

Abstract
OBJECTIVES
To compare time to administration of oral antibiotics in the pediatric emergency department (ED) when antibiotics are stored in the pediatric ED versus when they were dispensed by central pharmacy services within an academic medical center.
METHODS
This was a retrospective review of patients who received a one-time dose of oral antibiotics within the pediatric ED and were subsequently discharged home. Two 3-month time periods were compared to determine the metrics of providing oral antibiotics before and after these medications were stocked in the pediatric ED automated dispensing cabinet (ADC). The primary outcome was to compare the time to administration. Secondary outcomes were to assess wastage of stocked medications and time to ED discharge.
RESULTS
In the ADC time period (n = 74), the median time to administration was 17.5 minutes versus 57 minutes in the central pharmacy time period (n = 34) (p < 0.001). The ED length of stay during the ADC time period was 188.5 minutes versus 228.5 minutes (p = 0.094). 35.4% of doses from the ADC expired resulting in a wholesale acquisition cost of $53.14 wasted.
CONCLUSION
Stocking commonly used oral antibiotics in the pediatric ED led to a significant decrease in the time to medication administration. This decreased time to administration has the potential to lead to improved patient and nursing satisfaction. Routine surveillance is needed after implementation to ensure compliance and to minimize wastage.
Keywords: antibiotics, automation, discharge, emergency medicine, medication systems, practice management
Introduction
With the 24-hour availability of emergency care, patients may not have reliable access to obtain medications at time of discharge. Many emergency department (ED) physicians will order medications to be administered prior to discharge knowing that the patient may have delays in getting prescriptions filled. In 2012, the American Academy of Pediatrics (AAP) Committee on Pediatric Emergency Medicine discussed strategies for dispensing medications at hospital discharge from the ED.1 The ED plays an important role as a safety net for children requiring emergent medical care of acute and chronic conditions.1,2 Care in the pediatric ED commonly requires treatment for acute conditions, with high priority placed on timely administration of medications.1 An important goal in emergency medicine care is rapid administration of ordered medications in order to reduce the patient's length of stay (LOS) and increase room turnover. Many EDs maintain a limited drug inventory, especially in pediatric areas where doses need to be reconstituted and given in liquid formulation. Conners and Hays3 described that storing medications within the ED allowed more reliable obtainment from automated dispensing cabinets (ADCs) rather than central hospital pharmacies and increased the use of medications stored with the ADC.
The AAP's Committee on Pediatric Emergency Medicines review discussed giving the first antibiotic dose in the ED prior to discharge.1 This strategy is also common within many institutions to ensure tolerability of the prescribed antibiotic and allow time to follow up at a community pharmacy to continue care.1 Most pediatric antibiotic doses necessitate being in a liquid formulation. However, providing around-the-clock pediatric-specific dosing within the ED can be difficult due to limited availability of pediatric pharmacy services at some institutions. In addition, dispensing a single dose can be time consuming and place a burden on pharmacy services to quickly prepare and dispense antibiotics. This may lead to administration delays, increased ED LOS, and reduced room turnover.
This study attempts to describe the practice of using ADCs to stock unit-dosed standardized syringes of common pediatric antibiotics within the ED in order to ensure timely administration of doses prior to discharge. Secondary goals were to analyze the differences in ED LOS and antibiotic use.
Materials and Methods
This was a retrospective, single-center study evaluating time to oral antibiotic administration within a pediatric ED of an academic medical center. The University of Kentucky Chandler Medical Center is an 825-bed university teaching hospital that is a designated Level I Adult/Pediatric Trauma Center and houses an 85-bed ED with 12 designated pediatric examination rooms. Due to the location and noncontinuous staffing of the decentralized pediatric pharmacy satellite, drug distribution within the pediatric ED is via central pharmacy services and ADCs (Pyxis MedStation, Cardinal Health, Pyxis Products, San Diego, CA) 24 hours per day.
