.80) | 0.65 (0.42–0.80) |
Data are mean (SD), median (IQR) or n (%) LOGIC-C patients randomized to algorithm-guided blood glucose control, Nurse-C patients randomized to blood glucose control by trained nurses, APACHE-II Acute Physiology and Chronic Health Evaluation-II, BMI body mass index, Adm admission, EQ-5D Euroqol-5D, VAS visual analog scale
Blood glucose control
The GPI, the primary outcome measure, was 6.3 points lower in the LOGIC-C group than in the Nurse-C group (P < 0.001) (Table 2). Time-in-target range was increased from 47.1% in the Nurse-C group to 67.0% in LOGIC-C group (P < 0.001). Mean blood glucose levels and the hyperglycemic index were also lower in the LOGIC-C group (all P < 0.001). Moreover, blood glucose variability was decreased in the LOGIC-C group (P < 0.001). The proportion of patients experiencing at least one episode of hypoglycemia did not differ between treatment groups (all P > 0.07). However, the proportion of blood glucose readings <70 mg/dL and <60 mg/dL was smaller in the LOGIC-C group (both P = 0.02). None of the subjects in either randomized group experienced recurrent severe hypoglycemic episodes or refractory hyperglycemia that warranted withdrawal from the study. Workload was higher in the LOGIC-C group, as reflected in a 23% shorter sampling interval (P < 0.001).
Table 2.
Blood glucose control in the two randomized groups
| Nurse-C | LOGIC-C | P value | |||
|---|---|---|---|---|---|
| 95% CI | 95% CI | ||||
| Patients | 773 | 777 | |||
| Study period, median (IQR), days | 2 (2–4) | 2 (2–4)) | 0.7 | ||
| Efficacy | |||||
| Glycemic penalty index (GPI), median (IQR) | 17.1 (10.6–26.2) | 16.3–18.1 | 10.8 (6.2–16.1) | 10.0–11.5 | <0.001 |
| Blood glucose, mean (SD), mg/dL | 119 (21) | 118–121 | 111 (15) | 110–112 | <0.001 |
| Minimum blood glucose, mg/dL | 21 | 26 | |||
| Maximum blood glucose, mg/dL | 428 | 511 | |||
| Hyperglycemic index, median (IQR), mg/dL | 8.3 (3.4–16.3) | 7.5–8.8 | 3.5 (1.4–7.0) | 3.1–4.0 | <0.001 |
| Time-in-target range, median (IQR), percentage | 47.1 (28.1–65.0) | 45.7–49.3 | 67.0 (52.1–80.1) | 65.4–68.6 | <0.001 |
| Time to reach target range, median (IQR), h | 3.6 (0–9.3) | 3.2–4.3 | 2.2 (0–5.1) | 1.8–2.5 | <0.001 |
| Mean of maximum delta glycemia per day, median (IQR), mg/dL | 36 (27–52) | 35–38 | 34 (24–46) | 32–36 | <0.001 |
| Safety | |||||
| Hypoglycemia, proportion of patients | |||||
| <70 mg/dL, n (%) | 173 (22.4) | 151–196 | 149 (19.2) | 128 –171 | 0.1 |
| <60 mg/dL, n (%) | 78 (10.1) | 62–95 | 58 (7.5) | 44–73 | 0.07 |
| <40 mg/dL, n (%) | 9 (1.2) | 4–15 | 7 (0.9) | 2–13 | 0.6 |
| Hypoglycemia, proportion of samples | |||||
| <70 mg/dL, n (%) | 346 (1.8) | 311–382 | 342 (1.5) | 306–379 | 0.02 |
| <60 mg/dL, n (%) | 123 (0.7) | 102–145 | 105 (0.5) | 85–125 | 0.02 |
| <40 mg/dL, n (%) | 9 (0.05) | 4–15 | 9 (0.04) | 4–15 | 0.9 |
| Workload | |||||
| Sampling interval, mean (SD), h | 3.0 (0.8) | 2.9–3.0 | 2.3 (0.5) | 2.3–2.3 | <0.001 |
Data are mean (SD), median (IQR) or n (%). LOGIC-C patients randomized to algorithm-guided blood glucose control, Nurse-C patients randomized to blood glucose control by trained nurses
Predefined subgroups
The effect of the LOGIC-Insulin algorithm on BGC was more pronounced in Hasselt and Amsterdam (Fig. 2). While the GPI was 3.6 points lower in the Leuven LOGIC-C group, the difference was 10.1 in Hasselt and 15.1 in Amsterdam (Additional file 1: Tables S1-S3). Furthermore, LOGIC-Insulin-guided BGC resulted in mean blood glucose levels in the target range for Hasselt (110 mg/dL) and Amsterdam (134 mg/dL), whereas those in the Nurse-C group were above the target range, at 123 mg/dL and 150 mg/dL, respectively. This was in contrast to Leuven, where the mean blood glucose level was in the target range in both the Logic-C (106 mg/dL) and the Nurse-C (109 mg/dL) groups. While the incidence of mild hypoglycemia decreased in the Leuven LOGIC-C group, it increased in the Hasselt LOGIC-C group, compared with their respective Nurse-C groups. In all three centers, the sampling interval was shorter in the LOGIC-C, compared with the Nurse-C group.
