

Abstract
Background
The objective of this evaluation is to understand the human health impacts of mountaintop removal (MTR) mining, the major method of coal mining in and around Central Appalachia. MTR mining impacts the air, water, and soil and raises concerns about potential adverse health effects in neighboring communities;exposures associated with MTR mining include particulate matter (PM), polycyclic aromatic hydrocarbons (PAHs), metals, hydrogen sulfide, and other recognized harmful substances.
Methods
A systematic review was conducted of published studies of MTR mining and community health, occupational studies of MTR mining, and any available animal and in vitro experimental studies investigating the effects of exposures to MTR-mining-related chemical mixtures. Six databases (Embase, PsycINFO, PubMed, Scopus, Toxline, and Web of Science) were searched with customized terms, and no restrictions on publication year or language, through October 27, 2016. The eligibility criteria included all human population studies and animal models of human health, direct and indirect measures of MTR-mining exposure, any health-related effect or change in physiological response, and any study design type. Risk of bias was assessed for observational and experimental studies using an approach developed by the National Toxicology Program (NTP) Office of Health Assessment and Translation (OHAT). To provide context for these health effects, a summary of the exposure literature is included that focuses on describing findings for outdoor air, indoor air, and drinking water.
Results
From a literature search capturing 3088 studies, 33 human studies (29 community, four occupational), four experimental studies (two in rat, one in vitro and in mice, one in C. elegans), and 58 MTR mining exposure studies were identified. A number of health findings were reported in observational human studies, including cardiopulmonary effects, mortality, and birth defects. However, concerns for risk of bias were identified, especially with respect to exposure characterization, accounting for confounding variables (such as socioeconomic status), and methods used to assess health outcomes. Typically, exposure was assessed by proximity of residence or hospital to coal mining or production level at the county level. In addition, assessing the consistency of findings was challenging because separate publications likely included overlapping case and comparison groups. For example, 11 studies of mortality were conducted with most reporting higher rates associated with coal mining, but many of these relied on the same national datasets and were unable to consider individual-level contributors to mortality such as poor socioeconomic status or smoking. Two studies of adult rats reported impaired microvascular and cardiac mitochondrial function after intratracheal exposure to PM from MTR-mining sites. Exposures associated with MTR mining included reports of PM levels that sometimes exceeded Environmental Protection Agency (EPA) standards; higher levels of dust, trace metals, hydrogen sulfide gas; and a report of increased public drinking water violations.
Discussion
This systematic review could not reach conclusions on community health effects of MTR mining because of the strong potential for bias in the current body of human literature. Improved characterization of exposures by future community health studies and further study of the effects of MTR mining chemical mixtures in experimental models will be critical to determining health risks of MTR mining to communities. Without such work, uncertainty will remain regarding the impact of these practices on the health of the people who breathe the air and drink the water affected by MTR mining.
Keywords: mountaintop removal mining, coal mining, Appalachia, surface mining, community health, systematic review, exposure, risk of bias, risk
Introduction
Since its introduction in the 1960s, mountaintop removal (MTR) mining has become a major method of coal mining in and around Central Appalachia (including parts of Kentucky, Ohio, Pennsylvania, Tennessee, Virginia, and West Virginia) because it is typically faster, cheaper, and less labor intensive than underground mining (Holzman 2011). This mining method involves clearing the area of trees and topsoil and using explosives to blast apart the mountain rock to access coal seams (Palmer et al. 2010). The excess rock (i.e., mine spoil) is often pushed into adjacent valleys (i.e., valley fill). The air, water, and soil in the surrounding area are impacted by these mining practices and contamination due to MTR mining has the potential to adversely impact human health in the surrounding community (Acton et al. 2011; Palmer et al. 2010; Simmons et al. 2008). Exposures associated with MTR mining include PM, PAHs, metals, and other potentially harmful substances (Palmer et al. 2010).
The overall objective of this evaluation is to understand the human health impacts of MTR mining by conducting a systematic review of published studies of MTR mining and community health, occupational studies of MTR mining, and any available animal and in vitro experimental studies investigating the effects of exposures to MTR-mining-related chemical mixtures. The Population, Exposure, Comparator, and Outcome (PECO) Statement includes all human population studies and animal models of human health, direct and indirect measures of MTR-mining exposure, studies which provided vehicle-only controls in experimental studies, any health-related effect or change in physiological response, and any study design type. To provide context for these health effects by characterizing components of these MTR-mining-related mixtures, a summary of the exposure literature is included as well. This analysis will identify important areas of future research needs and provide recommendations to strengthen the design and conduct of future studies assessing the health effects of MTR mining.
Methods
The detailed protocol for conducting this systematic review was drafted in consultation with experts in the field, registered in PROSPERO (an international prospective register of systematic reviews, registration number PROSPERO 2016:CRD42016037192 , http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42016037192), and posted publicly on the NTP website (http://ntp.niehs.nih.gov/go/780611) on April 3, 2016 (Boyles et al. 2016). A revised protocol with updated exclusion criteria was posted on July 27, 2016 prior to initiating data extraction. The protocol includes: review aims, problem formulation, literature search strategy, detailed inclusion/exclusion criteria, data extraction process, individual study quality assessment method (i.e., risk of bias), and strategy for evidence synthesis and reaching hazard conclusions.
The literature search strategy included 6 databases (Embase, PsycINFO, PubMed, Scopus, Toxline, and Web of Science) with customized terms and no restrictions on publication year or language (see Appendix 1 of protocol). This review includes all references identified through October 27, 2016. Hand searching for additional relevant references was conducted of the reference lists of relevant reviews and commentaries identified during the initial search and the reference lists of studies included after the full text review. A Request for Information on “Mountaintop removal mining (health impacts on surrounding communities)” including published, ongoing, or planned studies related to evaluating adverse health outcomes was published in the Federal Register on October 7, 2015 (https://ntp.niehs.nih.gov/ntp/pressctr/frn/2015/80frn194ntp20151007_htm.pdf) to try to identify additional references.
Title/abstract and full text screening was conducted by independent screeners (RBB, SBG, and SM) with two screeners per article. Conflicts were resolved by the lead scientist (ALB). Detailed inclusion/exclusion criteria are provided in Table 1.
Table 1.
Detailed PECO study eligibility criteria.
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Participants/Population (human studies or experimental model systems) | |
|
|
| Exposure | |
|
|
| Comparators | |
|
|
| Outcomes | |
|
|
| Publications (e.g., language restrictions, use of conference abstracts) | |
|
|
These criteria reflect the protocol revision to excluded studies that were not directly relevant to the research question: studies with unspecified type of mining conducted prior to widespread use of MTR mining or in geographic areas without MTR mining; exposure to coal samples, dust or leachates in vitro; descriptive case series of miners without a comparator group; and conference abstracts. Lists of all included and excluded studies (including stage of review when excluded and reason for exclusion) were posted to the NTP project website on September 7, 2016 (updated November 16, 2016).
