

Abstract
Objective
Patients with RA often ask if specific foods, popularized as “inflammatory” or “anti-inflammatory,” can improve or worsen their RA. We surveyed patients regarding diet and RA symptoms.
Methods
We mailed a diet survey to 300 subjects in a single-center RA registry at a large academic center. Subjects were asked whether they consume each of 20 foods and whether these foods make their RA symptoms better, worse, or unchanged. Semi-annual registry data include demographics, medications, comorbidities, and disease activity scores. Fisher's exact and Wilcoxon rank-sum tests evaluated associations between subject characteristics from the most recent registry assessment and change in RA symptoms from specific foods.
Results
Among 217 subjects (72% response rate), 83% were female, median RA duration was 17 years (IQR 9-27), and 58% were using a biologic DMARD. Twenty-four percent of subjects reported that foods affect their RA, with 15% reporting improvement and 19% worsening. Blueberries and spinach were the foods most often reported to improve RA symptoms, while soda with sugar and desserts were most often reported to worsen RA symptoms. Younger age and noting that sleep, warm room temperature, and vitamin/mineral supplements improve RA were each associated with reporting that foods affect RA symptoms. Medication use, sex, body mass index, smoking, disease duration, disease activity scores, and self-reported RA flares were not associated with reporting that foods affect RA.
Conclusion
Nearly one-quarter of RA subjects with longstanding disease reported an effect of diet on their RA symptoms.
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disease that generally requires use of disease-modifying anti-rheumatic drugs (DMARDs) to suppress joint inflammation. However, many RA patients ask if non-pharmacologic interventions could help to treat their RA. Patient interest in the effect of diet on RA has been noted for decades. Among a number of small clinical trials of dietary manipulation in RA, modest benefit has been noted for high-dose omega-3 fatty acids, fasting, vegetarian diet, and Mediterranean-type diet.1-3
In the 21st century, a lay trend has emerged focusing on “inflammatory” and “anti-inflammatory” foods. Some patient-oriented medical websites provide examples of such foods, along with advice to consume or avoid these foods in hopes of improving RA symptoms.4,5 In the clinical setting, patients often report to their providers that specific foods make their RA better or worse. We hypothesized that patient traits, including RA disease activity measures and use of biologic (b)DMARDs and non-biologic (nb)DMARDs, differ among patients who note that foods affect their RA compared to patients who do not. We surveyed RA patients to learn if specific foods affect their RA symptoms, and tested whether patient traits are associated with a change in RA symptoms from certain foods.
Patients and Methods
Study design and cohort
The Brigham RA Sequential Study (BRASS) is a single-center longitudinal RA registry that has enrolled >1400 subjects since 2003. All subjects were diagnosed with RA by a rheumatologist, and 97% of subjects meet ACR 1987 RA criteria. Rheumatoid factor (RF) and anti-cyclic citrullinated peptide (CCP) antibody are tested at enrollment. Patient-reported data collected every six months include demographics, RA medications, comorbidities, and self-reported disease activity scores (RA Disease Activity Index [RADAI] and modified Health Assessment Questionnaire [MDHAQ]). Physician-reported disease activity measures (Disease Activity Score in 28 Joints and CRP [DAS28-CRP3] and Clinical Disease Activity Index [CDAI]) are collected annually at a study visit. All elements of this study were approved by the Partners Healthcare Institutional Review Board.
Survey
From May 2015 to December 2015, we mailed a structured diet survey to a random sample of 300 subjects who were actively participating in the registry. For each of the 20 foods on the survey, subjects were asked: “For the following foods, please indicate whether it makes your RA unchanged, better, or worse.” Subjects were also given the option to indicate “I do not eat this food.” The 20 foods were included on the survey based on popular beliefs about being “inflammatory” (milk, cheese, red meat, tomato, eggplant, white potatoes, bell or hot peppers, diet soft drinks, beer),4-6 “anti-inflammatory” (fish, spinach, blueberries, strawberries, chocolate, red wine),4 or because we hypothesized that some subjects would report worsened RA symptoms after consuming them (soft drinks with sugar, caffeinated coffee, decaffeinated coffee, caffeinated tea, herbal or decaffeinated tea).7 Subjects were offered an opportunity to provide free-text entries about additional foods that make their RA better or worse. The survey included a question assessing food avoidance (never, sometimes, or often) due to worsened RA symptoms from food.
Subjects were also asked if four lifestyle/environmental factors improve their RA symptoms. These factors included the following: exercising regularly, good night's sleep, vitamin/mineral supplements, and warm room temperature. These questions were included as indicators of whether subjects perceive other lifestyle/environmental factors, aside from diet, to affect RA symptoms. Prior work supports beneficial effects of exercise in RA,8 and an association between poor sleep and RA symptoms.9 By contrast, little if any data exist about the impact of vitamin/mineral supplements or warm room temperature on RA symptoms. Subjects were also asked to report medical conditions that could potentially affect dietary choices (e.g. Crohn's disease, ulcerative colitis, acid reflux).
