

Abstract
Objective
The prevalence of cardiovascular diseases (CVD) is increasing in developing countries but the awareness regarding prevention and treatment of these diseases is still low. Therefore the present study was conducted with the aim of imparting health education regarding certain changes in lifestyle and dietary habits among general population through the use of short message service (SMS) that may lead to improved knowledge about prevention of cardiovascular diseases.
Methods
This cross-sectional study was conducted over a period of seven months. In the first phase, health education messages were sent through SMS to about 40,000 individuals from urban and rural population in Punjab. Twenty eight messages were sent to each individual and hence more than eleven lakh messages were sent over a period of six months. A questionnaire containing 11 questions based on these health education SMS was generated. Every 40th individual enrolled in the study was contacted on phone, and their responses noted. The data so collected was analyzed for correct responses.
Results
Complete responses could be obtained from 800 participants (males: 561 and females: 239). The participants giving correct responses to different questions ranged from 43% to 94%. Majority of participants could retain knowledge about many aspects of healthy heart habits provided by SMS except for topics concerning foods to be avoided, target for normal BP and precautions to be taken before BP measurement.
Conclusions
Health related information imparted through SMS can act as a very effective tool for disseminating knowledge about prevention of heart diseases in general population.
Keywords: Healthy heart habits, SMS, Cardiovascular, Prevention
1. Background
Cardiovascular diseases (CVDs) are the leading cause of morbidity and mortality among non-communicable diseases worldwide. An increasing trend in proportional mortality attributed to cardiovascular diseases has been reported in India as well, with an increase from 20.6% deaths in 1990 to 29.0% in 2013.1 This increase is mainly due to increase in prevalence of various modifiable risk factors of CVDs like dyslipidemias, smoking, diabetes, hypertension, abdominal obesity, psychosocial stress, unhealthy diet, and physical inactivity. Controlling this epidemic, therefore, requires laying more emphasis on the prevention of these modifiable risk factors.2 Developing nations generally lag behind in prevention of heart diseases because of lack of knowledge about risk factor prevention coupled with poor literacy rates. Creating awareness about these risk factors and spreading knowledge about their prevention should be the main target of health education programs.3, 4
Short message services (SMS) are a widely recognized communication method in societies, as the global outreach of the technology approaches nearly 100%. SMS can send information simultaneously to many people in real time which can be used for spreading health education messages in the community.5, 6 Health education through text messages could encompass primordial, primary and secondary prevention by bringing changes in the lifestyle, preventing the occurrence or slowing the progression of disease.7
Previous studies conducted in developed countries have emphasized that mobile related health (mhealth) interventions may improve cardiovascular-related lifestyle behaviours and disease management through interactive voice response and short message service interventions by addressing various risk factors7, 8, 9, 10, but only a few studies from the developing countries are available in the literature.7 Therefore the present study was planned with a goal of increasing awareness about preventable risk factors of CVDs in the community by using SMS services. The objective of the study was to assess the knowledge about healthy heart habits in urban and rural population of Punjab after providing health education through SMS campaign.
2. Methodology
The study was conducted by Hero DMC Heart Institute (HDHI), which is a part of Dayanand Medical College & Hospital (DMCH) Ludhiana, India. This was a cross-sectional study done over a period of seven months (July 2014 to January 2015). The participants included attendants of patients visiting in different departments of DMCH & three other hospitals in Ludhiana district, parents of students from five schools in urban & rural Ludhiana, members of two welfare clubs and seven voluntary organizations. Ethics clearance was taken from Institutional Ethics Committee for conducting this study and participants were enrolled after taking informed consent and explaining the purpose of the study.
First phase of the study involved sending health education messages regarding healthy heart habits to the above enrolled participants which formed a total population of about 40,000 healthy individuals aged more than 18 years from Urban and Rural population in Punjab (Appendix A). Twenty eight SMS (Appendix B) regarding prevention of heart disease were sent to each participant thus making a total of more than 11 lakh SMS sent over a period of six months. The messages focused on the role of exercise, physical activity, appropriate eating habits, adequate intake of nutrients and other health promotion strategies in the prevention of CVDs, and prevention and early diagnosis of hypertension.