Data extraction was conducted with structured forms and stored in a database format using Health Assessment Workspace Collaborative (HAWC, https://hawcproject.org), an open source, web-based interface (extracted by SBG and SM, reviewed for quality by RBB). The protocol lists all of the data extraction elements (Appendix 2 Human, Appendix 3 Animal, Appendix 4 In vitro), and all study data are publicly available in the Mountaintop Removal Mining (2016) assessment (https://hawcproject.org/assessment/288/). Individual study quality was assessed at the study level with the risk of bias tool developed by OHAT using a parallel approach to evaluate risk of bias in human and non-human animal studies (also available in HAWC, tool available at: https://ntp.niehs.nih.gov/pubhealth/hat/noms/index-2.html). Commentaries or letters on specific studies were also reviewed to see if they contain content that should be noted during data extraction or risk of bias assessment of the original report. All studies were assessed by two independent reviewers (RBB and SBG) prior to determining a consensus risk of bias rating. The evaluation criteria were developed a priori and detailed in the protocol utilizing 7 questions applicable to observational human studies and 9 questions for experimental animal studies. Each question was rated as one of 4 categories for each study: definitely high risk of bias, probably high risk of bias/not reported, probably low risk of bias, and definitely low risk of bias. If risk of bias criteria were not reported, authors were contacted to provide the missing information and all authors responded. There is no overall quality judgment or summation across elements of risk of bias, consistent with Cochrane review practice (Higgins et al. 2011).
Studies that measure and characterize the heterogeneous mixture of chemicals and particulate matter in air, water, or soil that are attributable to MTR mining are critical to the assessment of potential human health effects, yet do not strictly meet the PECO criteria. A comprehensive assessment of potential health effects of individual components of the exposure mixture (e.g., chemical composition of particulate matter and cardiopulmonary effects) associated with MTR mining is beyond the scope of this review.
Results and Discussion
The literature search retrieved 4,356 references, 3,088 after the removal of duplicates across databases (updated through October 27, 2016). No additional studies were identified through hand searching the reference lists of relevant reviews, commentaries, or included studies or in response to the Request for Information. Figure 1 details how title/abstract and full text screening identified: 33 human studies, (29 community, four occupational surface mining), four experimental studies (two in rats, one in human bronchial cell line and mice, and one in C. elegans), and 58 studies of MTR-mining exposures (nine with the potential for direct human exposure by air or drinking water, and 49 of other environmental exposures).
Figure 1.

Study screening diagram (through October 27, 2016)
* 29 community, 4 occupational surfacing mining
** 2 rat, 1 in vitro and mice, 1 C. elegans
*** 9 air or drinking water, 49 other environmental studies
Observational studies
The 29 community-based studies included endpoints across a wide range of health outcome categories (see Table 2). Findings of individual studies summarized in Supplemental Tables include cardiopulmonary effects (n=7, Supplemental Table 1A), cancer (n=5, Supplemental Table 1B), reproductive effects (n=3, Supplemental Table 1C), mortality (n=11, Supplemental Table 1D), general health status (n=5, Supplemental Table 1E), and other effects (n=7, Supplemental Table 1F).
Table 2.
Overview of 29 community health studies
| Outcomes | Populations | Exposures | Findings | Publications | Risk of Bias Rating* |
|---|---|---|---|---|---|
| Cardiopulmonary: diagnoses, hospitalizations, and symptoms | 1 national study; 2 regional studies in WV, KY, PA, and IN; 3 in WV; 1 in KY, 1 in VA; (2000–2014) | Coal production by county; MTR mining (present or absent); Appalachia or non- Appalachia area ; residence within 3 miles of active surface mine | Associated with adverse cardiopulmonary outcomes in most studies | 8 studies (Brink et al. 2014; Hendryx et al. 2007; Hendryx and Ahern 2008; Hendryx and Zullig 2009; Hendryx 2013; Hendryx and Entwhistle 2015; Hendryx and Luo 2015; Talbott et al. 2015) |
|
| Cancer: hospitalization, self-reported, lung | 1 regional study in WV, KY, and PA; 2 in KY; 2 in WV; (1995–2012) | Coal production by county; MTR mining (present or absent) | Not associated with cancer in most studies | 5 studies (Christian et al. 2011; Hendryx et al. 2007; Hendryx and Ahern 2008; Hendryx et al. 2012b; Hendryx 2013) |
|
| Reproductive: birth defects and low birth weight | 1 regional study in WV, VA, TN, and KY; 2 in WV; (1996–2009) | Coal production by county; MTR mining (present or absent) | Associated with low birth weight and some birth defects, but not associated with birth defects after adjusting for hospital of birth | 3 studies (M Ahern et al. 2011; MM Ahern et al. 2011; Lamm et al. 2015) |
|
| Mortality: all-cause and specific causes | 3 national studies; 5 regional studies in Appalachia, WV, VA, TN, KY, and NC; 2 in WV; 1 in KY; (1950–2014) | Coal production by county, per capita, by type, by GIS distance; MTR mining (present or absent) Appalachia or non- Appalachia area | Associated with mortality in most studies (varying by type). Mortality was also associated with Appalachia and poverty in general. | 11 studies (Borak et al. 2012; Buchanich et al. 2014; Esch and Hendryx 2011; Hendryx et al. 2008; Hendryx 2009; Hendryx and Ahern 2009; Hendryx et al. 2010; Hendryx 2013; Hendryx and Holland 2016; Hitt and Hendryx 2010; Woolley et al. |
|
| General Health Status: self-reported scales and serious illness | 1 national study; 2 regional studies in WV, TN, NC, KY, and VA; 1 in WV; 1 in KY; (2000–2012) | Coal production by county; MTR mining (present or absent); Appalachia or non- Appalachia area; number of mining facilities near residence | Associated with poorer health status in most studies | 5 studies (Hendryx and Ahern 2008; Hendryx 2013; Woolley et al. 2015b; Zullig and Hendryx 2010, 2011) |
|
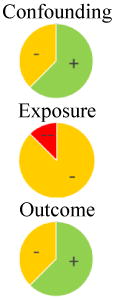
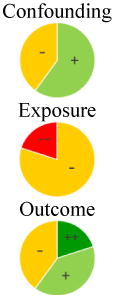
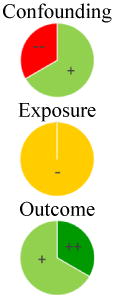
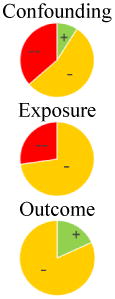
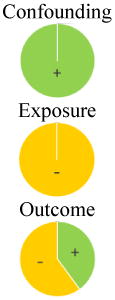
Risk of bias for 3 key questions: 1) Did the study design or analysis account for important confounding and modifying variables?, 2) Can we be confident in the exposure characterization?, and 3) Can we be confident in the outcome assessment? Pie charts depict the percent of studies that were rated as (++, dark green) definitely low risk of bias, (+, light green) probably low risk of bias, (-, yellow) probably high risk of bias, or (--, red) definitely high risk of bias.