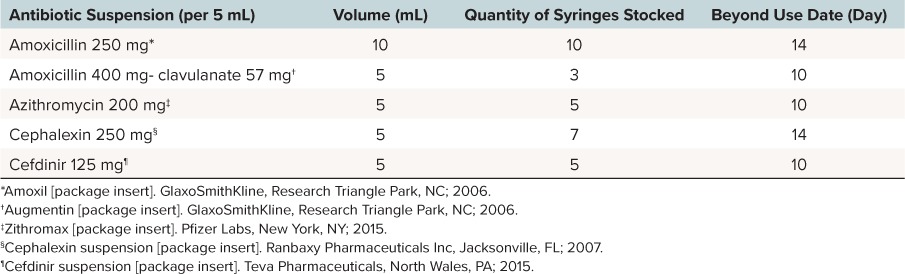
In April 2015, our institution developed a plan to address medication and ED discharge delays through stocking oral syringes of common antibiotics in ADCs in the pediatric ED. To determine the inventory of each medication, the ED pharmacist reviewed one-time orders for the orals antibiotics for the previous 90 days and decided to provide the antibiotics and quantities listed in Table 1. Within the ED, all medications are available to ED staff via override from the ADC. Therefore, time to antibiotic administration was determined by taking the difference between the time of order entry and time of administration as documented on the electronic medication administration record.
Table 1.
Oral Antibiotic Stock Syringes
Patients were identified by pharmacy charges for unit-doses of suspension formulations of amoxicillin, amoxicillin-clavulanate, azithromycin, cephalexin, and cefdinir. This included unit-doses dispensed from the ADC and patient specific doses sent from central pharmacy. The first time period included patients that were discharged from the ED when orders for these medications were dispensed from central pharmacy between September 1, 2014, and November 30, 2014. The second time period included patients that were discharged from the ED when orders for these medications were retrieved from the ADCs between August 1, 2015, and October 31, 2015. There was a washout period of 3 months after the April implementation in order to allow staff to become accustomed to the change in practice.
Institutional review board approval was obtained and consent was waived. All children who were at least 30-days-old and ≤ 18 years old and who received only 1 dose of oral antibiotic prior to discharge from the ED were included for analysis. Patients who were admitted to the children's hospital and those patients who had orders for oral suspension but were administered another dosage form were excluded from analysis.
The primary outcome was time to oral antibiotic administration before and after the implementation of oral unit-dose syringes within the ADCs. Secondary outcomes included ED LOS, number of expired doses, and the institution cost of expired medication. Data collection also included the following: chief complaint, discharge diagnosis, time of ED admission and discharge, antibiotic selected and dose, patient age and weight, time of order entry, and time of administration. In order to assess utilization and potential product waste, data from the ADCs included the following: number of doses stocked and number of units wasted due to expiration. Data on amount of drug wasted at the time of administration were not captured as part of this investigation. Descriptive statistics were employed to characterize the population and ADC use. Mann-Whitney U testing was used to compare the primary and secondary outcomes. A p value < 0.05 was considered statistically significant. All statistical analyses were conducted using IBM SPSS Statistics Version 23 (IBM Corporation, Armonk, NY).
Results
A total of 108 patients were identified as meeting inclusion criteria with 34 patients included in the preintervention group and 74 patients in the postintervention group. Patient characteristics are listed in Table 2. The only statistical difference was in the antibiotics prescribed. With regards to the primary outcome, when oral antibiotics were stocked in the ADC, the median time to administration was 17.5 minutes versus 57 minutes when doses were dispensed from central pharmacy (p < 0.001). There was a median reduction in ED LOS by 40 minutes, which was not statistically significant (p = 0.094) (Table 3).
Table 2.