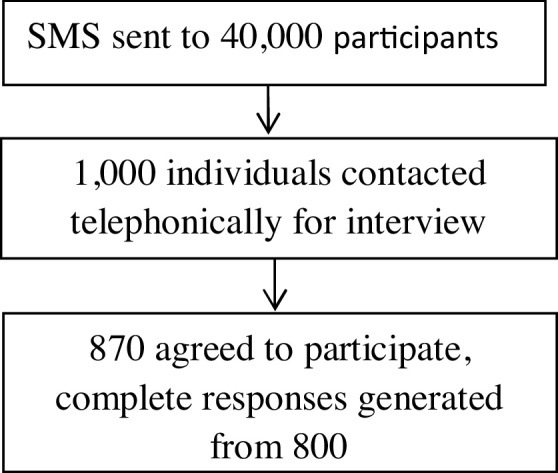
The second phase of the study included assessing the recall of knowledge about healthy heart habits among the participants. A proforma containing 15 questions based on the healthy heart SMS was generated and circulated among five physicians, two cardiologists and one epidemiologist and after consensus, 11 questions were selected (Appendix C). These included six questions on modifiable risk factors of CVDs including diet, physical activity, smoking, dyslipidemia and obesity, and five questions on prevention and early detection of high Blood Pressure (BP). The questionnaire was also prepared in Hindi and Punjabi along with English so as to eliminate any translation bias. After running the SMS campaign for 6 months, every 40th individual enrolled in the study was contacted on phone to interview 1000 individuals but 870 participants agreed to participate and complete responses could be obtained from 800 participants by our data entry operators. For 70 participants, the complete data could not be collected because of discontinuation of the telephone call or the participants disconnected the call due to some other reasons and could not be contacted again. The questionnaire was administered to the participants on phone in their vernacular language. The gender and years of education of the participants was also noted. The answers were then matched to the preformed answer-key for the proforma. The collected data was analyzed using Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.).
3. Results
Out of 1000 participants contacted on phone, 870 participants agreed to respond, thus making a response rate of 87%. Complete answers could be collected from 800 participants including 561 males and 239 females. The mean years of education for the male and female participants were 11.45 ± 5 yrs and 11.59 ± 4.9 yrs respectively. Table 1 shows the genderwise distribution of participants according to correct responses provided by them for the eleven questions. Approximately 94% of participants were aware that reheating of food is a bad practice. More than 90% participants were able to recall that excessive salt intake increases blood pressure and blood pressure medicines have to be adjusted seasonally. Most of them (91.2%) were aware about the role of regular walk in decreasing the risk of heart attacks. Eighty percent of participants were aware that childhood obesity may lead to diabetes, high cholesterol and hypertension. The participants were able to retain less knowledge in topics concerning certain foods to be avoided (51.1%), target for normal BP (66.5%), and precautions to be taken before BP measurement (43.1%). When the percentage of correct responses to different questions was compared with respect to gender, no statistically significant difference in knowledge among male and female participants could be found.
Table 1.
Knowledge of participants with respect to Gender.
