

Dear Editor,
A 30-year-old female presented to the dermatology clinic with complaints of severe pain on slight pressure on the left middle finger. The pain exaggerated on cold exposure. On local examination, there was bluish tinge seen under the nail plate at the terminal phalanx of the left middle finger and Love's sign was elicited. The patient was advised magnetic resonance imaging (MRI), which on axial/T2W/PDSF/sagittal images of the terminal phalanx of the left middle finger at nail bed region showed focal midline hyperintensity measuring approximately 5 mm × 3 mm size [Figure 1] with mild cortical scalloping of underlying terminal phalanx. A small intramedullary bone cyst was also seen at metacarpal bone (distal level) of the left middle finger (incidental finding) [Figure 2]. Histopathology was consistent with glomus tumour [Figure 3]. Orthopaedic consultation for bone cyst of metacarpal bone of the left middle finger was done.
Figure 1.

On magnetic resonance imaging, images of terminal phalanx of the left middle finger at nail bed region show focal midline hyperintensity measuring approximately 5 mm × 3 mm size (circled with red marker). A small intramedullary bone cyst is also seen at metacarpal bone (distal level) of the left middle finger (incidental finding)
Figure 2.
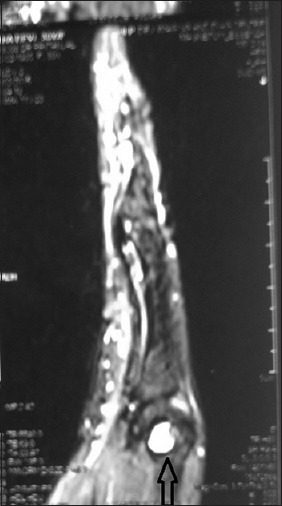
On magnetic resonance imaging, a small intramedullary bone cyst is also seen at metacWarpal bone (distal level) of the left middle finger (marked with an arrow)
Figure 3.

Sheets of monomorphic round cells with pale to eosinophilic cytoplasm having well-defined margin (H and E, ×40)
The digit to be operated was anaesthetized with proximal nerve block using the 2% lignocaine. Tourniquet was applied for having an avascular operating field. The nail plate was removed with the help of a Freer elevator. Glomus tumour was then visualised after removal of the nail plate [Figure 4]. The lesion was then excised and later cauterised, and pressure dressing was done. The patient was given antibiotics and anti-inflammatory drugs for one week. The patient was called for follow-up after 24 h to recheck for any bleeding, and on the 8th post-operative day, dressing was removed.
Figure 4.

Glomus tumour was then visualised after removal of the nail plate
DISCUSSION
Glomus tumour is an uncommon hamartoma arising from glomus bodies which are arteriovenous shunts present mainly in digits and are composed of endothelium-lined vascular spaces (Sucquet-Hoyer canal) surrounded by glomus cells.[1] It usually presents as bluish/red papules or nodules located in the dermis. Glomus tumours most commonly affect patients in the third to fifth decades of life, as were also seen in our study, although cases have been described in all age groups.[2] The lesion is tender to slight touch and at times may be associated with severe paroxysmal pain in response to cold exposure and pressure. Mostly located in the nail beds and palm, but other cutaneous locations have also been reported. Cold sensitivity is the most accurate test (100%) aiding in diagnosis of glomus tumour after reviewing different clinical tests.[3] MRI being a non-invasive technique has proven to be one of the most sensitive methods for diagnosis of glomus tumour and also delineating the tumour size and location preoperatively. Excision is the treatment of choice.
Simple bone cyst is benign cystic lesions seen commonly in skeletally immature persons. Males are twice more commonly affected than females.[4] Common sites of occurrence are femur and humerus.[4] Hand is a very rare site of occurrence. Treatment options for simple bone cyst include observation, curettage, bone grafting and intralesional steroid injection.[4]
To the best of our knowledge, this is the first case report where subungual glomus tumour on the terminal digit of the left middle finger with intramedullary bone cyst of metacarpal head of the left middle finger is being reported.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Murthy PS, Rajagopal R, Kar PK, Grover S. Two cases of subungual glomus tumor. Indian J Dermatol Venereol Leprol. 2006;72:47–9. doi: 10.4103/0378-6323.19719. [DOI] [PubMed] [Google Scholar]
- 2.Song M, Ko HC, Kwon KS, Kim MB. Surgical treatment of subungual glomus tumor: A unique and simple method. Dermatol Surg. 2009;35:786–91. doi: 10.1111/j.1524-4725.2009.01129.x. [DOI] [PubMed] [Google Scholar]
- 3.Girisha BS, Shenoy MM, Mathias M, Mohan R. Glomus tumor of the nail unit. Indian J Dermatol. 2011;56:583–4. doi: 10.4103/0019-5154.87163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wilkins RM. Unicameral bone cysts. J Am Acad Orthop Surg. 2000;8:217–24. doi: 10.5435/00124635-200007000-00002. [DOI] [PubMed] [Google Scholar]