

Abstract
Introduction:
Hospitalization of patients with cancer has a significant economic impact and avoidance where unnecessary has great potential for significant cost savings for patients, individual hospitals and the health system in general.
Methods:
Demographic, clinical and economical data were collected from medical records in our hospital retrospectively. Oncology clinicians reviewed medical records to categorize each hospitalization as “potentially avoidable” or “not avoidable.” Patient demographic and clinical data were abstracted and quantitative and qualitative analyses were performed to identify patient characteristics and outcomes associated with potentially avoidable hospitalizations. Finally data on the cost of the latter were estimated.
Results:
Of 451 hospitalizations, medical oncologists identified 55 (12.2%) as potentially avoidable. Avoiding these and caring for the patients in alternative locations would save some $ US 641,240 yearly. Among patients with avoidable hospitalization, 70.9% were males and the median age and median length of stay was 55 years and 4.7 days. Most of them had general signs (83.6%) and a fever body temperature lower than 38.5’C (96.4%). Lung, kidney and urinary tract cancers were the most common diagnoses (10.9%). The majority of avoidable hospitalized patients had local cancer (85.5%) and poor performance status (43.6%). The most prevalent procedure for patients with avoidable hospitalization was sonography and the least frequent were laboratory tests and MRI. Most cases received no treatment.
Conclusion:
Avoidable hospitalizations are common in patients with cancer. Age, final results of hospitalization and length of stay were established as significant variables for patients with avoidable hospitalization.
Keywords: Avoidable hospitalization, economic burden, patients with cancer
Introduction
Cancer is one of the main causes of disorders, mortality and inability around the world and has been increased so dramatically. Thus, it is natural that most of decisions and the measures in health care systems and resources have been allocated for its treatment and management (Hatam et al., 2015). Cancer is defined as the fast and abnormal growth and development of body cells so that all body organs can be affected. However, many sorts of them are preventable and curable (Stewart and Wild, 2014) In spite of considerable improvements in medicine, cancer is known as the main cause of inability and mortality (Jemal et al., 2010). According to WHO’s statistical figures, 14.1 million new cases suffering from cancer have been recognized in 2012 and 8.2 million people died due to this disease around the world in the same year (Stewart and Wild, 2014; Prevention Quality Indicators Overview, 2012). In Iran, as a developing country, cancer is the third cause of death and its prevalence is estimated 110.4 and 98.2 males and females per one hundred thousand people (Mousavi et al., 2008; Kolahdoozan et al., 2010). The cares provided for these patients are varied. However, the hospitalization of some of them, especially in the end stages, can be avoidable (Chang Cyril, 2009; Brooks et al., 2014). In general, hospitalization is a stressful and expensive experience for the clients and their families (Ouslander et al., 2010; Morden et al., 2012). Ouslander et al. found that hospital admissions lead to discomfort, anxiety and inability for the patients and their families and an increase in their costs. They believed that most of these hospitalizations can be replaced by effective outpatient cares (Ouslander et al., 2010). Brooks et al. stated that potentially avoidable hospitalizations are widespread among patients suffering from GI cancers which are done in the last months of life (Brooks et al., 2014). According to Agency for Healthcare Research and Quality’s statement in the U.S, avoidable hospitalization is the condition in which patient’s hospitalization and unnecessary consumption of hospital resources can be avoided by providing outpatient services effectively and timely before they become seriously ill. This is supposed to be done in primary health centers with qualified management (Foote et al., 2008; Chang Cyril, 2009; Prevention Quality Indicators Overview, 2012). The hospital services and resources are known as the major parts of health system’s costs economically (Yabroff et al., 2008). Regarding high treatment and prevention costs of cancer, the economical burden of this disease has been increased considerably by increasing health system costs accompanied with demographic changes and the senility of the population. This will lead to increased financial burden for the governments, especially in developing ones such as Iran (Aprile et al., 2013). It is clear that adjusting high level of costs specified for cancer should be prioritized at top levels. It needs health system official’s consideration for controlling the elevating growth of cancer costs and providing high quality cares (Yabroff et al., 2008). Since hospitalization leads to increase in the costs rather than outpatient services (14), it is necessary to take measures in order to decrease avoidable hospitalization. This is done for achieving high quality cares, awareness in specifying the cost and client-centered cares (Smith and Hillner, 2011).