| Q. No. | Number of correct responses (N = 800) | Male (N = 561) | Female (N = 239) | Chi Square | P-value | Odd’s Ratio (95% CI) |
|---|---|---|---|---|---|---|
| 1. | 530(66.1%) | 374 (66.7%) | 156 (65.3%) | 0.703 | 0.381 | 0.940 (0.683−1.293) |
| 2. | 729(91.1%) | 516 (92.0%) | 213 (89.1%) | 0.193 | 0.123 | 0.714 (0.430−1.188) |
| 3. | 409(51.1%) | 281 (50.1%) | 128 (53.6%) | 0.369 | 0.206 | 1.149 (0.848−1.556) |
| 4. | 751(93.9%) | 527 (93.9%) | 224 (93.7%) | 0.907 | 0.510 | 0.963 (0.515−1.804) |
| 5. | 593(74.1%) | 418 (74.5%) | 175 (73.2%) | 0.703 | 0.383 | 0.935 (0.663−1.319) |
| 6. | 728(91.0%) | 511 (91.1%) | 217 (90.8%) | 0.895 | 0.495 | 0.965 (0.570−1.633) |
| 7. | 487(60.9%) | 347 (61.9%) | 140 (58.6%) | 0.385 | 0.215 | 0.872 (0.641−1.187) |
| 8. | 532(66.5%) | 373 (66.5%) | 159 (66.5%) | 0.992 | 0.530 | 1.002 (0.727−1.381) |
| 9. | 730(91.2%) | 512 (91.3%) | 218 (91.2%) | 0.981 | 0.539 | 0.993 (0.582−1.697) |
| 10 | 345(43.1%) | 250 (44.6%) | 95 (39.7%) | 0.208 | 0.119 | 0.821 (0.603−1.117) |
| 11 | 642(80.2%) | 450 (80.2%) | 192 (80.3%) | 0.969 | 0.526 | 1.008 (0.689−1.474) |
Knowledge of the participants about healthy heart habits was also evaluated with respect to years of education. As shown in Table 2, years of education was found to be a significant variable for higher knowledge of participants regarding some questions related to prevention of cardiovascular diseases including food for lowering cholesterol, change in medicines for high BP, normal blood pressure, benefits of regular walk and diseases causing childhood obesity.
Table 2.
Knowledge of participants as per years of Education.
| Q. No. | ≤5 yrs (n = 108) |
6–10 yrs (n = 171) | ≥10 yrs (n = 521) | Chi Square | P-value |
|---|---|---|---|---|---|
| 1. | 57 (52.8) | 90 (52.6) | 383 (73.5) | 35.24 | <0.001 |
| 2. | 55 (50.9) | 164 (95.9) | 510 (97.9) | 250.1 | <0.001 |
| 3. | 63 (58.3) | 53 (31.0) | 293 (56.2) | 35.4 | <0.001 |
| 4. | 100 (92.6) | 159 (93.0) | 492 (94.4) | 0.83 | 0.661 |
| 5. | 85 (78.7) | 110 (64.3) | 398 (76.4) | 11.13 | <0.01 |
| 6. | 102 (94.4) | 147 (86.0) | 479 (91.9) | 7.44 | <0.05 |
| 7. | 76 (70.4) | 74 (43.3) | 337 (64.7) | 29.5 | <0.001 |
| 8. | 64 (59.3) | 91 (53.2) | 377 (72.4) | 24.12 | <0.001 |
| 9. | 91 (84.3) | 157 (91.8) | 482 (92.5) | 7.72 | <0.05 |
| 10. | 60 (55.6) | 48 (28.1) | 237 (45.5) | 23.79 | <0.001 |
| 11. | 80 (74.1) | 123 (71.9) | 439 (84.3) | 15.36 | <0.001 |
4. Discussion
Overall, participants retained a significant amount of information about the healthy heart habits provided by SMS service. Thus, SMS services can be effectively used to impart knowledge about prevention of heart disease in general population. In today’s era, mobile phone technology and communication have changed the speed of sending and receiving information among people with more than seven billion mobile phone users worldwide. In recent times it has been recognized that advanced information and telecommunication technologies should be employed to their fullest extent wherever possible, so that interactive sharing and learning can be promoted in an effective and transparent manner.7 It is being explored as a medium to disseminate health related information because of low cost and quick delivery.
Many studies have been done in various developed countries where the potential of text messages and other technological advances have been used for disease prevention and management. A randomized controlled trial conducted by Chow and colleagues (TEXT ME), which included sending text messages to patients with coronary artery disease encouraging them to make healthier lifestyle choices conducted over a period of six months, has shown improvement in their cardiovascular risk factors. The researchers observed a modest improvement in LDL-C level and greater improvement in other cardiovascular disease risk factors.11 In another study, it was shown that text messaging interventions increased adherence to anti retroviral therapy and smoking cessation.12 Text messages may provide useful reminders about prevention and treatment about chronic health problem such as asthma.13 It also can help young people with substance abuse problems in prevention and adherence to treatment.14 Piette et al. in their systematic review of literature about mobile health devices as tools for worldwide cardiovascular risk reduction and disease management, emphasized that interactive voice response and SMS can target the risk factors such as weight, smoking, and physical activity and improve cardiovascular preventive care in developed countries.8
In our study, we had focused on the practices by which health information about healthy heart habits could be imparted to a group of large population in the quickest possible way using SMS services. We also assessed the information participants will be able to recall at a later time. Most of the participants were aware of the harmful effects of reheating of food, excessive salt intake and childhood obesity. They were also knowledgeable about benefits of regular walking and seasonal adjustment of blood pressure medicines. We found that there were certain points which faded away from the memory and may need to be stressed upon by regular reminders. The participants were able to retain less knowledge in topics concerning certain foods to be avoided to prevent CVDs, target for normal BP and precautions to be taken before BP measurement because probably the information was more technical and so the participants could not recall it properly. We also compared years of education with knowledge about healthy heart habits and responses of some questions showed a significant relationship with years of education.
