

Colonoscopy is a widely used diagnostic and therapeutic intervention. The procedure is usually well tolerated, with less than 0.5% of patients developing bowel perforation. Perforation usually manifests soon after the procedure with generalised abdominal pain. We present the case of a near fatal complication after colonoscopy in which the initial features suggested bowel perforation but further investigation showed an unsuspected cause that necessitated urgent surgery.
Figure 1.
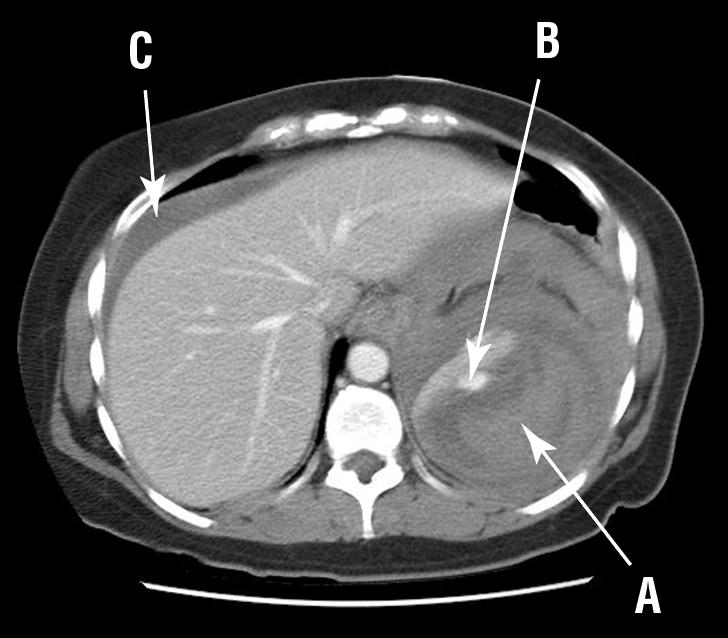
Computed tomogram showing intrasplenic haematoma (A), extravasating contrast indicating active bleeding (B), and haemoperitoneum (C)
Case report
A 47 year old woman presented to our emergency department 24 hours after colonoscopy with left shoulder tip and abdominal pain. Her abdominal pain felt like “trapped wind,” becoming progressively worse throughout the day. Two weeks previously, she had had hysteroscopy and laparoscopy to investigate menorrhagia and had been diagnosed with endometriosis. Colonoscopy was performed to exclude colonic involvement. She had been given 5 mg intravenous diazepam for sedation, and colonoscopic diathermy or biopsy had not been used. She had insulin dependent type 2 diabetes, with hypertension and hyperlipidaemia.
On examination she was pale, but vital signs were normal. Her lower abdomen was tender, with normal bowel sounds and no abdominal distension. Initial blood tests showed a haemoglobin concentration of 76 g/l (normal range 110-160 g/l). Colonic perforation after colonoscopy was suspected, yet there was no evidence of free air on erect chest and abdominal radiographs. Additionally, she had no history of rectal bleeding. Her abdominal pain seemed to resolve, and discharge was considered. However, soon her abdominal pain increased, warranting urgent abdominal computed tomography. This showed active bleeding within an intrasplenic haematoma, and a large haemoperitoneum, presumably secondary to splenic rupture (figure). The splenic hilum appeared intact.
Initially she was haemodynamically stable and was transferred to the high dependency unit, where we started a transfusion of 4 units of packed red cells. Her haemoglobin concentration increased to 132 g/l. Two hours later, however, her abdominal pain worsened, and she developed hypotension and tachycardia. An urgent laparotomy was done. There was active bleeding from the splenic pedicle, with more than three litres of intraperitoneal blood present. We performed a splenectomy and ligated the bleeding vessels. After the operation she made steady progress, being discharged on the eighth postoperative day after receiving prophylactic vaccination for encapsulated organisms. Serological testing for Epstein-Barr virus was negative, and the spleen was histologically normal.
Discussion
This case highlights the difficulty in diagnosing unsuspected trauma to the spleen. Our patient presented with lower abdominal pain, whereas most patients with splenic rupture after colonoscopy have pain localised to the left upper quadrant.1 Our patient also had pain radiating to the left shoulder tip (Kehr's sign). This sign is present, however, in about half of patients after uncomplicated colonoscopy, so it has little discriminating value.