Fig. 2.
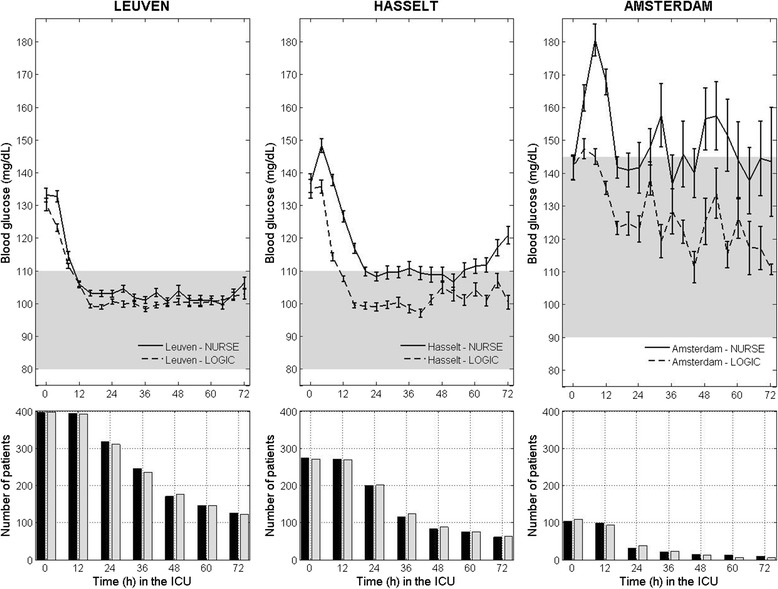
Blood glucose control and numbers of patients in the two randomized groups during the first 3 days in the ICU, per study center. Upper panels overall mean blood glucose levels (mg/dL) for both the algorithm-guided (dashed line) and the nurse-directed (solid line) blood glucose control group per center during the first 72 h in the ICU, which is the median ICU stay. The average blood glucose is computed over all glucose samples (per center) belonging to the previous 4-h time slot. The glycemic target range was 80–110 mg/dL for Leuven and Hasselt, unlike Amsterdam where the glycemic target range was 90–145 mg/dL. Lower panels the number of patients for the Nurse-C group (Nurse) (black bars) and LOGIC-C group (LOGIC) (gray bars)
The quality of BGC was improved by the algorithm in the predefined subgroups of cardiac surgery (Additional file 1: Table S4), medical admission (Additional file 1: Table S6), sepsis on admission (Additional file 1: Table S8), infection on admission (Additional file 1: Table S10) and known diabetes mellitus (Additional file 1: Table S12).
Factors interfering with blood glucose control and compliance with the LOGIC-Insulin software during the study period
Patients in the LOGIC-C group received a larger daily insulin dose (median 32 IU/day IQR 18–48 versus median 27 IU/day IQR 14–43 in the Nurse-C group) (P < 0.001). The median daily amount of carbohydrates was 42 g (IQR 31–68) in the LOGIC-C and 42 g (IQR 30–70) in the Nurse-C group (P = 0.88). The number of LOGIC-C patients who received steroids (24.1%) was comparable to the Nurse-C group (21.7%) (P = 0.28). Also the proportion of patients on mixed-bag parenteral nutrition did not differ between the LOGIC-C (7.3%) and the Nurse-C (10.0%) groups (P = 0.07). The number of days patients received inotropics/vasopressors (2 days, IQR 1–3 versus 2 days, IQR 1–3) and antibiotics (1 day, IQR 1–3 versus 2 days, IQR 1–3) did not differ between treatment groups (both P > 0.39).