In developing countries, the literature about the use of short message services in disease prevention and treatment is scarce. In a study in Ernaculum district of Kerala, authors assessed the potential of use of mhealth (mobile health) in management of cardiovascular diseases by exploring experiences and challenges of current CVD management, current mobile phone use and expectations of and barriers to mobile phone use in CVD management. They noted that lack of knowledge about diseases, difficulties in implementing primary prevention and poverty were the main barriers in use of mhealth for the improvement of health care.15 In another study it was observed that the cumulative incidence of type 2 diabetes was lower in those who received mobile phone messages than in controls.16 Pfammatter et al. demonstrated that participants receiving texts demonstrated greater improvement in health behaviour composite score over 6 months, compared with those who received no messages.17 In a systematic review, authors found that majority of published text-messaging interventions were effective when addressing diabetes self-management, weight loss, physical activity, smoking cessation, and medication adherence for antiretroviral therapy, and also emphasized that further studies are needed to focus on specific health behaviours and outcomes.18 We also agree that imparting health education is the need of the hour to create an impact on risk factor reduction and the incidence of cardiovascular diseases. The use of SMS related interventions for health education is still in its adolescence, and more research is needed with diverse study designs, health topics and study purposes so that these findings can be translated into best practices.
Limitations of the study included that the level of knowledge before SMS campaign was not assessed and regional language was not used for SMS campaign.
5. Conclusions
Mobile phones have become an integral part of our life and can act as important link in preventing diseases and promoting health. SMS related interventions can be used as an effective tool for providing health information about prevention of cardiovascular diseases in the community. The need of the hour is to tap the potential of this technology in disseminating the health information for bringing out behaviour change in the general population regarding health promotion and specific protection in relation to risk factors of CVDs.
Presentation at a meeting
Presented at CSI Cardiac Prevent 2015.
Conflict of interest
Nil.
Source(s) of support
Nil.
Appendix A.
See Fig. A1.
Fig. A1.

Map of Punjab.
Appendix B.
| 1. “80% of heart disease is preventable the power to have healthy hearts is in your hands” |
|---|
| 2. “Heart Patients who are on blood thinners should not stop medicines on their own” |
| 3. 30 mins. of brisk walk (5 km/h) reduces 30% risk of heart attacks in healthy individuals. Start walking and stay healthy” |
| 4. “Air pollution due to crackers increases the risk of respiratory problems and can worsen heart failure. So we should go for cracker free Diwali” |
| 5. 5 things which reduce cholesterol are green tea, soya, tomatoes, garlic and oats. Consume more for better health” |
| 6. “In summer, proper hydration with liquids is must but avoid cold drinks and alcohol. 1 glass of water 30 min before a meal helps digestion” |
| 7. “Avoid three whites “Maida”, sugar and extra salt to stay healthy” |
| 8. “Patient of hypertension and heart disease should take pain killers with caution as it can worsen the heart failure” |
| 9. “HYPERTENSION IS A SILENT KILLER.” Blood pressure lowering medicines should not be stopped without doctor’s advice. Control of blood pressure is must” |
| 10. “Papad, Pickle and Processed foods are high source of salt which increase the chances of hypertension, paralysis and heart attacks. Say no to three ‘P’s. |
| 11. “Avoid three “A” to stay Healthy and Happy. Anger, Aggression & Alcohol” |