To the best of our knowledge, since no study has been done in Iran about this issue and also few projects have been done in other regions of the world about economic effect of avoidable hospitalization for the patients suffering from cancer (Bindman et al., 2005; Foote et al., 2008; Torio et al., 2013; Brooks et al., 2014), the present study can be effective in order to find the clients in need of admission, avoid from providing unnecessary hospital services and, subsequently, decrease high costs of health care and treatment of cancer for the patients and also health system. Therefore, we studied the financial burden of avoidable hospitalizations among the patients with cancer in Namazi hospital in Shiraz (a south Iranian city) as the main center of providing hospital services for the mentioned patients.
Materials and Methods
This is a cross-sectional, descriptive-analytical study which was conducted retrospectively to study the financial burden imposed on the patients who were suffering from cancer and were hospitalized in Namazi hospital in Shiraz (in Iran) in 2013. Financial burden was counted based on Iran’s national currency (Rial). In order to change it into dollar, the average price of dollar was searched from Iranian Central Bank’s reports in 2013. Then, the costs (based on Rial) were divided by the average price of dollar in the mentioned year for computing the rate of costs based on dollar. In the present study, all of the hospitalized patients with cancer (2834 patients) in hematology, oncology, emergency and internal medicine wards of Namazi hospital in 2013 were the subjects of this study, because this hospital is the biggest general hospital in southern Iran and most cancerous patients are referring to it. If a patient was hospitalized some times during the year, all hospitalizations were regarded. According to the conducted studies, the percentage of avoidable hospitalization has been reported between 4 to 30 percent. Since the average percentage of avoidable hospitalization was about 15 percent in the mentioned studies (p=0.15) (Bindman et al., 2005; Barron et al., 2008; Johnson et al., 2012, Brooks et al., 2014), the accuracy and confidence level were supposed 5% (d=0.05) and 95% (1-α=0.95), respectively. The sample size was extracted based on the following formula:
Therefore, the lowest number of the cases in our study was estimated 196. However, it was possible to gather the data of more patients so that 451 patients were studied. This was done to achieve more reliable and precise results which can be generalized as well. The studied patients were selected randomly so that a random number, from zero to nine, was selected by the use of random numbers table. Then, the total number of the community was divided by the number of the sample size. The obtained number was added to the first random number for selecting the first studied case and so on to select all cases.
Recognizing avoidable hospitalization
In order to collect information, the researchers designed a data gathering form and the necessary information found in other studies (Bindman et al., 2005; Ouslander et al., 2010; Torio et al., 2013; Brooks et al., 2014) was used as well. The mentioned form was localized according to the studied patient’s conditions. It contained five parts. The first part included their demographic information such as age, gender, the type of a health insurance, and the time and numbers of admission per year. The second part contained cancer diagnostic data and admission time, treatment and the cares provided for the patients and the information of patient’s mortality. The third part determined the rate of avoidability of the hospitalizations among the admitted cases based on four-option format. These options included absolute unavoidable hospitalization, possibly unavoidable hospitalization, possibly avoidable hospitalization, and absolute avoidable hospitalization. In order to complete this part, three oncologists were asked to assist the researcher through “expert opinion” framework. Each of these specialists investigated individually the necessity of the patient’s hospitalization and gave their opinion based on four mentioned options. The last part of the form included the data on the cost of the patient’s supposed to be avoidable hospitalization case within the period of their hospitalization in hospital. It consisted of treatment costs, diagnostic measures, medicines, laboratory tests and all therapeutical measures. They were extracted from the patient’s bill in order to determine the financial burden.
T-test and Chi-square test were used to determine the relationship between quantitative and qualitative variables with avoidable hospitalization. In order to cluster the patients and determine final significant variables, logistic regression and forward stepwise method were used. Finally, the collected data were analyzed through SPSS (version 18). The level of agreement between the consultants was assessed by Cohen’s Kappa coefficient. In addition, the significance level was determined 0.05 in this study.
Results
The number of studied cases was 451; among them 396 (87.8%) and 55 cases (12.2%) had unavoidable and voidable hospitalization, respectively. 266 cases (59%) were males and 185 (41%) were females. In addition, the number of males was more than females among those having avoidable hospitalization (70.9%). The mean age of the patients with avoidable and unavoidable hospitalization was reported 55±19.2 and 48±19.3 years old, respectively.