More than 30 cases of splenic rupture after colonoscopy have been reported.2 The incidence of minor splenic injury after colonoscopy is probably higher, however, as the diagnosis may not be clinically apparent, and less severe splenic injuries might not have been reported in the literature. As seen in our patient, the onset of abdominal pain is usually within 24 hours of colonoscopy,1 although cases have been diagnosed up to 10 days later. This may reflect delayed diagnosis of an under-recognised complication of colonoscopy.
Computed tomography is the best imaging procedure for diagnosing splenic injuries. Grading scales based on computed tomography findings can predict the likelihood of successful non-operative management, which is often possible if the splenic hilum is intact (even when capsular disruption is present).3 However, intraobserver and interobserver reliability for high grade splenic injuries is low, and experienced radiologists often underestimate the magnitude of injury.4 As our case shows, grading scales may have less predictive power on an individual basis: because the splenic capsule and hilum appeared intact and the patient was haemodynamically stable, we initially opted for non-operative management.
Factors that predict failure of non-operative management include persistent haemodynamic instability; underlying disease within the spleen; splenic trauma grade 3 or above, according to the American Association for Surgery Trauma classification; haemoperitoneum shown on computed tomography; and extremes of age.5 Some studies suggest that non-operative management of high grade injuries is likely to fail if more than one unit of blood transfusion is required.6 Had we applied these criteria to our case, we would have realised that non-operative management was likely to fail.
Concerns about the risk of developing overwhelming post-splenectomy infection (about 1% for adults) have fuelled a recent trend towards conservative management of splenic trauma.7 Failure rates of non-operative management as low as 10% have recently been reported,6 although this may be due partly to increased detection of less severe injuries as abdominal imaging becomes more widespread. It is important to note that conservative management may require more blood transfusion than operative intervention,6 so the risks associated with transfusion must be balanced against the risks of overwhelming post-splenectomy infection if splenic conservation is being considered.
Conditions predisposing to splenocolic adhesions (previous abdominal surgery; pancreatitis; or inflammatory bowel disease) may increase the risk of splenic trauma after colonoscopy owing to decreased mobility between the spleen and colon. Partial capsular avulsion after traction (during polypectomy or biopsy) is the postulated mechanism. Direct trauma to the spleen during colonoscopy may also cause splenic rupture,1 as may technical manoeuvres that produce excessive torsion on the splenocolic ligament during colonoscopy.2 Splenomegaly or underlying splenic diseases may have an important role.
As the indications for colonoscopy expand—including the introduction of mass screening for colorectal cancer—physicians should be increasingly aware of the possibility of splenic injury after colonoscopy. Splenic injury should be considered if patients become haemodynamically unstable after colonoscopy, once bowel perforation or rectal bleeding is excluded.
Consider splenic trauma as a cause of abdominal pain after colonoscopy, once perforation is excluded
Contributions: SEJJ looked after the patient, had the initial idea, and drafted the paper. IAC did the computed tomography. BD did the laparotomy. IAC and BD critically reviewed the paper. BD is the guarantor.
Funding: None.
Competing interests: None declared.
References
- 1.Ahmed A, Eller PM, Schiffman FJ. Splenic rupture: an unusual complication of colonoscopy. Am J Gastroenterol 1997;92: 1201-4. [PubMed] [Google Scholar]
- 2.Holzer K, Thalhammer A, Bechstein WO. Splenic trauma a rare complication during colonoscopy. Z Gastroenterol 2004;42: 509-12. [DOI] [PubMed] [Google Scholar]
- 3.Williams RA, Black JJ, Sinow RM, Wilson SE. Computed tomography assisted management of splenic trauma. Am J Surg 1997;174: 276-9. [DOI] [PubMed] [Google Scholar]
- 4.Barquist ES, Pizano LR, Feuer W, Pappas PA, McKenney KA, LeBlang SD, et al. Inter- and intrarater reliability in computed axial tomographic grading of splenic injury: why so many grading scales? J Trauma 2004;56: 334-8. [DOI] [PubMed] [Google Scholar]
- 5.Tsugawa K, Koyanagi N, Hashizume M, Ayukawa K, Wada H, Tomikawai M, et al. New insight for management of blunt splenic trauma: significant differences between young and elderly. Hepatogastroenterology 2002;49: 1144-9. [PubMed] [Google Scholar]
- 6.Velmahos GC, Chan LS, Kamel E, Murray JA, Yassa N, Kahaku D, et al. Nonoperative management of splenic injuries: have we gone too far? Arch Surg 2000;135: 674-9. [DOI] [PubMed] [Google Scholar]
- 7.Reihner E, Brismar B. Management of splenic trauma-changing concepts. Eur J Emerg Med 1995;2: 47-51. [DOI] [PubMed] [Google Scholar]