In 80/777 patients (10.3%) in the LOGIC-C group, the software had not been used for more than 8 h. In total 240 minor and 147 major overrules occurred in the LOGIC-C group, representing 1.15% and 0.70% of blood glucose measurements, respectively. Of the major overrules, 14 (9.5%) were justified, and of these only 2 overrules were made to avoid hypoglycemia, representing 2/777 LOGIC-C patients (0.3%). In Amsterdam the proportion of overrules (minor 19 (1.71%), major 20 (1.80%) for insulin dosing advice given in 1114 instances) was higher than in Leuven (minor 155 (1.30%), major 89 (0.75%) for insulin dosing advice given in 11926 instances) and Hasselt (minor 66 (0.84%), major 38 (0.48%) for insulin dosing advice given in 7892 instances) (P < 0.001).
Clinical safety outcomes
The clinical outcomes did not differ between the treatment groups (Table 3 and Additional file 1: Table S16). However, in patients with sepsis on admission the incidence of new infections was lower in the LOGIC-C (20.16%) than in the Nurse-C group (33.33%) (P = 0.034). In patients with an infection on admission, the incidence of new infections was 23.04% in the LOGIC-C, compared with 31.96% in the Nurse-C group (P = 0.042). For all other predefined subgroups (cardiac surgery, medical admission, and diabetes mellitus) the incidence of new infections was comparable between treatment groups.
Table 3.
Clinical safety outcome measures
| Nurse-C | LOGIC-C | P value | |
|---|---|---|---|
| Patients | 773 | 777 | |
| Length of ICU stay, median (IQR), days | 3 (2–6) | 3 (2–6) | 0.39 |
| Length of hospital stay, median (IQR), days | 12 (8–23) | 12 (8–23) | 0.18 |
| Mortality in the ICU, n (%) | 41 (5.30) | 47 (6.05) | 0.61 |
| Mortality in the hospital, n (%) | 84 (10.81) | 72 (9.31) | 0.35 |
| Mortality at 90 days, n (%) | 89 (11.71) | 91 (11.51) | 0.93 |
| Incidence of new infections in the ICU, n (%) | 117 (15.14) | 104 (13.38) | 0.35 |
| Ventilator days, median (IQR), days | 1 (1–2) | 1 (1–3) | 0.85 |
| EQ-5D index value at ICU discharge, median (IQR) | 0.28 (0.13–0.58) | 0.29 (0.13–0.58) | 0.59 |
| EQ-5D index value at 90 days, median (IQR) | 0.73 (0.56–1) | 0.73 (0.56–1) | 0.58 |
| EQ-5D VAS score at ICU discharge, median (IQR) | 0.60 (0.50–0.70) | 0.60 (0.50–0.70) | 0.42 |
| EQ-5D VAS score at 90 days, median (IQR) | 0.70 (0.60–0.80) | 0.70 (0.60–0.80) | 0.97 |
Data are mean (SD), median (IQR) or n (%). LOGIC-C patients randomized to algorithm-guided blood glucose control, Nurse-C patients randomized to blood glucose control by trained nurses, EQ-5D Euroqol-5D, VAS visual analog scale
Discussion
Using the LOGIC-Insulin algorithm improved the quality of BGC reflected by a reduction in the GPI, an increase in time-in-target range and a reduction in blood glucose variability, without increasing the incidence of hypoglycemia.
The beneficial effects of software-guided BGC were independent of the chosen target blood glucose range and of the center’s expertise in BGC. Morbidity and mortality did not differ between patients in whom BGC was done either by expert nurses or aided by the LOGIC-Insulin algorithm in the context of similar blood glucose target ranges.