Completed surveys were mailed to the registry coordinator and were double-data entered into REDCap™ by two different research assistants.
Statistical analyses
The primary outcome was reporting that foods affect RA symptoms, which included three non-overlapping groups of subjects: those who reported that foods only improve RA, that foods only worsen RA, or that some foods improve RA and other foods worsen RA. Responses for each of the 20 specific foods, as well as free-text entries, were taken into account. For each of the 20 foods listed in the survey, we calculated the percentage of subjects reporting either worsened or improved RA symptoms due to that food.
Data on medications and disease activity scores were collected from the registry study visit closest to the date of diet survey completion. Many of the continuous variables were non-normally distributed; thus, for consistency, all continuous data were analyzed with non-parametric tests. Descriptive statistics summarized traits among all subjects, and then separately among those who reported that foods affect RA and those who did not. We tested for associations between subject traits and reporting that foods affect RA, using Fisher's exact test for categorical variables and Wilcoxon rank-sum test for continuous variables.
Statistical significance was defined as two-sided p<0.05. Analyses were performed using SAS v9.4 (Cary, N.C.).
Results
Characteristics of the 217 subjects who completed the survey (72.3% response rate) are presented in Table 1. Subjects had longstanding RA, with median disease duration of 17.0 years (IQR 9.0-27.0). Methotrexate was used by 54.8%, either as monotherapy or combination therapy. The use of a bDMARD was common, including TNF inhibitors (43.3%), abatacept (8.3%), rituximab (1.4%), tocilizumab (3.2%), and tofacitinib (1.8%). One-fourth of subjects were taking corticosteroids, with a median prednisone dose of 5 mg daily (IQR 4-10). Among 8.3% of subjects, either no RA medications were used or only non-steroidal anti-inflammatory drugs (NSAIDs) were used. Although half of subjects reported having a flare in the past six months, disease activity was low overall with median DAS28-CRP3 score of 2.1 (IQR 1.6-3.0). The frequency of self-reported acid reflux and lactose intolerance was similar to published studies of these self-reported conditions in the general U.S. population.10,11
Table 1. Characteristics of 217 RA subjects within six months of completing the dietary survey.
| Characteristic | |
|---|---|
| Age, years | 65.0 (53.0-71.0) |
| Female | 83.0% |
| White | 94.9% |
| BMI, kg/m2* | 26.0 (22.2-31.0) |
| Some college education or greater | 84.8% |
| Smoking* | |
| Never | 56.4% |
| Past | 40.6% |
| Current | 3.0% |
| Seropositive (RF and/or anti-CCP)* | 72.3% |
| Duration of RA, years | 17.0 (9.0-27.0) |
| Current RA therapy | |
| No treatment or NSAIDs only | 8.3% |
| Corticosteroids# | 24.9% |
| nbDMARD only+ | 13.4% |
| Triple nbDMARD therapy++ | 0.9% |
| Methotrexate mono- or combination therapy | 54.8% |
| bDMARD^ | 58.1% |
| ≥1 self-reported flare in past 6 mo. | 51.2% |
| Disease activity scores* | |
| DAS28-CRP3 | 2.1 (1.6-3.0) |
| CDAI | 6.0 (2.5-11.5) |
| MDHAQ | 0.4 (0.1-0.8) |
| RADAI | 2.2 (1.0-4.1) |
| Self-reported medical conditions* | |
| Coronary artery disease** | 5.5% |
| High blood pressure | 6.0% |
| High cholesterol | 6.0% |
| Type 2 diabetes | 0.5% |
| Crohn's or ulcerative colitis | 3.3% |
| Irritable bowel syndrome | 5.2% |
| Celiac or gluten sensitivity | 3.3% |
| Acid reflux or GERD | 33.5% |
| Lactose intolerance | 13.1% |
| Food allergy | 11.5% |
Presented as median (IQR) or %
Data missing for BMI (n=25), smoking (n=15), seropositive (n=29), DAS28-CRP3 (n=21), CDAI (n=15), MDHAQ (n=15), RADAI (n=15), Crohn's or ulcerative colitis (n=3), irritable bowel syndrome (n=5), celiac or gluten sensitivity (n=5), acid reflux or GERD (n=2), lactose intolerance (n=3), food allergy (n=9)
Includes corticosteroid monotherapy and combination therapy with DMARDs
Includes methotrexate, leflunomide, sulfasalazine, hydroxychloroquine. This category includes subjects taking one nbDMARD only
Triple therapy: methotrexate plus sulfasalazine plus hydroxychloroquine
Includes TNF inhibitors, abatacept, rituximab, tocilizumab, tofacitinib as monotherapy or combination therapy
Patient-reported history of myocardial infarction, coronary angioplasty, or coronary artery bypass grafting
The vast majority of subjects reported that exercising regularly (83.7%) and getting a good night's sleep (86.5%) improved RA symptoms. Warm room temperature (35.9%) and vitamin/mineral supplements (34.0%) were less often reported to improve RA symptoms.
