

Abstract
INTRODUCTION:
Cardiovascular diseases are the leading cause of death all over the world. Lifestyle can have an important role not only in reducing risk factors but also in the prevention and treatment of coronary heart diseases. The aim of this study was to examine the relationship between clinical parameters and various aspects of patients’ lifestyles according to the severity of their coronary artery stenosis.
MATERIALS AND METHODS:
This study was a descriptive, analytic study carried out on 220 patients undergoing coronary angiography at Mazandaran Heart Center. Based on the angiography results, patients were divided into two groups: artery stenosis > 50% (110 cases) and < 50% (110). Patients’ lifestyles were evaluated using health-promoting behavior questionnaire. Blood pressure and triglyceride, low-density lipoprotein, high-density lipoprotein, cholesterol, and fasting blood sugar were also measured. After collecting data, SPSS 21 software, Chi-square test, t-test, and multiple linear regression were used for analysis of the data.
RESULTS:
The results showed that in patients with positive angiographic data, there is a significant correlation between clinical parameters and dimensions of health-promoting behavior (P < 0.05).
CONCLUSION:
Given the impact of clinical parameters on various aspects of lifestyle, it seems that by teaching the different aspects of lifestyle (such as having a healthy diet consisting of fresh fruits and vegetables, reducing intake of saturated fat, physical activity and regular exercise, stress management, and blood pressure control) to patients with a positive angiographic result, we can improve their lifestyles by means of improving clinical parameters.
Keywords: Angiography, cardiovascular diseases, health-promoting behavior, lifestyle
Introduction
Globally, cardiovascular diseases (CVDs) are the leading cause of death. About 17.5 million people lost their lives in 2012 due to CVDs.[1] The majority of deaths from CVDs occur in low- and middle-income countries, and it is estimated that by 2030, more than 23 million people will lose their lives due to CVD.[2] According to the World Health Organization report, this disease has been the leading cause of death in Iran in 2014, and by causing 46% of total adult mortality, it is known as the primary cause of death.[3] The death rate due to coronary artery disease in Iran is 179.6 in 100,000, and it has been ranked 25th in the world.[4] Several factors play roles in the development of CVDs, some of which cannot be modified such as male gender, age, and inheritance and some are modifiable. Modifiable factors include smoking, physical inactivity, unhealthy diet, alcohol consumption, obesity, hypertension, dyslipidemia, diabetes, and stress.[1,5] However, preventing and controlling these risk factors and adopting a healthy lifestyle have reduced the disease burden caused by coronary heart disease (CHD) in many countries.[6]
Unhealthy lifestyle has a significant impact on people's health. More than 50% of cancers and more than 40% of circulatory diseases are of heart diseases associated with lifestyle. It is estimated that about 31% of CVDs are due to poor diet (low fruit and vegetable consumption) and 22% due to physical inactivity, and over 22% is related to smoking.[7] High blood pressure, dyslipidemia, diabetes, and obesity are usually the manifestations of physical inactivity and unhealthy diet and are often known as metabolic risk factors of CVDs.[8] One of the main factors in reducing deaths caused by CVDs is adopting healthy lifestyle behavior. This is the reason why people should include health-promoting behavior in their daily lives.[9] In fact, lifestyle consists of a set of daily life behaviors that affect people's health and include behaviors such as nutrition, physical activity, and responsibility for one's health, stress management, interpersonal relationships, and spiritual growth.[10] Lifestyle can play an important role not only in reducing risk factors but also in effective prevention and treatment of CHD.[11] Thus, interventions to promote healthy lifestyle in the general population are considered as a useful and cost-effective method for primary prevention.[12] The American Heart Association has considered Healthy Heart Program until 2020 for a 20% reduction in mortality from CVD and stroke that includes seven health behaviors: lean body mass, quitting smoking, physical activity, healthy diet, total cholesterol <200 mg/dl, blood pressure <120/80 mmHg, and fasting blood glucose <100 mg/dl.[13] The likelihood of showing CVD signs decreases in people who reduce the risk factors.[14] To control amendable heart risk factors and to improve the adoption of healthy behaviors, one can try to improve public knowledge about CHDs and lead them to adopt a healthy lifestyle through counseling and behavioral interventions.[15] Therefore, considering the importance of lifestyle and its effect on the prevention of CHD and maintaining individuals’ health, this study has examined the relationship between clinical parameters and various aspects of patients’ lives according to the severity of their coronary artery stenosis to provide the needed educational grounds for the correct lifestyle of heart disease patients.