These data confirm the findings from our single center trial, in which LOGIC-Insulin improved tight BGC and lowered the incidence of mild hypoglycemia [25]. However, the treatment effect in the pragmatic multicenter LOGIC-2 trial was twofold that in the LOGIC-1 trial and that for which it was statistically powered. This was explained by more pronounced benefits of algorithm-guided BGC in centers with looser BGC. The performance of the Leuven nurses in BGC, incorporated in the LOGIC-Insulin algorithm, may also have blunted the effect in Leuven. Similar blood glucose profiles in the software groups in Leuven and Hasselt, using the same target range, demonstrate that the LOGIC-Insulin software can be generalized outside the context of centers with extensive BGC experience. The fact that more than 98% of all insulin dosing advice provided by the LOGIC-Insulin algorithm were followed by the nurses in all centers in the algorithm-guided BGC group indicates high protocol compliance and indicates that the results are protocol-induced and not a representation of the nurses’ BGC performance in the intervention group. This further underpins the generalizability of the study findings and the potential for implementation of the LOGIC-Insulin software, independent of the chosen blood glucose target range. This is important as the interaction between the BGC algorithm and patient glucose dynamics may be influenced by the performance of the bedsides nurses, who are the ultimate “controllers” in open-loop BGC software.
The larger treatment effect in the broader target range of 90–145 mg/dL (delta GPI 15.1) than in the narrow target range of 80–110 mg/dL (delta GPI 5.7) was therefore not anticipated. One might have expected that BGC is easier for nurses when the target is broader. This indicates that nurses, in the context of a broader target range, tend to be more lenient towards the upper target limit. The higher incidence of extended hyperglycemia above 180 mg/dL reflects this, in spite of the consensus in all guidelines on BGC in the ICU that excessive hyperglycemia should be avoided. Nevertheless, the higher incidence of overrules in Amsterdam, possible practical differences in the insulin administration, and greater statistical uncertainty due to the smaller patient numbers may have contributed as well. Most likely, BGC will be even looser outside study settings. In contrast, use of the narrower target range results in greater incidence of mild hypoglycemia. Algorithm-guided BGC did not increase the incidence of potentially harmful, severe hypoglycemia, which should always be strictly avoided. A recent randomized controlled trial used computerized insulin-dosing algorithms in the intensive BGC group, but did not show a clinical difference with more conservative, nurse-directed BGC [31].
Algorithm-guided BGC increased the workload, similar to other algorithms [32]. Ten instead of eight blood glucose measurements per day were needed to improve BGC in one patient by software use. The workload of blood glucose measurements may be offset by lowering of the cognitive burden for the nurses in deciding on the right insulin dose [33]. Hence, this slight increase in workload may be inevitable in obtaining safe and effective blood glucose control, especially in the initial phase, aiming for a short time to reach the chosen target range combined with a high time-in-target range, low glucose variability, and avoidance of hypoglycemia, and this in a setting with rapid changes in patients insulin sensitivity and in the presence of external confounding factors such as use of steroids and parenteral nutrition. There is now a consensus that a minimal measurement frequency is needed to provide safe glycemic control without adverse effects on the outcome [28]. Whether the increased workload resulted in more attention paid to the patient (collateral benefit) or less attention to the patient (added risk) cannot be delineated from this study.
The improvement in BGC provided by the software was comparable in all patient populations, such as cardiac surgery, pre-existing diabetes, sepsis, and medical admissions. However, the clinical effects of improved BGC should be the ultimate determinants to evaluate medical interventions. Although the LOGIC-2 trial was not set up to test differences in clinical outcomes, it was monitored. As expected, no clinical differences were seen in the overall patient population. Patients with diabetes mellitus did not benefit more from algorithm-guided BGC, as was seen in a recent trial of BGC in patients after coronary artery bypass graft surgery [34]. However, the level of pre-admission control of the diabetes mellitus may be the most important factor in determining whether patients benefit from tight BGC.
In patients with infectious problems on admission, improved BGC resulted in lowering of the incidence of new infections. This may be explained by the fact that patients with infectious problems on admission are more severely ill, have greater risk of more severe hyperglycemia, which is more difficult to control, and have greater risk of new infections.