| 12. “Regular use of cold drinks increases the risk of “Heart disease and Diabetes (Sugar)” by 20%. Give up now for better health” |
| 13. “Childhood obesity has doubled in last few decades. So, by adopting healthy eating habits and encouraging outdoor games one can lower the risk of obesity” |
| 14. “Swelling of feet is a marker of internal diseases like heart, kidney, and liver. Consult your physician” |
| 15. “In overweight people, 10% reduction of weight reduces risk of heart attack, stroke and hypertension. Keep your waist less than 90 cm in male and 80 cm in females” |
| 16. “Dose requirement of hypertensive and heart patients changes. So Get yourself checked to your doctor” |
| 17. “Repeated heating of oil produces dangerous chemicals that increase the risk of heart attacks. Avoid reheating of cooked food” |
| 18. “Children who take regular fast food are more likely to have high blood pressure and sugar in young age. Avoid fast food for better health” |
| 19. “Frequently use of pain killers like Brufen affects kidney and heart. Take it only when necessary” |
| 20. “First Time get your BP checked from both arms. Do not take coffee or tea 20 min & take rest for 5 min before BP check-up. Keep your BP below 140/90” |
| 21. “In case of paralytic attack due to clot, an emergency clot bursting drug given within 3 h can save many lives” |
| 22. “In winters, Incidents of paralytic attacks increases. So Check & control your blood pressure” |
| 23. “Eating regular fruits & Vegetables reduces the risk of heart & paralytic attacks by 15%. Start taking fruits and salads before every meal” |
| 24. “Not so sweet news – Regular use of cold drinks increases the risk of “Heart disease and Diabetes (Sugar)” by 20%. Give up now for better health” |
| 25. “Due to extreme weather, patients of heart failure & hypertension need to visit their respective physicians to avoid complications like dehydration & low sodium (salt) levels” |
| 26. “Childhood obesity can be an early marker of Diabetes, Hypertension & high cholesterol and can even lead to depression” |
| 27. “High blood pressure can occur at younger age group too. Obese children are at the risk for this” |
| 28. “In Summers, Dehydration not only causes fatigue and weakness but can also produce clot in the vessels of heart. So drink lots of water to avoid this” |
Appendix C.
| Questionnaire: |
|---|
| Q 1) Which food are good for lowering cholesterol except? |
| A) Milk B) Garlic C) Soya D) Green Tea |
| Q 2) When should we need to change BP medicines? |
| A) Change of Season B) Every Month |
| Q 3) Which white colored eatables to be avoided? |
| A) Sugar B) Salt C) Maida D) All of the above |
| Q 4) Is repeated heating of food a good or bad practice? |
| A) Good B) Bad |
| Q 5) Which is not a risk factor of heart disease? |
| A) Smoking B) Obesity C) Junk food D) Morning Walking |
| Q 6) Does salt increases blood pressure? |
| A) Yes B) No |
| Q 7) Do pain killers increase blood pressure? |
| A) Yes B) No |
| Q 8) What is the normal blood pressure? |
| Ans. 120/80 |
| Q 9) What are the benefits of regular walk? |
| A) Decreases heart attacks B) Increases blood pressure |
| Q 10) The following are important for blood pressure measurement except? |
| A) Rest for 5 min B) Avoid tea coffee before 20 min C) Check BP of both arms D) Check BP from right arm only |
| Q 11) Which diseases occur because of Childhood obesity? |
| A) Diabetes B) Hypertension C) High cholesterol D) All of the above |
References
- 1.Registrar General of India . Office of the Registrar General; New Delhi, India: 2015. Report on Medical Certification of Cause of Death 2013. [Available at: www.censusindia.gov.in/2011-document/mccd_2013.pdf (Last cited April 13, 2016)] [Google Scholar]
- 2.Gupta R., Mohan I., Narula J. Trends in Coronary heart disease epidemiology in India. Ann Global Health. 2016;82(2):307–315. doi: 10.1016/j.aogh.2016.04.002. [DOI] [PubMed] [Google Scholar]
- 3.Chan C.W., Chung J.W.Y. A survey of coronary heart disease knowledge in a sample of Hong Kong Chinese. Asia Pac J Public Health. 2011;23:288–297. doi: 10.1177/1010539509345869. [DOI] [PubMed] [Google Scholar]