55 percent of the studied cases used Iran Health Insurance and 33.9 percent of them were covered by Social Security Insurance.
One of the most important factors determining the decision of the patients’ hospitalization includes the presence of general signs (such as weakness, lethargy and tiredness) and specific ones (such as bleeding and infection). The result of the present study showed that 79.3, 16 and 4.7 percent of the studied patients complained about general, specific and both types of signs, respectively. On the other hand, 83.6 percent of the cases, in avoidable hospitalization group, had general signs. 34.8 and 38.2 percent of the patients with unavoidable and avoidable hospitalization suffered from another disease in addition to cancer and metastasis respectively.
Since having body temperature (fever) over 38.5 °C is an important factor in making decision for hospitalizing the patients, the findings of present study showed that 87.6 and 96.4 percent of unavoidable and avoidable hospitalization groups complained about body temperature (fever) less than 38.5°C, respectively.
The mean length of the stay of the patients with unavoidable and avoidable hospitalization was 9.7±9.54 and 4.7±6.6 days, respectively (with 9.5 and 6.6 standard deviation, respectively).
There was a significant relationship between length of stay and avoidable hospitalization (p<0.001). It means that the patients with avoidable hospitalization had fewer days of staying in hospital. The mean of hospitalization number in the year was 2.1±1.8 and 1.7±1.3 times for unavoidable and avoidable hospitalization group, respectively.
The commonest diagnosis of patients on admission in those with unavoidable hospitalization were lymphoma and leukemia (11.1%). Lung, kidney and urinary tract cancers were the most prevalent ones for the patients with avoidable hospitalization (10.9%).
The distribution of the cancer among the studied cases was investigated and the results showed that 75.3 percent of the patients with unavoidable hospitalization and 85.5 percent of those with avoidable hospitalization suffered from localized cancer. Also, 24.7 and 14.5 percent of the mentioned patients had metastatic cancer, respectively.
The clinical situation of the patients was also studied and results are shown in the Table 1:
Table 1.
The Clinical Situation of the Patients During Hospitalization among Patients with Cancer in Namazi Hospital in Shiraz in 2013
| Hospitalization situation | Unavoidable | Avoidable | Total | |||
|---|---|---|---|---|---|---|
| Clinical situation of the patients during hospitalization | number | percentage | number | percentage | number | percentage |
| Refractory to standard therapy | 42 | 10.6 | 1 | 1.9 | 43 | 9.5 |
| Poor performance status | 140 | 35.4 | 24 | 43.5 | 164 | 36.4 |
| Advised to consider care | 158 | 39.9 | 22 | 40 | 180 | 39.9 |
| None | 56 | 14.1 | 8 | 14.6 | 64 | 14.2 |
| Total | 396 | 100.0 | 55 | 100.0 | 451 | 100.0 |
The most prevalent procedure done for 42.2 percent of patients with unavoidable hospitalization and 34.5 percent of patients with avoidable hospitalization was sonography and the least procedure was laboratory tests for the same mentioned patients with 2 and 1.8 percent, respectively.
30.1 and 24.1 percent of the patients with unavoidable and avoidable hospitalization received surgery, respectively. 12.6% and 16.7% of the mentioned cases received radiotherapy as well. 10.4% and 11.1% of those two groups underwent chemotherapy. These findings are shown in the diagram 1:
Diagram 1.
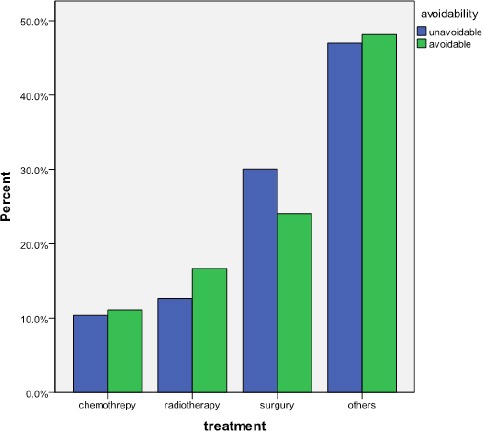
Treatment Performed for Hospitalized Patients with Cancer in Nemazi Hospital in Shiraz in 2013 According to Unavoidable and Avoidable Hospitalization Respectively
According to the findings of the present study, 61.9% and 90.9% of the patients with unavoidable and avoidable hospitalization were discharged from the hospital. The final result of hospitalization for 38.1% of patients with unavoidable hospitalization and 9.1% of patients with avoidable hospitalization was death. Thus, there was a significant relationship between death and avoidable hospitalization with a significant level of <0.001. It means that the rate of death among the patients with avoidable hospitalization was very low. According to the specialists’ opinion, the patients who died, needed to be hospitalized in hospital unavoidably. The commonest reason of death among the patients (71.3%) was metastasis or the cancer itself.