Materials and Methods
This study was a descriptive and analytic study carried out in 2015 among patients of angiography in Mazandaran Heart Center. The purpose is to investigate the relationship between clinical parameters and various aspects of lifestyle of patients according to the severity of coronary artery stenosis (narrowing of the arteries more than 50%). Sampling was purposive and convenient which was carried out for 3 months starting in April 2015 and ending in June 2015. Two hundred patients took part in this study of whom 110 patients were placed in the positive angiography group (stenosis of more than 50%) and 110 in negative angiography group (stenosis <50%). Inclusion criteria included age over 18 years, willingness to participate in research, having no speech and hearing difficulties, not being in an emergency situation, full consciousness at the time of research, and no physical diseases, mental disorders, and mental disabilities. A two-part questionnaire was used to collect data in this study: the first section included demographic questions (age, sex, level of education, occupation, and place of residence) and the second part included health-related variables (history of smoking, history of hypertension, and history of diabetes) that were completed based on self-report and using the information from the patients’ records. The second part included questions related to health-promoting behaviors of patients investigated using Health Promoting Lifestyle Profile 2 questionnaire designed by Walker et al. in 1987 This scale has high reliability and validity (Cronbach's alpha 0.87).[16] This tool has been tested in many countries throughout the world; the Persian Version of this questionnaire has been standardized in Iran and its validity and reliability are approved.[17,18] This scale measures health-promoting behaviors in six aspects: Health responsibility (nine items), physical activity (following a pattern of regular exercise with eight questions), nutrition (having a dietary pattern and food choices with nine questions), spiritual growth (feeling satisfied and purposefulness with nine questions), stress management (identifying sources of stress and stress management measures with eight questions), and interpersonal relations (nine items). The whole questionnaire contains 52 questions scored based on four-option Likert as never (1), sometimes (2), often (3), and always (4). The total score ranges between 52 and 208, where separate scores are calculated for each aspect of health-promoting behaviors, so the range of scores of responsibility, nutritional status, spiritual growth, and interpersonal relations was considered as 0–36 and 0–32 for each aspect of stress management and physical activity. Higher scores indicate adopting healthier lifestyle behavior. Blood pressure was measured twice; once in a sedentary position from the right hand and then after at least 5 min rest using a mercury manometer device based on Joint National Committee VII criteria, and the averages of these two were considered as the patients’ blood pressure. People with systolic blood pressure equal to 140 or greater, diastolic blood pressure equal to 90 or greater, or those with diagnosed high blood pressure, using antihypertensive drugs were classified as patients with high blood pressure.[19] To measure glucose and blood lipid levels, blood samples were taken after 12 h of fasting during the night. The tests included measurement of triglyceride (TG), high-density lipoprotein (HDL), cholesterol, and fasting blood sugar (FBS) and were carried out in enzymatic method using Pars Azmoon kits and Beckman's autoanalyzer device - Model CX4, and low-density lipoprotein (LDL) were calculated using Friedewald formula (LDL-cholesterol [LDL-C] = Total cholesterol – HDL-cholesterol [HDL-C] − TG/5 [mg/dl]).[20] To define diabetes, American Diabetes Association's criteria were used and those with FBS >126 mg% of those who had diabetes history and consumed hypoglycemic drugs were considered as diabetic patients.[21]
Classification of the amount of lipids was based on the National Cholesterol Education Program and total cholesterol equal to or more than 200 mg/dL was considered as hypercholesterolemia. Patients with TGs above 150 mg/dL, LDL-C equal to or >160 mg/dL, and HDL-C ≤40 mg/dL were considered as dyslipidemia.[22] Two cardiologists determined the severity of coronary artery stenosis in all participants in this study. In the first stage, one of two cardiologists determined the severity of coronary artery stenosis through visual method, and then in the next stage, the other cardiologists reviewed angiography videos to increase the accuracy of diagnosis. At the end, each patient was placed in one of the groups (more than 50% and ≤50%) based on the severity of coronary artery stenosis. Ethical approval for this study was obtained from the Research Ethic Committee of Tehran University of Medical Sciences. The purposes of the study were explained to the participants, and all the patients had signed the informed consent. The participants were free to continue or give up the procedures at any time during the study. They were assured of the confidentiality of their information.