The LOGIC-2 trial has its limitations though. Blood glucose dynamics in the ICU are determined by patient characteristics, by the BGC protocol, and by the experience of the bedside nurses in executing the BGC. Therefore, the differences in the quality of BGC in the Nurse-C group between the centers are most likely multifactorial. The variability in the “baseline” quality of BGC may have affected the performance using the LOGIC-Insulin software. It can also not be excluded that nursing practice in performing BGC changed over time during the study, under the influence of the algorithm. However, participating in a study on BGC had most likely improved the performance of BGC by the nurses over time due to a training effect. The LOGIC-Insulin software was now only tested when using glucose readings from arterial blood measured in accurate blood gas analyzers. To gain further applicability the software should be able to cope with blood glucose measurements from point-of-care, handheld blood glucose meters. Other computerized protocols however, have already used these point-of-care glucometers showing a safe and efficient level of blood glucose control [23, 24]. Efficiency or cost-effectiveness of the LOGIC-Insulin software is still unproven, despite that the present pragmatic multicenter RCT showed that the software works in real-life circumstances.
Conclusions
In a randomized controlled trial of a mixed critically ill patient population, the use of the LOGIC-Insulin blood glucose control algorithm, compared with blood glucose control by expert nurses, improved the quality of blood glucose control without increasing hypoglycemia. This is demonstrated by an important improvement in all domains of glycemic control: a decrease in GPI, an increase in the time-in-target range, and a decrease in glucose variability. Moreover, the LOGIC-Insulin algorithm was shown to be efficient and safe when used in three different ICUs with local variations in clinical practice, with different blood glucose target ranges, and with different levels of experience in blood glucose control. The slight increase in workload generated by the LOGIC-insulin algorithm should be considered an inevitable trade-off when providing safe and efficient blood glucose control.
Additional files
Tables showing predefined subgroup analyses. (DOCX 50 kb)
Study protocol: Competent Authority submission. (PDF 8786 kb)
Acknowledgements
We thank Drs Roger Bouillon, Peter Lauwers, Jan J Vranckx, and Jos De Brabanter for serving on the DSMB; the team of research nurses, Sylvia Van Hulle, Alexandra Hendrickx, Heidi Utens Tineke Winters, Peter Beckers, and Nora Croonen for data collection; Jan Vermeyen for data quality auditing; Drs Yves Debaveye and Tom Fivez for the scoring of infections; and the attending nurses and physicians for ensuring protocol compliance and patient care.
Funding
This study was supported by the Flemish Agency for Innovation by Science and Technology (IWT-TBM-100793), the KU Leuven (IOF-HB/13/27) and iMINDS Medical Information Technologies (SBO 2015). DM holds a Senior Clinical Investigator fellowship of the Research Foundation Flanders (FWO). GVdB, via the University of Leuven, receives structural research financing via the Methusalem program, funded by the Flemish Government (METH08/07 and METH14/06), and holds an ERC Advanced grant (AdvG-2012-321670) from the Ideas Program of the EU FP7. The sponsor/funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, and approval of the manuscript.
Availability of data and materials
Tom Van Herpe and Dieter Mesotten had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Jasperina Dubois, Tom Van Herpe and Dieter Mesotten conducted and are responsible for the data analysis. The datasets used and/or analyzed during the current study are available from the corresponding author and the data manager on reasonable request.
Abbreviations
- BGC
Blood glucose control
- DSMB
Data and safety monitoring board
- GPI
Glycemic penalty index
- ICU
Intensive care unit
- IQR
Interquartile range
- LOGIC-C group
Patients randomized to algorithm-guided blood glucose control
- Nurse-C group
Patients randomized to blood glucose control by trained nurses
- RCT
Randomized controlled trial
Authors’ contributions
JD, TVH, MJS, GVdB, and DM designed the study protocol. TvH and DM wrote the statistical analysis plan. JD, TVH, RvH, RW, DC, AVA, JW, and AW supervised patient recruitment in each participating center. PW and TVH designed the database, supervised and monitored data entry by the study nurses, checked the database for accuracy, and exported the data for statistical analysis. TVH, GV, and BDM were responsible for operating the software and its data extraction. TVH and DM performed the statistical analyses and JD, TVH, and DM drafted the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
The study protocol and informed consent documents were approved by the Belgian Federal Agency for Medicines and Health Products (80 M0563) (Additional file 2) and the institutional review boards of each participating center. The trial was registered on ClinicalTrials.gov (NCT02056353) on 4 February 2014.