- 4.Pandey R., Khadka I. Knowledge regarding preventive measures of heart disease among the adult population in Kathmandu. Health (N Y) 2012;4:601–606. [Google Scholar]
- 5.Kaplan W.A. Can the ubiquitous power of mobile phones be used to improve health outcomes in developing countries? Global Health. 2006;2:9. doi: 10.1186/1744-8603-2-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fjeldsoe B.S., Marshall A.L., Miller Y.D. Behavior change interventions delivered by mobile telephone short-message service. Am J Prev Med. 2009;36(2):165–173. doi: 10.1016/j.amepre.2008.09.040. [DOI] [PubMed] [Google Scholar]
- 7.Déglise Carole, Suzanne Suggs L., Odermatt Peter. Short message service (SMS) applications for disease prevention in developing countries. J Med Internet Res. 2012;14(1):e3. doi: 10.2196/jmir.1823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Piette John D., List J., Rana G.K., Townsend W., Striplin D., Heisler M. Mobile health devices as tools for worldwide cardiovascular risk reduction and disease management. Circulation. 2015;132:2012–2027. doi: 10.1161/CIRCULATIONAHA.114.008723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Franklin V., Waller A., Pagliari C. Sweet Talk: text messaging support for intensive insulin therapy for young people with diabetes. Diabetes Technol Ther. 2003;5(6):991–996. doi: 10.1089/152091503322641042. [DOI] [PubMed] [Google Scholar]
- 10.Neville Ron, Greene Alexandra, McLeod John, Tracy Andrew. John Surie Mobile phone text messaging can help young people manage asthma. BMJ. 2002;325(7364):600. doi: 10.1136/bmj.325.7364.600/a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chow Clara K., Redfern Julie, Hillis Graham S. Effect of lifestyle-focused text messaging on risk factor modification in patients with Coronary heart disease a randomized clinical trial. JAMA. 2015;314(12):1255–1263. doi: 10.1001/jama.2015.10945. [DOI] [PubMed] [Google Scholar]
- 12.Free Caroline, Phillips Gemma, Galli Leandro. 2017. The Effectiveness of Mobile-Health Technology-Based Health Behaviour Change or Disease Management Interventions for Health Care Consumers: a Systematic Review. [Available at http://dx.doi.org/10.1371/journal.pmed.1001362 (last cited on October 20, 2016)] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Neville Ron, Greene Alexandra, McLeod John, Tracy Andrew, Surie John. Mobile phone text messaging can help young people manage asthma. BMJ. 2002;325(7364):600. doi: 10.1136/bmj.325.7364.600/a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gonzales Rachel, Douglas Anglin M., Deborah C. Glik Exploring the feasibility of text messaging to support substance abuse recovery among youth in treatment. Health Educ Res. 2014;29(1):13–22. doi: 10.1093/her/cyt094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Smith R., Menon J., Rajeev J.G., Feinberg L., Kumar R.K., Banerjee A. Potential for the use of mHealth in the management of cardiovascular disease in Kerala: a qualitative study. BMJ Open. 2015;5:e009367. doi: 10.1136/bmjopen-2015-009367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ramachandran A., Snehalatha C., Ram J. Effectiveness of mobile phone messaging in prevention of type 2 diabetes by lifestyle modification in men in India: a prospective, parallel-group, randomised controlled trial. Lancet Diabetes Endocrinol. 2013;1(3):191–198. doi: 10.1016/S2213-8587(13)70067-6. [DOI] [PubMed] [Google Scholar]
- 17.Pfammatter A., Spring B., Saligram N. MHealth intervention to improve diabetes risk behaviors in India: a prospective, parallel group cohort study. J Med Internet Res. 2016;18(8):e207. doi: 10.2196/jmir.5712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hall Amanda K., Cole-Lewis Heather, Bernhardt Jay M. Mobile text messaging for health: a systematic review of reviews. Annu Rev Public Health. 2015;18(36):393–415. doi: 10.1146/annurev-publhealth-031914-122855. [DOI] [PMC free article] [PubMed] [Google Scholar]