To comply with ethical considerations, we asked for permission from Mazandaran Heart Center Hospital officials. To gather data, questionnaires along two of the researchers referred to the patients in person. After the introduction and expressing the aim of the study and ensuring that the information will remain confidential and the results will be used in the overall form of a scientific paper, the questionnaires were handed to the participants to complete, and the questionnaires were completed anonymously. It should be noted that patients who did not have the ability to complete the questionnaires responded to questions with the help of trained interviewers during individual interviews, and when necessary, the researchers referred to the patients’ records and extracted the necessary information. After collecting the data, (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, V.21.0, IBM Corp., Armonk, New York, USA) Chi-square test, t-test, and multiple linear regression were used to analyze the data.
Results
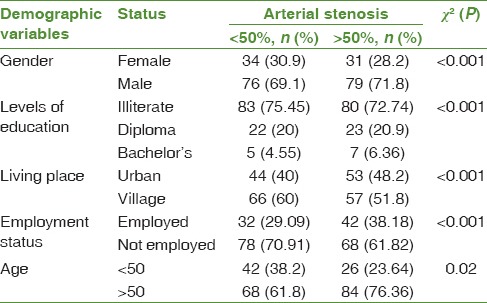
In Table 1, absolute frequency and relative frequency of the patients participating in the study based on demographic variables such as gender, level of education, location, occupation, and age group are shown. The results showed that with respect to patients with coronary artery stenosis above 50% compared with patients with stenosis <50%, men were more than women (71.8% vs. 69.1%), urban residents more than rural residents (48.2% vs. 40%), and unemployed people more than employed. The Chi-square test also showed that the difference between the demographic characteristics of the two groups is statistically significant (P < 0.05).
Table 1.