Consent for publication
Not applicable.
Competing interests
Tom Van Herpe, Bart De Moor and Greet Van den Berghe are inventors on EP1487518. Bart De Moor and Greet Van den Berghe are inventors on US2005171503. Roosmarijn T.M. van Hooijdonk reports consulting work for Medtronic Inc., GlySure Ltd and research support from Medtronic Inc. and Optiscan Biomedical - all fees and financial support were paid to the institution. Marcus J. Schultz reports receiving consultant fees from Medtronic Inc., GlySure Ltd, Edwards Life Sciences and Roche Diagnostics, and financial support from Medtronic Inc. and OptiScan Biomedical - all fees and financial support were paid to the institution. All other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Footnotes
Electronic supplementary material
The online version of this article (doi:10.1186/s13054-017-1799-6) contains supplementary material, which is available to authorized users.
A comment to this article is available at https://doi.org/10.1186/s13054-017-1824-9.
Contributor Information
Jasperina Dubois, Email: jasperina.dubois@jessazh.be.
Tom Van Herpe, Email: tomvanherpe@gmail.com.
Roosmarijn T. van Hooijdonk, Email: r.t.vanhooijdonk@amc.uva.nl
Ruben Wouters, Email: rubenwouters@hotmail.com.
Domien Coart, Email: domien.coart@icloud.com.
Pieter Wouters, Email: pieter.wouters@uzleuven.be.
Aimé Van Assche, Email: aime.vanassche@jessazh.be.
Guy Veraghtert, Email: guy.veraghtert@gmail.com.
Bart De Moor, Email: bart.demoor@esat.kuleuven.be.
Joost Wauters, Email: joost.wauters@med.kuleuven.be.
Alexander Wilmer, Email: alexander.wilmer@uzleuven.be.
Marcus J. Schultz, Email: marcus.j.schultz@gmail.com
Greet Van den Berghe, Email: greet.vandenberghe@med.kuleuven.be.
Dieter Mesotten, Email: dieter.mesotten@gmail.com.
References
- 1.Siegelaar SE, Hermanides J, Oudemans-van Straaten HM, van der Voort PH, Bosman RJ, Zandstra DF, et al. Mean glucose during ICU admission is related to mortality by a U-shaped curve in surgical and medical patients: a retrospective cohort study. Crit Care. 2010;14(6):R224. doi: 10.1186/cc9369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345(19):1359–67. doi: 10.1056/NEJMoa011300. [DOI] [PubMed] [Google Scholar]
- 3.Van den Berghe G, Wilmer A, Hermans G, Meersseman W, Wouters PJ, Milants I, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006;354(5):449–61. doi: 10.1056/NEJMoa052521. [DOI] [PubMed] [Google Scholar]
- 4.Vlasselaers D, Milants I, Desmet L, Wouters PJ, Vanhorebeek I, van den Heuvel I, et al. Intensive insulin therapy for patients in paediatric intensive care: a prospective, randomised controlled study. Lancet. 2009;373(9663):547–56. doi: 10.1016/S0140-6736(09)60044-1. [DOI] [PubMed] [Google Scholar]
- 5.Krinsley JS. Effect of an intensive glucose management protocol on the mortality of critically ill adult patients. Mayo Clin Proc. 2004;79(8):992–1000. doi: 10.4065/79.8.992. [DOI] [PubMed] [Google Scholar]
- 6.Furnary AP, Cheek DB, Holmes SC, Howell WL, Kelly SP. Achieving tight glycemic control in the operating room: lessons learned from 12 years in the trenches of a paradigm shift in anesthetic care. Semin Thorac Cardiovasc Surg. 2006;18(4):339–45. doi: 10.1053/j.semtcvs.2007.01.004. [DOI] [PubMed] [Google Scholar]
- 7.Finfer S, Chittock DR, Su SY, Blair D, Foster D, Dhingra V, et al. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283–97. doi: 10.1056/NEJMoa0810625. [DOI] [PubMed] [Google Scholar]