The findings related to the financial burden
Based on the findings of the present study, the total cost of avoidable hospitalization was $ US 64,115; about $ US 51,175 of which was covered with insurances and health subsidies, and $ US 12,372 to the patient’s payment, respectively. highest rates were paid for the medicine taken in the ward was $ US 26,159 and the services and instruments was $ US 11,596. The next highest costs were paid for laboratory and hotelling. In addition, for the majority of the patients (90 percent) with avoidable hospitalization, medication used and after that, the laboratory tests for 87 percent and services and instruments in the ward were used for 85 percent.
Discussion
The present study investigated the necessity of hospitalization which was done for the hospitalized patients with cancer in Nemazi hospital in Shiraz (south of Iran) (Eggli et al., 2012). Among 451 hospitalized patients in the mentioned hospital, 55 cases (12.2%) were recognized as avoidable hospitalization. Gardiner et al. (2013) reported that the rate of avoidable hospitalization was 7.2 percent among the patients with GI cancer. Brooks et al. (2014) and Gott et al. (2013) reported this rate as 19% and 6.7%, respectively.
It seems that our findings are near to the mean rates of similar studies. The estimated point, in the present study, is the lack of any standard protocol as the guideline for determining if the patients are necessary to be hospitalized in the hospital or not. Therefore, it sounds to be essential to determine a basis for making suitable decisions about hospitalization. It, of course, is important to attract the decision-makers’ attention about this issue.
The findings of the present study show that age, as a variable, has a significant relationship with avoidable hospitalization (p=0.005). It was shown as a risk ratio. In fact, it means that the chance of avoidable hospitalization increases 1.02 times more by elevating every year of age. There are different studies with results similar to those of the present research. Different investigators emphasize that age is an effective factor to determine the necessity of hospitalization among patients which imposes back breaking expenses on them. Brooks et al., (2014), Stranges and Stocks (2008), O’neil et al., (2015) and Yam et al., (2010) found in their studies that the mean ages of 70, 65, 46, and 74.8 years old are the significant factors in determining avoidable hospitalization. In addition, it is found that avoidable hospitalization occurred more among old people rather than young ones. Therefore, it is better to use social and outpatient cares for old people instead of hospitalization for reducing physical, mental and financial pressures on the patients and their families.
On the other hand, length of stay in the hospital is related significantly to the avoidablity of hospitalization (p<0.0001), so that the avoidable hospitalization will decrease to 0.1 if the length of stay is increased one day since the patients with avoidable hospitalization usually experience less length of stay. So, it seems that they don’t need to be taken care of for a long-time.
The result of the patient’s hospitalization is either discharge or death. Both mentioned situations were studied in the present project. The rate of discharge was 90 percent among the patients with avoidable hospitalization. It can be concluded that very few of the mentioned patients passed away. In addition, the final result of hospitalization, as a variable, had a significant relationship with avoidability of hospitalization (p<0.001). By increasing one dead case, the chance of avoidable hospitalization is decreased 0.17 time compared to discharge. To justify this finding, it can be declared that the dead people were in the end stages of their disease during their hospitalization and they were supposed to receive the health care in the hospital according to the specialists’ diagnosis. Therefore, the rate of avoidable hospitalization among the mentioned cases is so rare.
Although there was not any significant relationship between gender and avoidable hospitalization (p=0.55) in the present study, opposite finding was reported in Johnson et al.’s (2012) and Eggli et al.’s (2014) studies. The results showed that the prevalence of avoidable hospitalization was 70.9 percent among the males and this was more in the females.