Patient Characteristics
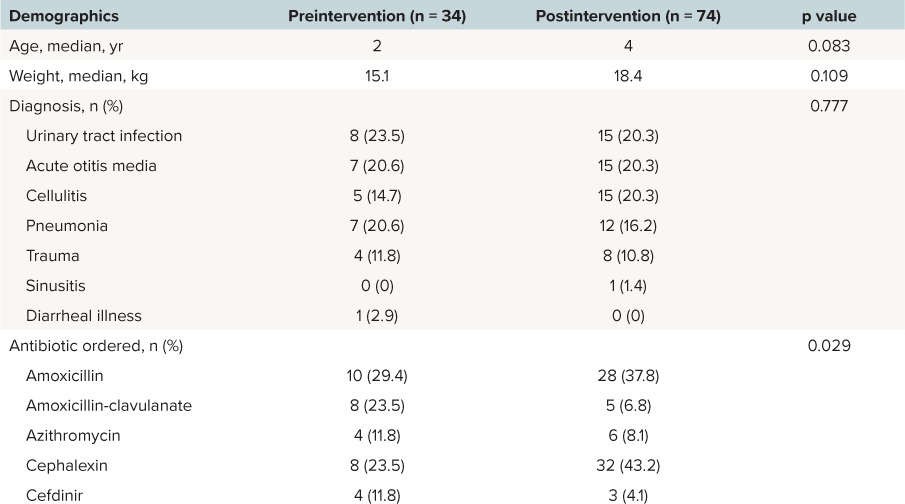
Table 3.
Median Time to Antibiotic Administration and Emergency Department Length of Stay

During the postintervention period, medication wastage declined as staff became accustomed to obtaining medications from the ADC. The percent of doses wasted from the ADC over the postintervention period was 40.6%, 50.3%, and 15.3% for August, September, and October, respectively. From the institution's perspective, the total cost of medications wasted was $53.14 (wholesale acquisition cost). Amoxicillin and cephalexin were wasted the least often with only 13 of 144 doses expiring.
Discussion
After addition of the 5 oral antibiotic suspensions to the ADC, a significant decrease in the time to administration and nonsignificant decrease in the ED LOS were noted. Despite a 3-month washout period, there were a high percentage of doses that expired in the ADC the first 2 months of the study period; however, this translated to a low overall cost to the institution. Both staff reeducation and par level adjustments have since been completed to further reduce waste.
Placing medications in ADCs has previously been shown to decrease the time to medication administration in the ED.4–6 To our knowledge, this is the first study to use the practice of stocking unit doses for commonly prescribed pediatric oral antibiotic suspensions. Since evaluating the results, pharmacy technicians now routinely check stock to ensure all products that expired are removed and refilled in a timely manner.
We were unable to directly measure patient and nursing satisfaction through this evaluation. It was recently shown that adding medications may increase the time to retrieval; however, the nursing staff believed that ADCs saved time in their workflow.7 Additionally, a decrease in the time to administration of the first dose of medication of nearly 40 minutes can lead to improvements in both these areas. Poor patient satisfaction is more likely to occur if ED LOS times are longer than what is perceived to be appropriate.8 Therefore, if the perceived time to obtain antibiotics is reduced, this can improve overall satisfaction for the patients and families.
The change in ED LOS during the study period was not statistically significant; however, a time savings of 40 minutes could potentially lead to substantial impacts on throughput including: quicker patient turnover throughout a shift, reduced times to be seen by a provider, and reduction in lobby wait times. The overall costs to the institution were determined to be minimal. In follow up discussions with central pharmacy leadership, the change has not negatively impacted the pharmacy workflow.
This intervention required a multidisciplinary teaching approach to ensure appropriate utilization and to minimize the risk for errors. First, doses are not patient-specific and must be transferred by nursing staff to another measuring device. Many nurses within the ED are comfortable with this practice, as many other medication doses from ADCs need to be promptly manipulated to make the patient-specific dose. Also, due to the potential for selecting a look-a-like sound-a-like product, appropriate space is needed within an ADC to ensure that the correct medication is consistently retrieved. Our strategy was to install multiple shelves in our refrigerated ADC and place each product on a different shelf.