- 8.Preiser JC, Devos P, Ruiz-Santana S, Melot C, Annane D, Groeneveld J, et al. A prospective randomised multi-centre controlled trial on tight glucose control by intensive insulin therapy in adult intensive care units: the Glucontrol study. Intensive Care Med. 2009;35(10):1738–48. doi: 10.1007/s00134-009-1585-2. [DOI] [PubMed] [Google Scholar]
- 9.Brunkhorst FM, Engel C, Bloos F, Meier-Hellmann A, Ragaller M, Weiler N, et al. Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med. 2008;358(2):125–39. doi: 10.1056/NEJMoa070716. [DOI] [PubMed] [Google Scholar]
- 10.Jacobi J, Bircher N, Krinsley J, Agus M, Braithwaite SS, Deutschman C, et al. Guidelines for the use of an insulin infusion for the management of hyperglycemia in critically ill patients. Crit Care Med. 2012;40(12):3251–76. doi: 10.1097/CCM.0b013e3182653269. [DOI] [PubMed] [Google Scholar]
- 11.Mesotten D, Preiser JC, Kosiborod M. Glucose management in critically ill adults and children. Lancet Diabetes Endocrinol. 2015;3(9):723–33. doi: 10.1016/S2213-8587(15)00223-5. [DOI] [PubMed] [Google Scholar]
- 12.American Diabetes A (13) Diabetes care in the hospital, nursing home, and skilled nursing facility. Diabetes Care. 2015;38(Suppl):S80–5. doi: 10.2337/dc15-S016. [DOI] [PubMed] [Google Scholar]
- 13.Finfer S, Liu B, Chittock DR, Norton R, Myburgh JA, McArthur C, et al. Hypoglycemia and risk of death in critically ill patients. N Engl J Med. 2012;367(12):1108–18. doi: 10.1056/NEJMoa1204942. [DOI] [PubMed] [Google Scholar]
- 14.Krinsley JS. Understanding glycemic control in the critically ill: three domains are better than one. Intensive Care Med. 2011;37(3):382–4. doi: 10.1007/s00134-010-2110-3. [DOI] [PubMed] [Google Scholar]
- 15.Mesotten D, Van den Berghe G. Glycemic targets and approaches to management of the patient with critical illness. Curr Diab Rep. 2012;12(1):101–7. doi: 10.1007/s11892-011-0241-8. [DOI] [PubMed] [Google Scholar]
- 16.Kavanagh BP, McCowen KC. Clinical practice. Glycemic control in the ICU. N Engl J Med. 2010;363(26):2540–6. doi: 10.1056/NEJMcp1001115. [DOI] [PubMed] [Google Scholar]
- 17.Saur NM, Kongable GL, Holewinski S, O’Brien K, Nasraway SA., Jr Software-guided insulin dosing: tight glycemic control and decreased glycemic derangements in critically ill patients. May Clin Proc. 2013;88(9):920–9. doi: 10.1016/j.mayocp.2013.07.003. [DOI] [PubMed] [Google Scholar]
- 18.Rattan R, Nasraway SA. The future is now: software-guided intensive insulin therapy in the critically ill. J Diabetes Sci Technol. 2013;7(2):548–54. doi: 10.1177/193229681300700231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Davidson PC, Steed RD, Bode BW. Glucommander: a computer-directed intravenous insulin system shown to be safe, simple, and effective in 120,618 h of operation. Diabetes Care. 2005;28(10):2418–23. doi: 10.2337/diacare.28.10.2418. [DOI] [PubMed] [Google Scholar]
- 20.Saager L, Collins GL, Burnside B, Tymkew H, Zhang L, Jacobsohn E, et al. A randomized study in diabetic patients undergoing cardiac surgery comparing computer-guided glucose management with a standard sliding scale protocol. J Cardiothorac Vasc Anesth. 2008;22(3):377–82. doi: 10.1053/j.jvca.2007.09.013. [DOI] [PubMed] [Google Scholar]
- 21.Cordingley JJ, Vlasselaers D, Dormand NC, Wouters PJ, Squire SD, Chassin LJ, et al. Intensive insulin therapy: enhanced Model Predictive Control algorithm versus standard care. Intensive Care Med. 2009;35(1):123–8. doi: 10.1007/s00134-008-1236-z. [DOI] [PubMed] [Google Scholar]
- 22.Juneja R, Roudebush C, Kumar N, Macy A, Golas A, Wall D, et al. Utilization of a computerized intravenous insulin infusion program to control blood glucose in the intensive care unit. Diabetes Technol Ther. 2007;9(3):232–40. doi: 10.1089/dia.2006.0015. [DOI] [PubMed] [Google Scholar]