Yam et al., (2010) found that the occurrence of avoidable hospitalization was 54.5 percent among males; this was more than the females. In contrast, Brooks et al. (2014) revealed that hospitalization among the females suffering from cancer was 56% which was more than the male patients. In spite of lack of significant relationship between gender and the situation of avoidable hospitalization in the present study, gender is still considered an effective and important factor.
The level of disease improvement, some signs of disease such as bleeding and infection, and high rate of fever (body temperature) are the influencing factors which affect the patient’s hospitalization. In the present study, fever and infection were found in 7.3 percent of the cases among the patients with avoidable hospitalization. Metastatic stage was seen in 14.5 percent of the patients with avoidable hospitalization. It sounds that most of our project’s cases with avoidable hospitalization were not in the progressive stage of their disease including the metastasis of the cancer towards other body organs and fever and infection. Thus, their hospitalization was considered as avoidable. Despite the present study’s results, Brooks et al. stated that a considerable number of patients had avoidable hospitalization (31%) and experienced fever and infection. In addition, all their studied cases were in metastasis stage of cancer.
The findings of this investigation showed that most of the patients with avoidable hospitalization (47 percent) did not receive any treatment or they received the remedies other than surgical procedures, chemotherapy and radiotherapy. According to this result which shows that hospitalized patients received no treatment during their hospitalization, it can be concluded that they were admitted in the hospital just for diagnostic or relieving procedures. Brooks et al. studied this factor. They found that the most treatment modalities done for them included social and outpatient supports.
Chemotherapy, as one of the most prevalent sorts of therapeutic measures among the patients suffering from cancer was performed rarely for the studied cases in this study (10 percent). However, this treatment was done for 86% of cases suffering from breast cancer in O’neil et al.’s study (2015). Brooks et al. found the same results as our study’s finding. They stated that avoidable hospitalization had a reverse relationship with receiving chemotherapy. Therefore, it can be concluded that those patients receiving chemotherapy have unavoidable hospitalization and it is necessary to be taken care of in hospital.
In the present study, the rate of expenses related to hospitalization of the patients suffering from cancer and also the therapeutic procedures for them have been investigated. Since financing the costs of health–related affairs is really catastrophic around the world, especially for the patients suffering from cancer and also their family members, community and the country with moderate income (Choi et al., 2014; O’Neill et al., 2015; Kim and Kwon, 2015) considering diagnostic and treatment expenses of cancer is so important.
It was shown in the present study that the highest cost was related to providing medicine and ward instruments with $ US 26,859 and $ US 11,596, respectively. Following that the costs of laboratory tests and hotelling are the highest ones $ US 4,814 and $ US 37,690, respectively). Regarding the number of patients receiving the services, the most numbers were included: ward medicine (50 patients), laboratory tests (48 ones), ward instruments (47 ones), nursing cares (46 ones) and hoteling (45 ones). As mentioned before, the highest cost paid for the patients suffering from cancer was related to their hospitalization and the next to medicine and primary cares. As it was found in our study, medicine costs are so high which needs to be taken into account during patients’ hospitalization, especially so that medicine resources wasting and, subsequently, financial burden are supposed to be controlled. In this project, the total cost of avoidable hospitalization was $ US 64,115; among them $ US 51,175 was related to insurance and health subsidies, $ US 12,940 to the patient’s contribution, and $ US 12,372 to the patient’s payment, respectively. However, hospitalization could be avoided and the patients could have received necessary services from other ways rather than hospitalization. It would have lead to decrease in the expenses. The costs of avoidable hospitalization have been studied in different investigations. Gardiner et al. (2013) found that the expenses were about 50 thousand pounds for one day and 5.9 million pounds in a year for two hospitals in England for avoidable hospitalization. Abel et al., (2009) stated that the cost of avoidable hospitalization for every patient was 3173 pounds. Jiang et al., (2009) found that annual expense of avoidable hospitalization was 30,8 milliard dollars in their study. National Audit Office in England (2007) found that the mentioned cost was 4,84 million pounds annually (Foote et al., 2008) and also Gardiner et al., (2012) stated that it was 180,000 pounds per year.
As the result, the findings of different studies show that a large amount of costs have been paid for cancer remedies. Since most of the countries are faced with the problem of providing health services resources, trying to decrease these costs and restraining health costs without diminishing the quality of services. Consequently, different studies are recommended to be conducted to investigate the importance of providing these services and also estimating financial burden from unnecessary services (Eggli et al., 2014).