Frequency of patients in terms of demographic variables
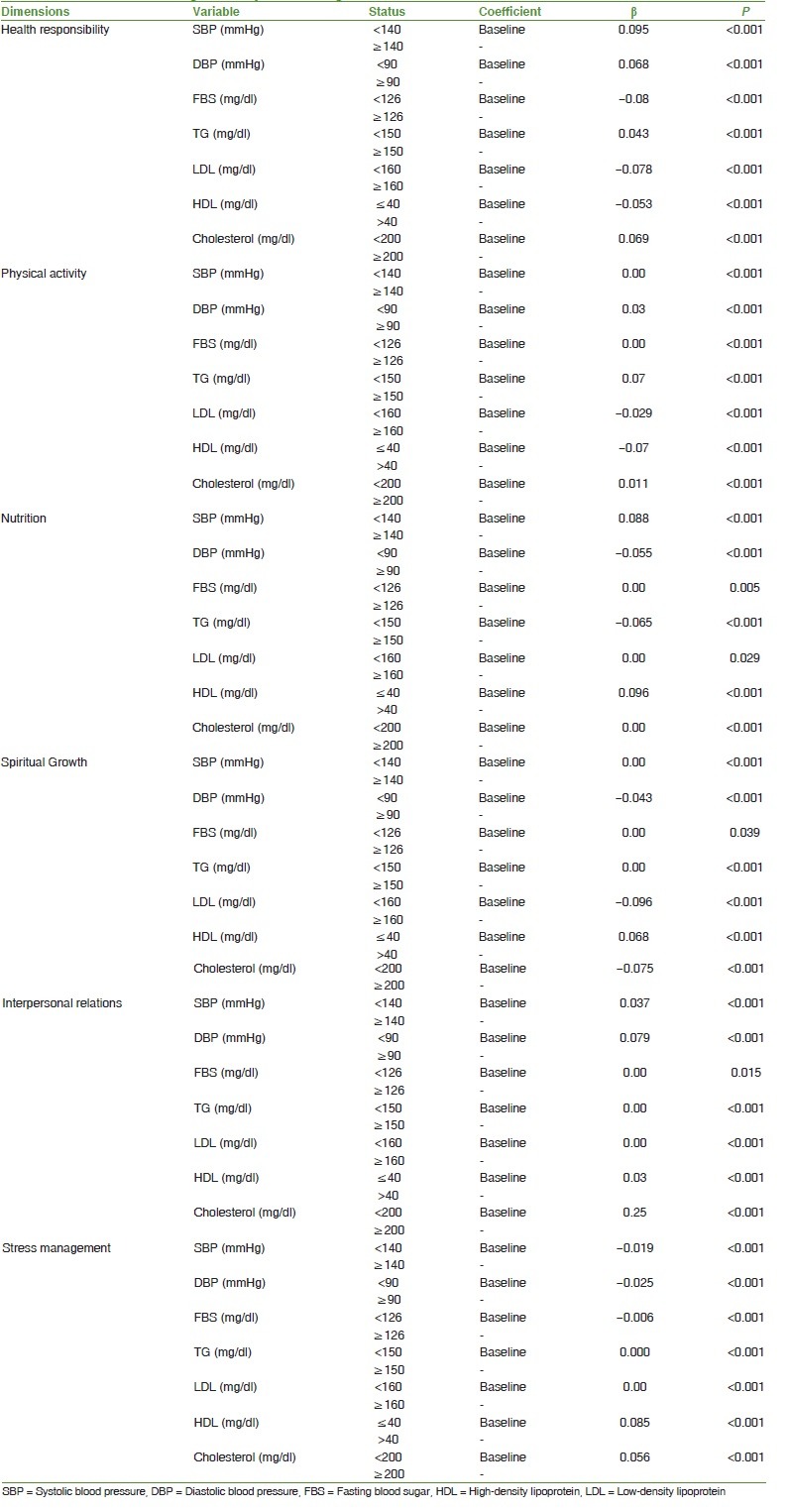
The relationship between health-promoting behaviors of lifestyle with the severity of coronary artery stenosis among patients referring to angiography was analyzed using t-test mean comparison. The results showed that there is a significant relationship between lifestyle aspects of health-promoting behaviors with intensity of coronary artery stenosis; the average score of health responsibility, physical activity, dietary habits, spiritual health, stress management, and the total score of health-promoting behaviors among patients with coronary artery stenosis more than 50% is lower in patients with coronary artery stenosis <50% [Table 2]. Because of the relationship between the aspects of health-promoting lifestyle behaviors with severity of coronary artery stenosis in patients above 50%, and also due to positive angiography patients’ being in the high-risk patients group, in the second stage of analysis, the relationship between paraclinical variables (systolic blood pressure, diastolic blood pressure, FBS, TGs, LDL, and HDL) and lifestyle aspects of health-promoting behaviors (health responsibility, nutrition, physical activity, spiritual growth, interpersonal relationships, and stress management) in patients with stenosis more than 50% was analyzed using multiple linear regressions. The results showed that there is a significant correlation between paraclinical variables and lifestyle aspects of health-promoting behaviors (P < 0.05) so that for every unit increase in the amount of paraclinical variables, β extent is added to or reduced from the average size of lifestyle aspects of health-promoting behaviors [Table 3].