While most studies reported some significant associations of health endpoints with mining activity, the results were inconsistent and few studies reported the same endpoint and exposure. Only one study measured indoor and outdoor particle counts and found elevated levels of high-sensitivity C-reactive protein (HsCRP) and cardiopulmonary conditions in residents near active surface coal mining operations (Hendryx and Entwhistle 2015). All other studies determined exposure to mining by proximity of residence or hospital to coal mining or production level. These studies likely included case and comparison groups that overlap across studies. Eleven studies of mortality were conducted with most reporting higher rates associated with coal mining, but many of these relied on the same national datasets and were unable to consider individual-level contributors to mortality such as poor socioeconomic status or smoking. Birth defects represent an outcome with a significantly shorter relevant exposure window than mortality, and results from two studies of birth defects (MM Ahern et al. 2011; Lamm et al. 2015) are shown in Figure 2. While Ahern et al. found significant associations with MTR mining for most types of birth defects (2011), Lamm et al. identified a potential reporting difference by hospital that may explain the underlying differences in rates of birth defects by region (2015).
Figure 2.

Selected prevalence ratios for birth defects from MTR-mining studies.
Additional graphs of results across studies are available for other outcome areas where comparable statistics were available (see Visualizations in HAWC (https://hawcproject.org/summary/assessment/288/visuals/). All extracted study information and risk of bias assessments can be viewed in HAWC or downloaded (https://hawcproject.org/assessment/288/downloads/).
Occupational exposure was the sole focus of four studies, while two other studies considered health effects self-reported by former coal workers (Supplemental Table 2). Studies of surface coal workers reported increased silicosis, pneumoconiosis, disability from occupational injuries and comorbidities, and decreased pulmonary function, but no increases in self-reported cancer or poor health (CDC 2000, 2012; Hendryx et al. 2012b; Prince and Frank 1996; Woolley et al. 2015b; Young and Rachal 1996).
Within the last 20 years, MTR mining has spread to impact a larger portion of Appalachia and all the community health studies identified were published in the last 10 years (2007–2016). Many of these studies have been conducted in overlapping regions, time frames, and with similar comparison groups (usually non-mining regions of Appalachia) –essentially including many of the same communities and cases. In one instance, Borak et al. (2012) re-analyzed mortality data used in 3 other papers (Hendryx et al. 2008; Hendryx 2009; Hendryx and Ahern 2009), however the original authors disputed how well the re-analysis matched their original geographic area and timeframe (Hendryx and Ahern 2012). Lamm et al. (2015) proposed an additional factor, hospital of birth, that could have biased outcome reporting in a previous study of birth defects and included a re-analysis of that study (MM Ahern et al. 2011). They concluded that there was no increased risk if this factor was considered. For these non-independent and inconsistent results, risk of bias analysis assessment offers a systematic consideration of the study design and conduct limitations of the studies.
Risk of bias assessment of observational studies
For the observational studies (community and occupational), seven risk of bias questions were applicable. Three of these questions were considered most critical to environmental health assessments. These were: 1) Did the study design or analysis account for important confounding and modifying variables?, 2) Can we be confident in the exposure characterization?, and 3) Can we be confident in the outcome assessment? In each outcome area, the pie charts in Table 2 show the ratings for these three questions. None of the studies were rated as low risk of bias for exposure characterization, reflecting the use of indirect measures of exposure that were inconsistently matched to the timeframe for the outcome assessment (see Supplemental Figure 1 for percent ratings across all questions). While there is evidence of exposures in air and water associated with MTR mining in separate publications (see Exposures from MTR-mining section), the data could not be incorporated into analyses of health effects, thus the available human health studies were limited by the exposure assessment methods. Lack of accounting for confounding and potential modifying variables were rated as high risk of bias for 59% of studies, particularly when these variables could not be considered because individual participants were not enrolled in the studies, such as for mortality data. A lack of blinding for self-reported outcomes, including types of symptoms and general health status, was of concern as residents likely know if they live near active mining operations and have prior opinions on its effect on their health. Risk of bias ratings for individual studies and additional visual displays are available in HAWC.
The results across MTR-mining studies indicate a potential influence of funding source on the authors’ interpretation or results and conclusions. Funding source is a potential bias that should be considered (Bero 2013), although it was not part of the risk of bias assessment for this systematic review. Sixteen studies did not report a funding source, five reported funding independent of the mining industry, and seven studies reported funding from the energy sector with a statement that the funders had no role in the study design, conduct, or publication. The only papers to report no adverse effects of coal mining had energy sector funding. Publication bias could explain this observation –negative results are often unpublished –and several of the negative studies were designed to be similar to previously published significant findings (Borak et al. 2012; Lamm et al. 2015).
This review’s risk of bias assessment found that all the human studies had critical flaws. Future studies are unlikely to resolve these conflicting results unless they improve exposure characterization, account for confounding variables, and use blinded, validated outcome assessment methods.
Experimental studies
The literature search and screen identified four experimental studies of MTR-mining mixtures: three rodent studies of exposure to PM collected from active MTR-mining sites and one worm study of water and sediment collected from MTR-mining-impacted streams (see Supplemental Table 3). Two studies of adult rats reported impaired microvascular function and impacts on cardiac mitochondrial function after intratracheal exposure to the same mixture of PM collected in the vicinity of MTR-mining sites (Knuckles et al. 2013; Nichols et al. 2015). Cytotoxicity and impaired cell proliferation and migration were reported in a human bronchial cell line exposed to MTR-mining PM, and transplantation of these cells into mice promoted tumor growth of co-transplanted human lung carcinoma H460 cells (Luanpitpong et al. 2014). Several strains of C. elegans had impaired growth after exposure to water and sediment collected from MTR-mining impacted streams (Turner et al. 2013).
Risk of bias assessment of these experimental studies found the rodent studies to have generally strong design and conduct (see Supplemental Figure 2). Failure to blind study personnel to treatment group at allocation and during the study resulted in definitely high risk of bias ratings for some questions, while the outcome assessment methods used were considered acceptable and most studies blinded or used non-subjective outcome assessment methods (see detailed justifications in HAWC). Blinding during the conduct of an experimental animal study is uncommon in the field, but has the potential to bias the results (Macleod et al. 2015).
Experimental evidence of biological effects of MTR-mining PM and water quality support the plausibility of the observed effects in people living near these sites, but definitive conclusions could not be reached due to the small number of studies and diverse endpoints evaluated.
Exposures from MTR-mining
During our literature search, we identified several studies that measured mining associated contaminants in air and water near MTR mining activities that could directly impact people in the community or indirectly impact them by effects on the ecology of the area. Nine studies, dated 1991–2015, examined air and/or drinking water contamination near surface-mining activities in Virginia, West Virginia, and Kentucky. Details of these studies are presented in Table 3. Three of these studies compared mining sites with reference/control sites to determine if there was significantly more contamination due to MTR-mining activities (Hendryx et al. 2012a; Kurth et al. 2015; Kurth et al. 2014). One study monitored water quality before and during a blasting event to determine if mining introduced contaminants (OSMRE 2002). These four studies found significant effects of mining activities. Five other studies measured contamination at MTR-mining sites of air and/or water, but not in relation to control sites (Aneja et al. 2012; Aneja et al. 2016; Ettinger and McClure 1983; Piacitelli et al. 1990; Simonton 2014).