This study is limited by its retrospective nature. Attempts were made to only include orders during the designated time period to narrow focus on dispensing practices rather than practice variations. There is an ED pharmacist present who provides clinical support to adult and pediatric patients 7 days per week. Between the 2 time periods, the hours of ED pharmacy support expanded from 10 hours to 16 hours per day. However, this change was predicted to have minimal impact on study outcomes as the scope of ED pharmacy services does not include dispensing oral suspensions. Given the retrospective nature of this evaluation, ED patient volumes could not be controlled, which could explain the difference in sample size during each time period and the significant difference in antibiotics prescribed. The increased volume after the intervention may also be secondary to an increased knowledge and utilization of readily available product by the medical staff. Attending and resident physicians, physician assistants, and nurses were notified of the practice change via email and encouraged continuation of predischarge doses of antibiotics.
Stocking commonly prescribed oral antibiotics within the ED ADC leads to a decreased time to administration of the first dose. The process must be routinely followed to ensure appropriate medications are stocked and to minimize wastage of product and resources. This practice could lead to improvements in patient and nursing satisfaction and possibly ED LOS.9,10 Further investigation is necessary to sufficiently determine if this process can directly impact other outcomes as described above.
Acknowledgments
Presented in part at the annual meeting of the Pediatric Pharmacy Advocacy Group, April 2016, Atlanta, Georgia.
Abbreviations
- AAP
American Academy of Pediatrics
- ADC
automated dispensing cabinet
- ED
emergency department
- LOS
length of stay
Footnotes
Disclosure The authors declare no conflicts or financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employment, gifts, and honoraria. All authors had full access to the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Copyright Published by the Pediatric Pharmacy Advocacy Group. All rights reserved. For permissions, email: matthew.helms@ppag.org.
REFERENCES
- 1. Yamamoto LG, Manzi S, Committee On Pediatric Emergency Medicine, . et al. Dispensing medications at the hospital upon discharge from an emergency department. Pediatrics. 2012; 129 2: e562. [DOI] [PubMed] [Google Scholar]
- 2. American Academy of Pediatrics Committee on Pediatric Emergency Medicine, Yamamoto LG.. Access to optimal emergency care for children. Pediatrics. 2007; 119 1: 161– 164. [DOI] [PubMed] [Google Scholar]
- 3. Conners GP, Hays DP.. Emergency department drug orders: does drug storage location make a difference? Ann Emerg Med. 2007; 50 4: 414– 418. [DOI] [PubMed] [Google Scholar]
- 4. Ward MJ, Boyd JS, Harger NJ, . et al. An automated dispensing system for improving medication timing in the emergency department. World J Emerg Med. 2012; 3 2: 102– 107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Hitti EA, Lewin JJ 3rd, Lopez J, . et al. Improving door-to-antibiotic time in severely septic emergency department patients. J Emerg Med. 2012; 42 4: 462– 469. [DOI] [PubMed] [Google Scholar]
- 6. Lo A, Zhu JN, Richman M, . et al. Effect of adding piperacillin-tazobactam to automated dispensing cabinets on promptness of first-dose antibiotics in hospitalized patients. Am J Health Syst Pharm. 2014; 71 19: 1663– 1667. [DOI] [PubMed] [Google Scholar]
- 7. Roman C, Poole S, Walker C, . et al. A ‘time and motion’ evaluation of automated dispensing machines in the emergency department. Australas Emerg Nurs J. 2016; 19 2: 112– 117. [DOI] [PubMed] [Google Scholar]
- 8. Boudreaux ED, O'Hea EL.. Patient satisfaction in the emergency department: a review of the literature and implications for practice. J Emerg Med. 2004; 26 1: 13– 26. [DOI] [PubMed] [Google Scholar]
- 9. Fanning L, Jones N, Manias E.. Impact of automated dispensing cabinets on medication selection and preparation error rates in an emergency department: a prospective and direct observational before-and-after study. J Eval Clin Pract. 2016; 22 2: 156– 163. [DOI] [PubMed] [Google Scholar]
- 10. Ostrowsky B, Sharma S, DeFino M, . et al. Antimicrobial stewardship and automated pharmacy technology improve antibiotic appropriateness for community-acquired pneumonia. Infect Control Hosp Epidemiol. 2013; 34 6: 566– 572. [DOI] [PubMed] [Google Scholar]