Table 2.
The relationship between health-promoting behaviors of lifestyle with the severity of coronary artery stenosis
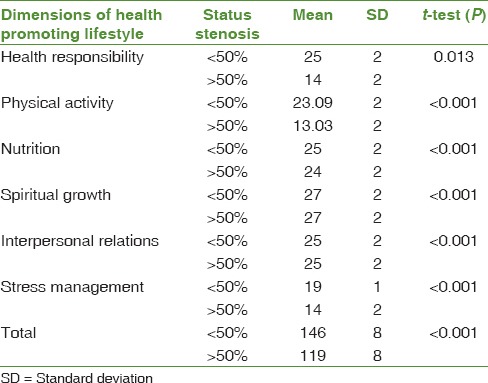
Table 3.
Results of the fitting of multiple linear regression
Discussions
Lifestyle is a dynamic chain in all aspects of human life and plays an important role in people's health, which being adjusted, the risk of many diseases, particularly CVDs, can be reduced. Therefore, in this study, different aspects of lifestyle and their relationship with clinical parameters in patients with positive and negative angiography were evaluated.
According to preliminary results of the study, the average score of all aspects of health-promoting behaviors in patients with positive angiography was lower than that of patients with negative angiography that can indicate that patients with coronary artery stenosis >50% have an unhealthier lifestyle and this has had an effect on their positive coronary angiography. In this regard, the studies based on health promotion interventions were investigated. In this regard, a study conducted by Lin and Chu in the evaluation of health promotion lifestyle associated with a regular exercise and diet program between the two groups of adult rural population (207 adults who have had such a program and 185 adults who have not) using Health-Promoting Lifestyle Profile Short Form questionnaire (HPLP-S) showed that the total score of health-promoting behaviors in the group that had a regular exercise and nutrition program is higher than those who did not have such a program in their daily lives.[23] Lin et al. (2010) conducted a study to evaluate the health-promoting lifestyle with exercise and nutrition program in patients with metabolic syndrome in Taiwan. In this study, lifestyle was measured using HPLP-S. Based on the results, the total score of health-promoting behaviors and its six aspects were significantly higher in the group with a regular exercise program and diet than the group who did not have such a program in their daily lives. Certainly, wrong foods, lack of exercise and bad mechanical lifestyle cause obesity, hypertension, diabetes, and eventually CVDs. The researchers believe that modifying lifestyle can have an impact on the reduction of obesity and blood pressure, and can reduce the risk of CVD.[24,25,26] Therefore, it reflects the vital role of a healthy lifestyle in reducing the burden of CVDs and the need for further intervention in this regard.
Bi et al. conducted a study to investigate the relationship between lifestyle factors and good health on 12,429 Chinese students. In the study, Health Promoting Lifestyle Profile 2 and Subhealth Measurement Scale questionnaires were used to collect data. The findings of the study showed that there is a significant correlation between health status with dimensions of spiritual growth, physical activity, responsibility, relationships, and stress management.
The average score for each aspect of health-promoting lifestyle behavior among participants who reported their health situation as “sick” was lower than the students who saw their health status as high. Adopting a healthy lifestyle can improve health. Hence, unhealthy lifestyle is seen as a risk factor for suboptimal health status.[27] In this study also, the mean score of different aspects of health-promoting behaviors in patients with positive angiography was lower than that of patients with negative angiography. Therefore, it can be said that the results of the present study are in line with those of Bi et al.