Table 3.
Summary of community health relevant studies of MTR-mining exposure
| Citation | Sampling Details | Site Characterization | Contaminant Levels | Results |
|---|---|---|---|---|
| Aneja (2012) | Virginia Aug 2008 AIR:
|
EXPOSURE: road near residential area where heavy truck traffic from coal surface mining facilities was reported (2 sites) No control |
Maximum level PM10: 469.7 μg/m3 |
PM10 samples exceeded EPA standard (150 μg/m3) in most of the samples from one site and half the samples from the other site Metals found in the samples included antimony, arsenic, beryllium, cadmium, chromium, cobalt, lead, manganese, mercury, nickel, and selenium |
| Aneja (2016) | Virginia 2012 AIR:
|
EXPOSURE: at Campbell, near coal mines and, at Willis, close to a haul road No control |
24-hour averages CAMPBELL SITE PM10: 250.2 ± 135.0 μg/m3 WILLIS SITE PM10: 138.4 ± 62.9 μg/m3 |
PM10 samples exceeded EPA standard (150 μg/m3) Predicted PM2.5 exceeded the World Health Organization 24 hour PM2.5 standard on some days, according to the multi-variate model |
| Ettinger and McClure (1983) | West Virginia Sep 1979 AIR:
|
EXPOSURE 1: drilling, overburden removal and coal loading EXPOSURE 2: regrading of land EXPOSURE 3: truck hauling of overburden and coal No control |
Emission rates EXPOSURE 1 381.6 kg/20 hr EXPOSURE 2 496.8 kg/20 hr EXPOSURE 3 0.2 g/sec m |
More fugitive dust produced by surface mining in Appalachian coal fields compared with similar activity in the western United States |
| Hendryx (2012a) | West Virginia 2001–2009 DRINKING WATER: Public drinking water violations |
EXPOSURE 1: counties with MTR mining (161 facilities) EXPOSURE 2: counties with coal mining other than MTR mining (184 facilities) CONTROL: counties with no coal mining (137 facilities) |
Not provided |
*Increased numbers of violations in counties with MTR mining facilities (73% of overall violations) compared to those with other coal mining and control counties Failure to conduct required sampling for organic compounds accounts for 85% of the violations in the counties with MTR mining |
| Kurth (2014) | West Virginia Jun 2011-May 2012 AIR:
|
EXPOSURE: valleys surrounded by mountains where active MTR mining and other coal- mining activities (rail and truck transportation, underground mines, and coal processing facilities) were prominent (2 sites) CONTROL: no mining activity, in area where ~60% of the land is federal or state owned (1 site) |
Maximum levels
EXPOSURE SITES: † TSP: 27.7 μg/m3 PM10: 10.6 μg/m3 PM2.5: 5.2 μg/m3 CONTROL SITES: TSP: 16 μg/m3 PM10: 6.8 μg/m3 PM2.5: 5.4 μg/m3 |
*Increased particle number concentrations and calculated deposited lung dose in mining areas compared with control *Increased PM10 mass concentration at the MTR mining sites for the overall sampling period and during June and July *Increased PM2.5 mass concentration at the MTR mining site during July |
| Kurth (2015) | West Virginia Jun 2011-Dec 2012 AIR:
|
EXPOSURE: majority of coal mined by MTR mining, but allows for contribution from contour and other methods (6 sites) “INTERNAL” CONTROL: predominantly underground mining (2 sites) “EXTERNAL” CONTROL: no mining activity within 160 km, in areas where ~60% of land is federal or state owned (2 sites) |
Not provided |
Decreased sampled PM in August 2011 (period of mining inactivity) in surface mining sites normalized to an internal control compared to sampled PM in June 2011 (a period of mining activity) in surface mining sites normalized to an external control Pronounced enrichment of crustal-derived elements present in PM samples in June 2011 (a period of mining activity) compared to external control (up to 10x) Increased low-molecular-weight alkylated compounds (including PAHs) in surface mining sites compared to internal and external controls *Increased primary aluminosilicate PM at surface mining sites compared to secondary PM at internal and external controls |
| OSMRE (2002) | Virginia, West Virginia, Kentucky Nov 2000-Dec 2001 WELL DRINKING WATER:
|
EXPOSURE: drinking water wells in proximity to surface mining sites (5 sites) No control |
Maximum levels TDS: 1740 mg/L TSS: 103 mg/L Sulfate: 991 mg/L Iron: 67.0 mg/L Manganese: 3.86 mg/L Aluminum: 0.07 mg/L |
*Differences in iron and TSS concentrations measured prior to and after blasting events in many monitoring wells Slight water quality changes were observed over time but were unrelated to blasting events |
| Piacitelli (1990) | Surface coal mines in the United States 1982–1986 AIR:
|
EXPOSURE: strip mining and preparation facilities by job category No control |
Not provided |
Average concentrations of Respirable coal mine dust usually below PELs; at least 10% of samples from preparation and most drilling areas exceeded PEL Very high proportion of respirable quartz silica samples in driller areas exceeded quartz PEL; highwall drill operators and helpers mostly exposed above PEL |
| Simonton (2014) | West Virginia 2006–2011 INDOOR AIR:
|
EXPOSURE: communities in Appalachia adjacent to mining operations (3 sites)††
No control |
Maximum levels
DRINKING WATER: Sulfate: 372 mg/L Sulfide: 5.5 ppm INDOOR AIR: H2S: 21 ppm |
H2S released into indoor air during domestic water use from sulfide which contaminates drinking water aquifers H2S in homes exceeded health safety standards |
PM = particulate matter; PAH = polycyclic aromatic hydrocarbon; TSP = total suspended particles; H2S = hydrogen sulfide; TDS = total dissolved solids; TSS = total suspended solids.
statistically significant result
Values provided by author communication
3 sites represent 3 communities; exact number of sampling sites in those 3 communities is unclear
Impact on air quality
Air quality impacts of mountain top mining are not monitored at the federal and state level due to the presence of very few air quality monitors in the rural areas (Hendryx 2013; Kurth et al. 2014; Pope and Wu 2014). As a result, it is difficult to study acute health effects of rural populations due to acute exposure to air pollution from MTR mining activities in these areas. The studies of ambient air quality or those measuring particulate matter in and around MTR mining sites that we identified are discussed below.