In conclusion, we studied hospitalizations in patients with cancer and identified 12.2% of hospitalizations as avoidable. Potentially avoidable hospitalization was associated with Age, final result of hospitalization and length of stay. Improving the quality of outpatient cancer care can lead to reducing avoidable hospitalizations and health care costs. So, future researches should focus on the evaluation of clinical interventions targeted at reducing avoidable hospitalizations.
Acknowledgement
This research was performed by Mrs. Tannaz Fanusi in partial fulfillment of the requirements for obtaining an MSc in Health Administration at Shiraz University of Medical Sciences. This article is the result of a research project 93-7303 approved by the Deputy of Research of the aforementioned university. Also, we thank the Research Consultation Center (RCC) at Shiraz University of Medical Sciences for their invaluable assistance in editing this article.
References
- Abel J, Rich A, Griffin T, Purdy S. End of life care in hospital: A descriptive study of all inpatient deaths in 1 Year. J Palliat Med. 2009;23:616–22. doi: 10.1177/0269216309106460. [DOI] [PubMed] [Google Scholar]
- Aprile G, Pisa FE, Follador A, et al. Unplanned presentations of cancer outpatients: a retrospective cohort study. Support Care Cancer. 2013;21:397–404. doi: 10.1007/s00520-012-1524-6. [DOI] [PubMed] [Google Scholar]
- Barron JJ, Quimbo R, Nikam PT, Amonkar MM. Assessing the economic burden of breast cancer in a US managed care population. Breast Cancer Res Treat. 2008;109:367–77. doi: 10.1007/s10549-007-9650-4. [DOI] [PubMed] [Google Scholar]
- Bindman AB, Chattopadhyay A, Osmond DH, et al. The Impact of medicaid managed care on hospitalizations for ambulatory care sensitive conditions. Health Serv Res. 2005;40:19–38. doi: 10.1111/j.1475-6773.2005.00340.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooks GA, Abrams TA, Meyerhardt JA, et al. Identification of potentially avoidable hospitalizations in patients with GI cancer. J Clin Oncol Res 2014. 2014 doi: 10.1200/JCO.2013.52.4330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chang Cyril F. Potentially avoidable hospitalizations in Tennessee. The methodist le Bonheur center for healthcare economics. The university of Memphis 2009. 2012 May [Google Scholar]
- Choi J, Cho K, Choi Y, et al. Changes in economic status of households associated with catastrophic health expenditures for cancer in South Korea. Asian Pac J Cancer Prev. 2014;15:2713–17. doi: 10.7314/apjcp.2014.15.6.2713. [DOI] [PubMed] [Google Scholar]
- Eggli Y, Desquins B, Seker E, Halfon P. Comparing potentially avoidable hospitalization rates related to ambulatory care sensitive conditions in Switzerland: the need to refine the definition of health conditions and to adjust for population health status. BMC Health Serv Res. 2014;14:25. doi: 10.1186/1472-6963-14-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foote C, Bowen T, Forte P. Identifying alternatives to hospital for people at the end of life. Report of findings. The balance of care group in association with the national audit office 2008. 2008 [Google Scholar]
- Gardiner C, Ward S, Gott M, Ingleton C. Economic analysis of potentially avoidable hospital admissions in patients with palliative care needs. Prog Palliat Care. 2012;20:147–53. [Google Scholar]
- Gardiner C, Ward S, Gott M, Ingleton C. Economic impact of hospitalisations among patientsin the last year of life: An observational study. Palliat Med. 2013;28:422–9. doi: 10.1177/0269216313517284. [DOI] [PubMed] [Google Scholar]