One of the main objectives of this study was to determine the relationship between different aspects of health-promoting lifestyle behaviors and clinical parameters in patients with positive angiographic results. In this study, the results of multiple linear regression showed that there is a significant correlation between paraclinical variables and aspects of lifestyle with health-promoting behaviors (P < 0.05), and hyperlipidemia, hypertension, and hypoglycemia have had an effect on reducing average aspects of health-promoting lifestyle behaviors. In this regard, several studies have been conducted of which the study by Kim et al. (2015) can be noted where the lifestyle and the risk of CVDs factors of 118 students were studied. The findings of the study showed that the lifestyle of the students was moderate. The most common risk factor for CVD belonged to high blood fat (26.3%), followed by overweight/obesity (25.4%), hypertension (17.8%), and high fasting blood sugar (5.1%). More than half of students (54.2%) had one or more of heart risk factors, and their lifestyle scores were significantly lower than those of other students.[28]
In a study by Chiou et al. to investigate the factors influencing health-promoting behavior and the relationship between health-promoting behaviors and the metabolic syndrome in Taiwan on 213 elderly people, people's lifestyle was measured by Health Promoting Lifestyle Profile 2 and their blood pressure, body mass index, and blood sugar and cholesterol were measured. The results showed that 3% of metabolic syndrome was predictable by health-promoting behavior. Moreover, the participants had the highest scores in aspects of interpersonal relations and stress management of health-promoting behaviors, and the lowest scores were obtained in aspects of physical activity and spiritual growth. Whereas in the present study, the highest scores were, respectively, allocated to the dimensions of spiritual growth, interpersonal relationships, and nutrition, and the lowest scores were obtained in health responsibility, stress management, and physical activity.[29] On the other hand, in a case study by Lin et al., which aimed to assess the effect of lifestyle modification on metabolic risk factors showed that lifestyle modification programs can be effective in reducing the amount of TGs, waist circumference, and systolic blood pressure levels.[30] In addition, in the study by Sutherland (2014) that was carried out to investigate the relationship between risk factors of metabolic syndrome and health behaviors among 225 men and women in Latin America, there was no statistically significant difference between the aspects of HPLP-II and paraclinical variables (blood pressure, blood fat, and glucose), except for physical activity.[31]
The limitations of this study can be mentioned that the study was designed to assess lifestyle through self-administered questionnaires. Other limitation of this study was to allow the participants reporting their own lifestyle levels which might have been lower or higher than the actual level.
It can be concluded that given the impact of clinical parameters on various aspects of lifestyle, interventional and educational plans play an important role in encouraging patients to promote their health through changing their lifestyles.
Further studies are recommended to be conducted under the same title in other cities, and other the health-related variables of patients should be compared according to their different cultural and environmental situations. Furthermore, it is recommended to do some quantitative and qualitative research to identify barriers and facilitators of the health-promoting lifestyle in patients with heart disease.
Conclusion
People with stenosis <50%, have experienced hospitalization and angiography so that they understand the threat posed by CVD better than others, and thus they tend to change their behavior. Therefore, with motivational approaches, we can persuade the patients to change their behaviors and adopt a healthy lifestyle. Unhealthy lifestyle choices that lead to poor health also increase the risk of disease in people. The results of this study show the importance of health-promoting lifestyle and coronary artery stenosis risk factor management among patients. Thus, health promotion and education programs at the community level might increase knowledge of the public about heart disease and expectantly delay the development of CVDs. It seems that by educating patients, with a positive angiographic result, in different aspects of lifestyle including using a healthy diet such as fresh fruits and vegetables, reducing intake of saturated fat, physical activity and regular exercise, stress management training, and blood pressure control, we can improve clinical parameters to improve people's lifestyles.
Financial support and sponsorship
This work was financially supported by Tehran University of Medical Sciences, Tehran, Iran.
Conflicts of interest
There are no conflicts of interest.