Particulate matter (PM) was measured in residential areas near surface mining sites in West Virginia and compared to nearby sites with no mining-related activity as well as “internal controls” with non-MTR mining (Kurth et al. 2015; Kurth et al. 2014). Coal mining activities at these sites included related activities, such as rail and truck transportation, underground mines, and coal processing facilities. To estimate potential human exposure to PM, respiratory deposition was calculated as well (Kurth et al. 2014). The authors found that particle number concentrations and model-predicted deposited lung dose were significantly greater around mining areas compared with the non-mining area and variations in PM size related to the time of year (e.g., PM10 peaked during June and July, but PM2.5 mass concentration peaked only during July) (Kurth et al. 2014). The presence of trace metals was also determined. During a period of active mining (June 2011), there was pronounced enrichment in crustal-derived elements at the MTR-mining sites (some at more than ten times the concentration of the external control sites) that was not present during a period of MTR mining inactivity (August 2011) (Kurth et al. 2015). Alkylated compounds of low molecular weight, including low-molecular-weight PAHs, consistent with coal dust were also found at MTR-mining sites (Kurth et al. 2015).
In another study (Aneja et al. 2012), PM10 air testing of residential sites near areas of mining activity in Virginia found ten of twelve samples from one location and half the samples from another location exceeded the PM10 EPA standard of 150 μg/m3, but this study did not compare MTR-mining sites with control sites or baseline data (Aneja et al. 2012). Compared to the U.S. national ambient air quality standard, Aneja et al. (2016) reported higher 24-hour average PM10 concentrations near coal mines and close to a mining haul road. Another study found that miners could potentially be exposed to dust/quartz levels above acceptable permissible exposure limits (PELs): drilling job area dust concentrations were above the 2 mg/m3 limit and over ¾ of samples from highwall drill operators exceeded the 0.1 mg/m3 quartz exposure limit (Piacitelli et al. 1990). Fugitive dust emissions at a contour surface coal mine in southern West Virginia were higher for several varied mining activities compared with a similar study in the western United States (Ettinger and McClure 1983).
Impact on drinking water
Sulfide and sulfate in tap water and hydrogen sulfide gas (H2S) in indoor air were measured inside residences in three communities near mining activity in West Virginia (Simonton 2014). An odor consistent with H2S was observed when running the tap or shower in several homes and H2S measurements in these homes exceeded health safety standards. The author concluded that sulfide-contaminated drinking water from aquifers in MTR-mining communities is released into indoor air as H2S during domestic water use (Simonton 2014).
Other aspects of water quality have been considered in these communities. Hendryx et al. (2012a) found significantly more drinking water violations at water treatment facilities near MTR-mining activities (73.0 violations/system) than near non-surface coal mining activities (16.7 violations/system) and control areas (10.2 violations/system). The contamination violation types included: organic compounds, coliform, disinfection by-products, inorganic elements/compounds, radium, lead, and copper (Hendryx et al. 2012a). A quarterly monitoring program for domestic wells located near active mining operations found differences in iron and total suspended solids concentrations during a three-week period during blasting events (OSMRE 2002). Some studies evaluated ground water quality around surface mining operations and found the water chemistry to be unfit for human consumption, but wells or municipal water supplies were not tested (Bonta et al. 1992; Corbett 1977; Hamon et al. 1979; O'Bara and Don Estes 1985).
Numerous other studies were identified that are not directly relevant to understanding human health impacts of MTR mining, but provide broader insights into the impact of MTR mining on the environment (see Supplemental Reference Lists). These include impacts of mining on the land, water, and stream fauna. These effects may indirectly impact human health through exposure to chemicals in streams and ground water or through consumption of stream biota and contaminated fish.
These studies focused on the watersheds, streams, and landscapes near mining operations in the Appalachian region. Studies were categorized into impacts of coal mining on:
Land use and geomorphic changes;
Wetlands and hydrologic changes;
Water chemistry and quality; and
Abundance and diversity of benthic macroinvertebrates, and microbial, avian, fish, and insect species in streams associated with such mining activities.
The methodologies used in these studies included field sampling and analytical chemistry, as well as modeling, regression, and prediction methods (e.g., generalized additive models, principal component analysis, satellite data, landscape-based cumulative effects models). References identified are listed by two categories in the Supplemental Reference Lists: impact on water chemistry/quality and impact on the aquatic ecosystem.
Impact on water chemistry/quality
Most studies found significant impact on the water quality and chemistry of streams that were disturbed by MTR-mining operations, including changes in pH, specific conductance, concentration of metals, trace elements, turbidity, isotopes, dissolved inorganic carbon, organic carbon, dissolved solids, suspended solids, sediments, hardness, PAHs, etc. If the chemical constituents are above the recommended or regulatory exposure levels, consumption of such poor-quality water could be potentially harmful for humans. However, none of these studies extrapolated results to specifically predict or estimate the impacts on human health resulting from this water consumption.
Impact on the aquatic ecosystem
Abundance and diversity of aquatic species and stream biota were examined in many studies, including macroinvertebrates, avian, microbial, fish, insect, and amphibian communities and populations. These studies found significant impacts due to MTR operations in the mining areas compared to undisturbed areas. Many of these studies concluded that the impacts of MTR mining on the aquatic ecosystem could directly impact recreational fishing and indirectly negatively influence a general sense of well-being in local residents (McGarvey and Johnston 2013; Zullig and Hendryx 2010).
Studies of MTR mining impacts on the air, water, and surrounding ecosystem point to what impacts might be expected based on established health effects of components of these exposures. PM2.5, PM10 and other air pollutants contribute to adverse cardiopulmonary health and premature death (EPA 2009). Hydrogen sulfide is a respiratory irritant at low levels and may cause long-term central nervous system effects in some people, including headaches and poor neurological function (ATSDR 2014). Future research in human populations should include appropriate measures of exposures to these chemical mixtures and focus on cardiopulmonary or neurological endpoints, particularly indicators of acute exposure that may contribute to chronic disease.
Limitations of this systematic review
The focus of this systematic review was on MTR mining including studies of surface or unspecified Appalachian coal mining conducted in the last 25 years (when MTR mining became predominant). This review did not include related types of coal mining outside of this region that may be relevant to community health exposures as covered in recent systematic reviews by Jenkins et al. (2013) of coal mining and cancer and Mactaggart et al. (2016) of mining in rural communities in high-income countries. Although perhaps limiting, we felt justified focusing on the potential health effects from MTR mining in the Appalachian Mountains. MTR mining has been in practice since the 1960s, and ramped up in the 1990s with amendments to the Clear Air Act, which promoted a reduction of sulfur emissions from coal plants. Subsequently, low-sulfur, high-efficiency, coal became high in demand, and mining of low-sulfur coal deposits increased. These deposits are located in the Appalachian Mountains of West Virginia, Ohio, Kentucky, southern Virginia, and eastern Tennessee. Improvements to MTR mining techniques have made this method of surface mining preferable to strip mining, which only extracts surface coal. However, MTR mining is far more destructive than strip mining, using dynamite to blast mountaintops in order to access coal seams deep inside mountains, contaminating water and creating “coal dust that settles like pollen” over residential areas (Baller and Pantilat 2007; Fox 1999). Thus, the specific surface mining technique of MTR mining, coupled with the Appalachian region’s unique geography and geology, warranted a specific review of the health effects of MTR mining in these areas.