- Gott M, Gardiner C, Ingleton C, et al. What is the extent of potentially avoidable admissions amongst hospital inpatients with palliative care needs? BMC Palliat Care. 2013;12:9. doi: 10.1186/1472-684X-12-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hatam N, Askarian M, Javan-Noghabi J, et al. Cost-utility of “Doxorubicin and Cyclophosphamide” versus “Gemcitabine and Paclitaxel” for treatment of patients with breast cancer in Iran. Asian Pac J Cancer Prev. 2015;16:8265–70. doi: 10.7314/apjcp.2015.16.18.8265. [DOI] [PubMed] [Google Scholar]
- Jemal A, Siegel R, Xu J, Ward E. Cancer Statistics. Ca Cancer J Clin. 2010;60:277–300. doi: 10.3322/caac.20073. [DOI] [PubMed] [Google Scholar]
- Jiang JH, Russo A, Barrett ML. Nationwide frequency and costs of potentially preventable hospitalizations. HCUP. Agency for Healthcare Research and Quality. 2009 April. 2009 [PubMed] [Google Scholar]
- Johnson PJ, Ghildayal N, Ward AC, et al. Disparities in potentially avoidable emergency department (ED) care: ED visits for ambulatory care sensitive conditions. Med Care. 2012;50:1020–8. doi: 10.1097/MLR.0b013e318270bad4. [DOI] [PubMed] [Google Scholar]
- Kim S, Kwon S. Impact of the policy of expanding benefit coverage for cancer patients on catastrophic health expenditure across different income groups in South Korea. Soc Sci Med. 2015;138:241–47. doi: 10.1016/j.socscimed.2015.06.012. [DOI] [PubMed] [Google Scholar]
- Kolahdoozan S, Sadjadi A, Radmard AR, Khademi H. Five common cancers in Iran. Arch Iran Med. 2010;13:143–46. [PubMed] [Google Scholar]
- Morden NE, Chang CH, Jacobson JO, et al. End-Of-Life care for medicare beneficiaries with cancer is highly intensive overall and varies widely. Health Aff (Millwood) 2012;31:786–96. doi: 10.1377/hlthaff.2011.0650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mousavi Sm, Gouya Mm, Ramazani R, et al. Cancer Incidence And Mortality In Iran. Ann Oncol. 2008;20:556–63. doi: 10.1093/annonc/mdn642. [DOI] [PubMed] [Google Scholar]
- Nakano K, Yoshida T, Furutama J, Sunada S. Quality of end-of-life care for patients with metastatic non-small-cell lung cancer in general wards and palliative care units in Japan. Support Care Cancer. 2012;20:883–88. doi: 10.1007/s00520-011-1374-7. [DOI] [PubMed] [Google Scholar]
- O’Neill KM, Mandig M, Pyda J, et al. Out-of-pocket expenses incurred by patients obtaining free breast cancer care in Haiti: A pilot study. Surgery. 2015;158:747–55. doi: 10.1016/j.surg.2015.04.040. [DOI] [PubMed] [Google Scholar]
- Ouslander JG, Lamb G, Perloe M, et al. Potentially avoidable hospitalizations of nursing home residents: frequency, causes, and costs. J Am Geriatr Soc. 2010;58:627–35. doi: 10.1111/j.1532-5415.2010.02768.x. [DOI] [PubMed] [Google Scholar]
- Prevention quality indicators overview. Agency for healthcare research and quality. U.S. department of health & human services. Available at: http://www.qualityindicators.ahrq.gov/modules/pqi_overview.aspx .
- Smith TJ, Hillner BE. Bending the cost curve in cancer care. N Engl J Med. 2011;364:2060–65. doi: 10.1056/NEJMsb1013826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stewart BW, Wild CP. World cancer report 2014. 2014. Available at: www.who.int/entity/mediacentre/factsheets/fs297/en/
- Stranges E, Stocks C, Potentially Preventable hospitalizations for acute and chronic conditions 2008. 2010 November. 2008 [PubMed] [Google Scholar]
- Torio CM, Elixhauser A, Andrews RM Trends in potentially preventable hospital admissions among adults and children 2005–2010. HCUP. Agency for healthcare research and quality. 2013 March. 2013 [PubMed] [Google Scholar]
- Yabroff KR, Lamont EB, Mariotto A, et al. Cost of care for elderly cancer patients in the United States. J Natl Cancer Inst. 2008;100:630–41. doi: 10.1093/jnci/djn103. [DOI] [PubMed] [Google Scholar]
- Yam C, Wong E, Chan F, Leung M, et al. Avoidable readmission in Hong Kong - system, clinician, patient or social factor? BMC Health Serv Res. 2010;10:311. doi: 10.1186/1472-6963-10-311. [DOI] [PMC free article] [PubMed] [Google Scholar]