References
- 1.World Health Organision. Cardiovascular Diseases (CVDs) 2015. [Last accessed on 2016 Apr 20]. Available from: http://www.who.int/mediacentre/factsheets/fs317/en/
- 2.Simoska E. Healthy Lifestyle in the Prevention of Heart Disease and Diabetes: A Literature Review [Dissertation] Finland: Seinäjoki University of Applied Sciences; 2012. [Google Scholar]
- 3.World Health Organision. Noncommunicable Diseases Country Profiles 2014. 2014. [Last accessed on 2016 Apr 20]. Available from: http://www.who.int/nmh/publications/ncd-profiles-2014/en/
- 4.World Life Expectancy. Coronary Heart Disease. 2014. [Last accessed on 2016 Apr 20]. Available from: http://www.worldlifeexpectancy.com/
- 5.American Heart Association. Understand Your Risk of Heart Attack. 2015. [Last accessed on 2016 Apr 20]. Available from: http://www.heart.org/HEARTORG/Conditions/HeartAttack/UnderstandYourRiskofHeartAttack/Understand-Your-Risk-of-Heart-Attack_UCM_002040_Article.jsp#.VxdtYXrZYTg .
- 6.Fakhrzadeh H, Bandarian F, Adibi H, Samavat T, Malekafzali H, Hodjatzadeh E, et al. Coronary heart disease and associated risk factors in Qazvin: A population-based study. East Mediterr Health J. 2008;14:33–41. [PubMed] [Google Scholar]
- 7.Sanderson SC, Waller J, Jarvis MJ, Humphries SE, Wardle J. Awareness of lifestyle risk factors for cancer and heart disease among adults in the UK. Patient Educ Couns. 2009;74:221–7. doi: 10.1016/j.pec.2008.08.003. [DOI] [PubMed] [Google Scholar]
- 8.Mendis S, Puska P, Norrving B. Global Atlas on Cardiovascular Disease Prevention and Control. Geneva: World Health Organization; 2011. [Google Scholar]
- 9.Eshah NF. Lifestyle and health promoting behaviours in Jordanian subjects without prior history of coronary heart disease. Int J Nurs Pract. 2011;17:27–35. doi: 10.1111/j.1440-172X.2010.01902.x. [DOI] [PubMed] [Google Scholar]
- 10.Pender NJ, Murdaugh C, Parsons MA. Health Promotion in Nursing Practice. 6th ed. Upper Saddle River, NJ: Pearson/Prentice-Hall; 2010. [Google Scholar]
- 11.Rippe JM, Angelopoulos TJ, Zukley L. Lifestyle medicine strategies for risk factor reduction, prevention, and treatment of coronary heart disease: Part II. Am J Lifestyle Med. 2007;1:79–90. [Google Scholar]
- 12.Kelly BB, Fuster V. Promoting Cardiovascular Health in the Developing World: A Critical Challenge to Achieve Global Health. Washington, DC: National Academies Press; 2010. [PubMed] [Google Scholar]
- 13.Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, et al. Heart disease and stroke statistics-2012 update: A report from the American Heart Association. Circulation. 2012;125:e2–220. doi: 10.1161/CIR.0b013e31823ac046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wong N, Black H, Gardin J. Preventive Cardiology: A Practical Approach. 2nd ed. New York: McGraw Hill Professional; 2005. [Google Scholar]
- 15.Eshah NF, Bond AE, Froelicher ES. The effects of a cardiovascular disease prevention program on knowledge and adoption of a heart healthy lifestyle in Jordanian working adults. Eur J Cardiovasc Nurs. 2010;9:244–53. doi: 10.1016/j.ejcnurse.2010.02.002. [DOI] [PubMed] [Google Scholar]
- 16.Walker SN, Sechrist KR, Pender NJ. The health-promoting lifestyle profile: Development and psychometric characteristics. Nurs Res. 1987;36:76–81. [PubMed] [Google Scholar]