Only four occupational studies were identified by our search that met the inclusion criteria, yet unpublished data likely exists on MTR-mining workers’ exposures and health, perhaps in work records. The risk of bias assessment considered high-level differences in exposure characterization (e.g., direct vs. indirect) and did not delve into relative strengths and weaknesses of indirect measures - for example, using a geographic information systems method to estimate community proximity to several coal mining activities versus a county-level tonnage measure (Hendryx et al. 2010). The protocol was not tailored to distinguish between these indirect assessments of personal exposure, which is a limitation of the risk of bias assessment. While the studies of MTR mining-related exposures were included here to provide context to the health outcome studies, these studies were not critically evaluated for potential sources of bias in their design and conduct.
The studies of exposures associated with MTR mining indicate that these activities cause the release of various chemicals and particulate matter into the surrounding air/water. These chemicals could in turn contribute to the poor health outcomes reported in the exposed areas. However, a direct link between the exposures and health effects cannot be confirmed, given the following limitations. The human health effects studies could not be combined quantitatively in a meta-analysis, as outcomes were either disparate (e.g., cardiopulmonary studies included a variety of self-reported and hospitalization outcomes) or studies had significant overlap in subjects such that estimates could not be considered independent (e.g. mortality in Appalachia). The available health effects studies had exposure assessment methods that were high risk of bias not tied to individual study participants. Ideally, point measures of air pollution and water contaminants would occur at the appropriate window of exposure (prior to the development of the outcome or incorporating information on longitudinal trends) and consider distribution patterns of air and water through this mountainous region. Water source (e.g. private well or municipal supply) was also not available in the human studies. Without individual subject level data, critical confounding variables (e.g., smoking, socioeconomic status) could not be incorporated into the analysis to minimize bias. Future studies should be designed to minimize the potential for bias by enrolling individual subjects and improving exposure assessment methods. While these types of studies are inherently more challenging to conduct, several well-conducted smaller studies could be combined through meta-analysis if they use comparable methods.
Conclusion
The aim of this review was to evaluate the existing literature assessing the exposure to and health effects of chemicals released by MTR mining, identify data gaps, and provide recommendations to strengthen the design and conduct of future studies. The observational literature identified by this systematic review was found to include inconsistent associations of MTR mining with a variety of human health effects (e.g., cardiopulmonary effects, mortality, and general health status). It was also found that these studies were not designed to tie individual-level exposure data to individual-level health effects, raising the potential for bias in the reported results. Experimental studies and measured exposures in the environment support the plausibility of effects on residents near open coal mining operations, but observational studies require stronger, more direct methods of exposure assessment. We identify a critical need for studies that employ direct methods for assessing individual exposure levels tied to health effects, including early indicators of impacts such as cardiopulmonary function tests. Particulate matter in the air and contaminants in the water supply can adversely affect the people who breathe and drink them, but without this additional research, the contribution of MTR mining on the health of residents in nearby communities cannot be fully assessed.
Supplementary Material
Highlights.
Identified inconsistent results across a broad range of diverse health effects
Critical limitations in the study design of observational studies in communities
Experimental animal models support the plausibility of adverse health outcomes
Individual mining contaminants associated with previously identified health impacts
Acknowledgments
The authors appreciate the input of the anonymous reviewers of the manuscript who provided suggestions to improve the paper and the internal reviewers in the National Toxicology Program, Cynthia Rider and Andrew Rooney. We would like to thank the following reviewers of the protocol and manuscript prior to submission: Frank Bove (CDC/ATSDR), Kacee Deener (US EPA), Michael McCawley, (WVU), Jerome A. Paulson (GWU), and Lora Werner (CDC/ATSDR). We also acknowledge project management provided by Courtney Skuce and Cara Henning (ICF) in coordinating the work with NIEHS.
Funding Sources: This work was supported by the National Toxicology Program at the National Institute of Environmental Health Sciences, National Institutes of Health with portions of this work performed by ICF under contract No WA OLPR-1-03.
This work was supported by the National Toxicology Program at the National Institute of Environmental Health Sciences, NIH. The protocol was registered in PROSPERO (2016:CRD42016037192).
Abbreviations
- ARIES
Appalachian Research Initiative for Environmental Science
- EPA
Environmental Protection Agency
- HAWC
Health Assessment Workspace Collaborative
- H2S
hydrogen sulfide
- MTR
mountaintop removal
- NTP
National Toxicology Program
- OHAT
Office of Health Assessment and Translation
- PAH
polycyclic aromatic hydrocarbon
- PECO
Population, Exposure, Comparator, and Outcome
- PEL
permissible exposure limit
- PM
particulate matter
- TDS
total dissolved solids
- TSP
total suspended particles
- TSS
total suspended solids
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Acton PM, Fox JF, Campbell JE, Jones AL, Rowe H, Martin D, et al. Role of soil health in maintaining environmental sustainability of surface coal mining. Environmental science & technology. 2011;45:10265–10272. doi: 10.1021/es202764q. [DOI] [PubMed] [Google Scholar]
- Ahern M, Mullett M, Mackay K, Hamilton C. Residence in coal-mining areas and low-birth-weight outcomes. Maternal and child health journal. 2011;15:974–979. doi: 10.1007/s10995-009-0555-1. [DOI] [PubMed] [Google Scholar]
- Ahern MM, Hendryx M, Conley J, Fedorko E, Ducatman A, Zullig KJ. The association between mountaintop mining and birth defects among live births in central appalachia, 1996–2003. Environmental research. 2011;111:838–846. doi: 10.1016/j.envres.2011.05.019. [DOI] [PubMed] [Google Scholar]
- Aneja VP, Isherwood A, Morgan P. Characterization of particulate matter (pm10) related to surface coal mining operations in appalachia. Atmospheric Environment. 2012;54:496–501. [Google Scholar]
- Aneja VP, Pillai PR, Isherwood A, Morgan P, Aneja SP. Particulate matter pollution in the coal-producing regions of the appalachian mountains: Integrated ground based measurements and satellite analysis. Journal of the Air & Waste Management Association (1995) 2016 doi: 10.1080/10962247.2016.1245686. [DOI] [PubMed] [Google Scholar]