- 23.Cochran S, Miller E, Dunn K, et al. EndoTool software for tight glucose control for critically ill patients. Crit Care Med. 2006;34(Suppl 2):A68. doi: 10.1097/00003246-200612002-00241. [DOI] [Google Scholar]
- 24.Stewart KW, Pretty CG, Tomlinson H, Thomas FL, Homlok J, et al. Safety, efficacy and clinical generalization of the STAR protocol: a retrospective analysis. Ann Intensive Care. 2016;6(1):24. doi: 10.1186/s13613-016-0125-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Van Herpe T, Mesotten D, Wouters PJ, Herbots J, Voets E, Buyens J, et al. LOGIC-insulin algorithm-guided versus nurse-directed blood glucose control during critical illness: the LOGIC-1 single-center, randomized, controlled clinical trial. Diabetes Care. 2013;36(2):188–94. doi: 10.2337/dc12-0584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Van den Berghe G, Berckmans D, Aerts J-M, De Moor B, Pluymers B, De Smet F. Automatic infusion system based on an adaptive patient model. Patent US2005/0171503 2005.
- 27.Van Herpe T, De Brabanter J, Beullens M, De Moor B, Van den Berghe G. Glycemic penalty index for adequately assessing and comparing different blood glucose control algorithms. Crit Care. 2008;12(1):R24. doi: 10.1186/cc6800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Finfer S, Wernerman J, Preiser JC, Cass T, Desaive T, Hovorka R, et al. Clinical review: Consensus recommendations on measurement of blood glucose and reporting glycemic control in critically ill adults. Crit Care. 2013;17(3):229. doi: 10.1186/cc12537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101(6):1644–55. doi: 10.1378/chest.101.6.1644. [DOI] [PubMed] [Google Scholar]
- 30.Efron B, Tibshirani R. Bootstrap methods for standard errors, confidence intervals, and other measures of statistical accuracy. Statist Sci. 1986;1(1):54–75. doi: 10.1214/ss/1177013815. [DOI] [Google Scholar]
- 31.Kalfon P, Giraudeau B, Ichai C, Guerrini A, Brechot N, Cinotti R, et al. Tight computerized versus conventional glucose control in the ICU: a randomized controlled trial. Intensive Care Med. 2014;40(2):171–81. doi: 10.1007/s00134-013-3189-0. [DOI] [PubMed] [Google Scholar]
- 32.Amrein K, Kachel N, Fries H, Hovorka R, Pieber TR, Plank J, et al. Glucose control in intensive care: usability, efficacy and safety of Space GlucoseControl in two medical European intensive care units. BMC Endocr Disord. 2014;14:62. doi: 10.1186/1472-6823-14-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ng LS, Curley MA. "One more thing to think about…" Cognitive burden experienced by intensive care unit nurses when implementing a tight glucose control protocol. J Diabetes Sci Technol. 2012;6(1):58–64. doi: 10.1177/193229681200600108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Umpierrez G, Cardona S, Pasquel F, Jacobs S, Peng L, Unigwe M, et al. Randomized controlled trial of intensive versus conservative glucose control in patients undergoing coronary artery bypass graft surgery: GLUCO-CABG trial. Diabetes Care. 2015;38(9):1665–72. doi: 10.2337/dc15-0303. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Tables showing predefined subgroup analyses. (DOCX 50 kb)
Study protocol: Competent Authority submission. (PDF 8786 kb)
Data Availability Statement
Tom Van Herpe and Dieter Mesotten had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Jasperina Dubois, Tom Van Herpe and Dieter Mesotten conducted and are responsible for the data analysis. The datasets used and/or analyzed during the current study are available from the corresponding author and the data manager on reasonable request.