- 17.Zeidi IM, Hajiagha AP, Zeidi BM. Reliability and validity of persian version of the health-promoting lifestyle profile. J Mazandaran Univ Med Sci. 2012;22:103–13. [Google Scholar]
- 18.Mohamadian H, Ghannaee M, Kortdzanganeh J, Meihan L. Reliability and construct validity of the iranian version of health-promoting lifestyle profile in a female adolescent population. Int J Prev Med. 2013;4:42–9. [PMC free article] [PubMed] [Google Scholar]
- 19.Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42:1206–52. doi: 10.1161/01.HYP.0000107251.49515.c2. [DOI] [PubMed] [Google Scholar]
- 20.Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499–502. [PubMed] [Google Scholar]
- 21.Canivell S, Gomis R. Diagnosis and classification of autoimmune diabetes mellitus. Autoimmunity reviews. 2014;13(4):403–7. doi: 10.1016/j.autrev.2014.01.020. [DOI] [PubMed] [Google Scholar]
- 22.Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) JAMA. 2001;285:2486–97. doi: 10.1001/jama.285.19.2486. [DOI] [PubMed] [Google Scholar]
- 23.Lin YH, Chu LL. The health promotion lifestyle of metabolic syndrome individuals with a diet and exercise programme. Int J Nurs Pract. 2014;20:142–8. doi: 10.1111/ijn.12149. [DOI] [PubMed] [Google Scholar]
- 24.Monasta L, Batty GD, Cattaneo A, Lutje V, Ronfani L, Van Lenthe FJ, et al. Early-life determinants of overweight and obesity: A review of systematic reviews. Obes Rev. 2010;11:695–708. doi: 10.1111/j.1467-789X.2010.00735.x. [DOI] [PubMed] [Google Scholar]
- 25.Wilson PW, D’Agostino RB, Sullivan L, Parise H, Kannel WB. Overweight and obesity as determinants of cardiovascular risk: The Framingham experience. Arch Intern Med. 2002;162:1867–72. doi: 10.1001/archinte.162.16.1867. [DOI] [PubMed] [Google Scholar]
- 26.Rivera JÁ, de Cossío TG, Pedraza LS, Aburto TC, Sánchez TG, Martorell R. Childhood and adolescent overweight and obesity in Latin America: A systematic review. Lancet Diabetes Endocrinol. 2014;2:321–32. doi: 10.1016/S2213-8587(13)70173-6. [DOI] [PubMed] [Google Scholar]
- 27.Kim CJ, Park J, Kang SW. Health-promoting lifestyles and cardio-metabolic risk factors among international students in South Korea. Collegian. 2015;22:215–23. doi: 10.1016/j.colegn.2014.09.008. [DOI] [PubMed] [Google Scholar]
- 28.Bi J, Huang Y, Xiao Y, Cheng J, Li F, Wang T, et al. Association of lifestyle factors and suboptimal health status: A cross-sectional study of Chinese students. BMJ Open. 2014;4:e005156. doi: 10.1136/bmjopen-2014-005156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Chiou AF, Chen IJ, Cho SL, Wu CH. The Relationship Between Health. Promoting Behavior and Metabolic Syndrome Among Community Older Adults. Proceedings of the 23rd Internationa Nursing Research Congress, 12 September, 2012. Brisbane, Australia: 2012. [Google Scholar]
- 30.Lin CH, Chiang SL, Tzeng WC, Chiang LC. Systematic review of impact of lifestyle-modification programs on metabolic risks and patient-reported outcomes in adults with metabolic syndrome. Worldviews Evid Based Nurs. 2014;11:361–8. doi: 10.1111/wvn.12069. [DOI] [PubMed] [Google Scholar]
- 31.Sutherland LL, Simonson S, Weiler DM, Reis J, Channel A. The relationship of metabolic syndrome and health-promoting lifestyle profiles of Latinos in the Northwest. Hisp Health Care Int. 2014;12:130–7. doi: 10.1891/1540-4153.12.3.130. [DOI] [PubMed] [Google Scholar]