- ATSDR. Toxicological profile for hydrogen sulfide /carbonyl sulfide (draft for public comment) Atlanta, GA: 2014. [Google Scholar]
- Baller M, Pantilat LJ. Defenders of appalachia: The campaign to eliminate mountaintop removal coal mining and the role of public justice. Environmental Law. 2007;37:629. [Google Scholar]
- Bero LA. Why the cochrane risk of bias tool should include funding source as a standard item. Cochrane Database Syst Rev. 2013:ED000075. doi: 10.1002/14651858.ED000075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bonta JV, Amerman CR, Dick WA, Harlukowicz TJ, Razem AC. Impact of surface coal-mining on 3 ohio watersheds - groundwater chemistry. Water Resources Bulletin. 1992;28:597–614. [Google Scholar]
- Borak J, Salipante-Zaidel C, Slade MD, Fields CA. Mortality disparities in appalachia: Reassessment of major risk factors. Journal of occupational and environmental medicine /American College of Occupational and Environmental Medicine. 2012;54:146–156. doi: 10.1097/JOM.0b013e318246f395. [DOI] [PubMed] [Google Scholar]
- Boyles AL, Skuce C, Henning C. Mountaintop removal mining: Impacts on health in the surrounding community. PROSPERO International prospective register of systematic reviews 2016 [Google Scholar]
- Brink LL, Talbott EO, Stacy S, Marshall LP, Sharma RK, Buchanich J. The association of respiratory hospitalization rates in wv counties, total, underground, and surface coal production and sociodemographic covariates. Journal of occupational and environmental medicine /American College of Occupational and Environmental Medicine. 2014;56:1179–1188. doi: 10.1097/JOM.0000000000000246. [DOI] [PubMed] [Google Scholar]
- Buchanich JM, Balmert LC, Youk AO, Woolley SM, Talbott EO. General mortality patterns in appalachian coal-mining and non-coal-mining counties. Journal of occupational and environmental medicine /American College of Occupational and Environmental Medicine. 2014;56:1169–1178. doi: 10.1097/JOM.0000000000000245. [DOI] [PubMed] [Google Scholar]
- CDC. Silicosis screening in surface coal miners--pennsylvania, 1996–1997. MMWR Morbidity and mortality weekly report. 2000;49:612–615. [PubMed] [Google Scholar]
- CDC. Pneumoconiosis and advanced occupational lung disease among surface coal miners--16 states, 2010–2011. MMWR Morbidity and mortality weekly report. 2012;61:431–434. [PubMed] [Google Scholar]
- Christian WJ, Huang B, Rinehart J, Hopenhayn C. Exploring geographic variation in lung cancer incidence in kentucky using a spatial scan statistic: Elevated risk in the appalachian coal-mining region. Public health reports (Washington, DC : 1974) 2011;126:789–796. doi: 10.1177/003335491112600604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corbett RG. Effects of coal mining on ground and surface water quality, monongalia county, west virginia. Science of the Total Environment, The. 1977;8:21–38. [Google Scholar]
- EPA US. 2009 final report: Integrated science assessment for particulate matter. Washington, DC: 2009. EPA/600/R-08/139F. [Google Scholar]
- Esch L, Hendryx M. Chronic cardiovascular disease mortality in mountaintop mining areas of central appalachian states. The Journal of rural health : official journal of the American Rural Health Association and the National Rural Health Care Association. 2011;27:350–357. doi: 10.1111/j.1748-0361.2011.00361.x. [DOI] [PubMed] [Google Scholar]
- Ettinger WS, McClure RE. Fugitive dust generation on a southern west virginia surface coal mine. 1983:45–53. [Google Scholar]
- Fox J. Mountaintop removal in west virginia an environmental sacrifice zone. Organ Environ. 1999;12:163–183. [Google Scholar]
- Hamon WR, Bonta JV, Haghiri F, Helgesen J. Research on the hydrology and water quality of watersheds subjected to surface mining - 1. Premining hydrologic and water quality conditions. 1979:70–98. [Google Scholar]
- Hendryx M, Ahern MM, Nurkiewicz TR. Hospitalization patterns associated with appalachian coal mining. Journal of toxicology and environmental health Part A. 2007;70:2064–2070. doi: 10.1080/15287390701601236. [DOI] [PubMed] [Google Scholar]
- Hendryx M, Ahern MM. Relations between health indicators and residential proximity to coal mining in west virginia. American journal of public health. 2008;98:669–671. doi: 10.2105/AJPH.2007.113472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hendryx M, O'Donnell K, Horn K. Lung cancer mortality is elevated in coal-mining areas of appalachia. Lung cancer (Amsterdam, Netherlands) 2008;62:1–7. doi: 10.1016/j.lungcan.2008.02.004. [DOI] [PubMed] [Google Scholar]
- Hendryx M. Mortality from heart, respiratory, and kidney disease in coal mining areas of appalachia. International archives of occupational and environmental health. 2009;82:243–249. doi: 10.1007/s00420-008-0328-y. [DOI] [PubMed] [Google Scholar]
- Hendryx M, Ahern MM. Mortality in appalachian coal mining regions: The value of statistical life lost. Public health reports (Washington, DC : 1974) 2009;124:541–550. doi: 10.1177/003335490912400411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hendryx M, Zullig KJ. Higher coronary heart disease and heart attack morbidity in appalachian coal mining regions. Preventive medicine. 2009;49:355–359. doi: 10.1016/j.ypmed.2009.09.011. [DOI] [PubMed] [Google Scholar]
- Hendryx M, Fedorko E, Anesetti-Rothermel A. A geographical information system-based analysis of cancer mortality and population exposure to coal mining activities in west virginia, united states of america. Geospatial health. 2010;4:243–256. doi: 10.4081/gh.2010.204. [DOI] [PubMed] [Google Scholar]
- Hendryx M, Ahern M. Reply to borak et al. "mortality disparities in appalachia: Reassessment of major risk factors". Journal of occupational and environmental medicine /American College of Occupational and Environmental Medicine. 2012;54:768–769. doi: 10.1097/JOM.0b013e318254622f. author reply 770–763. [DOI] [PubMed] [Google Scholar]
- Hendryx M, Fulk F, McGinley A. Public drinking water violations in mountaintop coal mining areas of west virginia, USA. Water Qual Expos Health. 2012a;4:169–175. [Google Scholar]
- Hendryx M, Wolfe L, Luo J, Webb B. Self-reported cancer rates in two rural areas of west virginia with and without mountaintop coal mining. Journal of community health. 2012b;37:320–327. doi: 10.1007/s10900-011-9448-5. [DOI] [PubMed] [Google Scholar]
- Hendryx M. Personal and family health in rural areas of kentucky with and without mountaintop coal mining. The Journal of rural health : official journal of the American Rural Health Association and the National Rural Health Care Association. 2013;29(Suppl 1):s79–88. doi: 10.1111/jrh.12016. [DOI] [PubMed] [Google Scholar]
- Hendryx M, Entwhistle J. Association between residence near surface coal mining and blood inflammation. Extractive Industries and Society. 2015;2:246–251. [Google Scholar]
- Hendryx M, Luo J. An examination of the effects of mountaintop removal coal mining on respiratory symptoms and copd using propensity scores. International journal of environmental health research. 2015;25:265–276. doi: 10.1080/09603123.2014.938027. [DOI] [PubMed] [Google Scholar]
- Hendryx M, Holland B. Unintended consequences of the clean air act: Mortality rates in appalachian coal mining communities. Environmental Science & Policy. 2016;63:1–6. [Google Scholar]
- Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The cochrane collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi: 10.1136/bmj.d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hitt NP, Hendryx M. Ecological integrity of streams related to human cancer mortality rates. EcoHealth. 2010;7:91–104. doi: 10.1007/s10393-010-0297-y. [DOI] [PubMed] [Google Scholar]
- Holzman DC. Mountaintop removal mining: Digging into community health concerns. Environmental health perspectives. 2011;119:A476–483. doi: 10.1289/ehp.119-a476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jenkins WD, Christian WJ, Mueller G, Robbins KT. Population cancer risks associated with coal mining: A systematic review. PloS one. 2013;8:12. doi: 10.1371/journal.pone.0071312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knuckles TL, Stapleton PA, Minarchick VC, Esch L, McCawley M, Hendryx M, et al. Air pollution particulate matter collected from an appalachian mountaintop mining site induces microvascular dysfunction. Microcirculation (New York, NY : 1994) 2013;20:158–169. doi: 10.1111/micc.12014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kurth L, Kolker A, Engle M, Geboy N, Hendryx M, Orem W, et al. Atmospheric particulate matter in proximity to mountaintop coal mines: Sources and potential environmental and human health impacts. Environmental geochemistry and health. 2015;37:529–544. doi: 10.1007/s10653-014-9669-5. [DOI] [PubMed] [Google Scholar]
- Kurth LM, McCawley M, Hendryx M, Lusk S. Atmospheric particulate matter size distribution and concentration in west virginia coal mining and non-mining areas. Journal of exposure science & environmental epidemiology. 2014;24:405–411. doi: 10.1038/jes.2014.2. [DOI] [PubMed] [Google Scholar]
- Lamm SH, Li J, Robbins SA, Dissen E, Chen R, Feinleib M. Are residents of mountain-top mining counties more likely to have infants with birth defects? The west virginia experience. Birth Defects Research Part A - Clinical and Molecular Teratology. 2015;103:76–84. doi: 10.1002/bdra.23322. [DOI] [PubMed] [Google Scholar]
- Luanpitpong S, Chen M, Knuckles T, Wen S, Luo J, Ellis E, et al. Appalachian mountaintop mining particulate matter induces neoplastic transformation of human bronchial epithelial cells and promotes tumor formation. Environmental science & technology. 2014;48:12912–12919. doi: 10.1021/es504263u. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Macleod MR, Lawson McLean A, Kyriakopoulou A, Serghiou S, de Wilde A, Sherratt N, et al. Risk of bias in reports of in vivo research: A focus for improvement. PLoS Biol. 2015;13:e1002273. doi: 10.1371/journal.pbio.1002273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mactaggart F, McDermott L, Tynan A, Gericke C. Examining health and well-being outcomes associated with mining activity in rural communities of high-income countries: A systematic review. The Australian journal of rural health. 2016;24:230–237. doi: 10.1111/ajr.12285. [DOI] [PubMed] [Google Scholar]
- McGarvey DJ, Johnston JM. 'Fishing' for alternatives to mountaintop mining in southern west virginia. Ambio. 2013;42:298–308. doi: 10.1007/s13280-012-0346-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nichols CE, Shepherd DL, Knuckles TL, Thapa D, Stricker JC, Stapleton PA, et al. Cardiac and mitochondrial dysfunction following acute pulmonary exposure to mountaintop removal mining particulate matter. American journal of physiology Heart and circulatory physiology. 2015;309:H2017–2030. doi: 10.1152/ajpheart.00353.2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O'Bara CJ, Don Estes R. Acid mine drainage contaminates groundwater of a tennessee watershed. Environmental Geology and Water Sciences. 1985;7:159–161. [Google Scholar]
- OSMRE. Comparative study of domestic water well integrity to coal mine blasting: Summary report. Govt Reports Announcements & Index. 2002:272. [Google Scholar]
- Palmer MA, Bernhardt ES, Schlesinger WH, Eshleman KN, Foufoula-Georgiou E, Hendryx MS, et al. Science and regulation. Mountaintop mining consequences. Science (New York, NY) 2010;327:148–149. doi: 10.1126/science.1180543. [DOI] [PubMed] [Google Scholar]
- Piacitelli GM, Amandus HE, Diefenbach A. Respirable dust exposures in USA surface coal mines (1982–1986) Archives of environmental health. 1990;45:202–209. doi: 10.1080/00039896.1990.9940803. [DOI] [PubMed] [Google Scholar]
- Pope R, Wu JG. A multi-objective assessment of an air quality monitoring network using environmental, economic, and social indicators and gis-based. J Air Waste Manage Assoc. 2014;64:721–737. doi: 10.1080/10962247.2014.888378. [DOI] [PubMed] [Google Scholar]
- Prince TS, Frank AL. Causation, impairment, disability: An analysis of coal workers' pneumoconiosis evaluations. Journal of occupational and environmental medicine /American College of Occupational and Environmental Medicine. 1996;38:77–82. doi: 10.1097/00043764-199601000-00020. [DOI] [PubMed] [Google Scholar]
- Simmons JA, Currie WS, Eshleman KN, Kuers K, Monteleone S, Negley TL, et al. Forest to reclaimed mine land use change leads to altered ecosystem structure and function. Ecological Applications. 2008;18:104–118. doi: 10.1890/07-1117.1. [DOI] [PubMed] [Google Scholar]
- Simonton DS. Hydrogen sulfide exposure and human-health risk in mining–impacted regions. 2014:1001–1009. [Google Scholar]
- Talbott EO, Sharma RK, Buchanich J, Stacy SL. Is there an association of circulatory hospitalizations independent of mining employment in coal-mining and non-coal-mining counties in west virginia? Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine. 2015;57:e30–36. doi: 10.1097/JOM.0000000000000425. [DOI] [PubMed] [Google Scholar]
- Turner EA, Kroeger GL, Arnold MC, Thornton BL, Di Giulio RT, Meyer JN. Assessing different mechanisms of toxicity in mountaintop removal/valley fill coal mining-affected watershed samples using caenorhabditis elegans. PloS one. 2013;8:e75329. doi: 10.1371/journal.pone.0075329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woolley SM, Meacham SL, Balmert LC, Talbott EO, Buchanich JM. Comparison of mortality disparities in central appalachian coal- and non-coal-mining counties. Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine. 2015a;57:687–694. doi: 10.1097/JOM.0000000000000435. [DOI] [PubMed] [Google Scholar]
- Woolley SM, Youk AO, Bear TM, Balmert LC, Talbott EO, Buchanich JM. Impact of coal mining on self-rated health among appalachian residents. Journal of environmental and public health. 2015b;2015:501837. doi: 10.1155/2015/501837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Young RC, Jr, Rachal RE. Pulmonary disability in former appalachian coal miners. Journal of the National Medical Association. 1996;88:517–522. [PMC free article] [PubMed] [Google Scholar]
- Zullig KJ, Hendryx M. A comparative analysis of health-related quality of life for residents of u.S. Counties with and without coal mining. Public health reports (Washington, DC : 1974) 2010;125:548–555. doi: 10.1177/003335491012500410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zullig KJ, Hendryx M. Health-related quality of life among central appalachian residents in mountaintop mining counties. American journal of public health. 2011;101:848–853. doi: 10.2105/AJPH.2010.300073. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.