Impact of foods on RA symptoms
At least one food was reported to affect RA symptoms in 24.0% of subjects. In 10.1% of subjects, some foods improved and some foods worsened RA symptoms. Foods only worsened RA in 9.2%, and foods only improved RA only in 4.6%. Additionally, 24.3% of all subjects reported avoiding foods (16.2% sometimes, 8.1% often) because they worsen their RA.
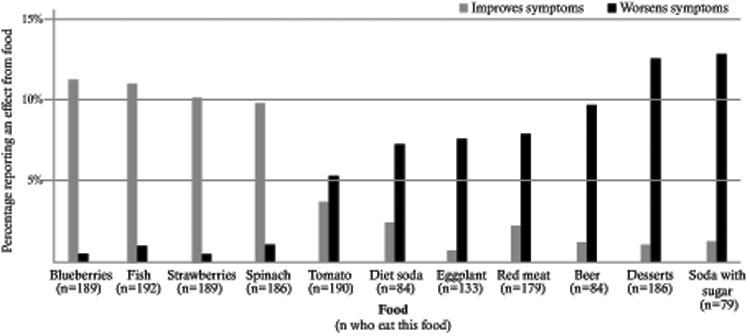
Among subjects who reported eating the specific foods listed, blueberries (11.1%) and fish (10.9%) were most often noted to improve RA symptoms (Figure 1). Soda with sugar (12.7%) and desserts (12.4%) were most frequently noted to worsen RA symptoms among subjects who consumed them. Caffeinated coffee and caffeinated tea were each reported to affect RA in less than five percent of subjects.
Figure 1. Specific foods that affect subjects' RA symptoms, displayed as the percentage of subjects who eat the food.
Associations between subject characteristics and reporting that foods affect RA
Subjects who reported that foods affect RA were younger than those who did not (median age 58.5 vs. 66.0 years, p=0.02) (Table 2). Sex, BMI, smoking status, seropositivity, duration of RA, and use of corticosteroids, nbDMARDs, and bDMARDs did not differ between those who reported that foods affect RA, and those who did not. Clinician-reported disease activity scores, patient-reported disease activity scores, and self-reported flares also did not differ between groups, nor did self-reported medical conditions that might affect diet (e.g., celiac disease/gluten sensitivity, irritable bowel syndrome).
Table 2. Comparison of subjects who report that specific foods affect their RA symptoms, and those who do not.
| Foods affect RA symptoms n=52 | Foods do not affect RA symptoms n=165 | p value | |
|---|---|---|---|
| Age, years | 58.5 (51.0-68.5) | 66.0 (54.0-72.0) | 0.02 |
| Female | 90.4% | 80.6% | 0.14 |
| White | 96.2% | 94.6% | 0.99 |
| BMI, kg/m2* | 25.2 (21.5-31.8) | 26.3 (22.3-30.9) | 0.55 |
| Some college education or greater | 82.7% | 85.5% | 0.66 |
| Smoking* | 0.41 | ||
| Never | 62.0% | 54.6% | |
| Past | 38.0% | 41.5% | |
| Current | 0% | 4.0% | |
| Seropositive (RF and/or anti-CCP)* | 65.1% | 74.5% | 0.25 |
| Duration of RA, years | 16.5 (8.5-22.0) | 17.0 (9.0-29.0) | 0.46 |
| Current RA therapy | |||
| Corticosteroids# | 26.9% | 24.2% | 0.72 |
| nbDMARD only+ | 7.7% | 15.2% | 0.24 |
| Methotrexate mono- or combination therapy | 48.1% | 57.0% | 0.27 |
| bDMARD^ | 65.4% | 55.8% | 0.26 |
| Disease activity scores* | |||
| DAS28-CRP3 | 2.0 (1.5-3.2) | 2.1 (1.6-3.0) | 0.68 |
| CDAI | 5.5 (2.0-12.0) | 6.8 (2.5-11.5) | 0.58 |
| MDHAQ | 0.5 (0.0-0.8) | 0.4 (0.1-0.8) | 0.89 |
| RADAI | 2.3 (1.0-4.1) | 2.1 (0.9-4.1) | 0.71 |
| ≥1 self-reported flares in past 6 mo. | 61.5% | 47.9% | 0.15 |
| Self-reported medical conditions* | |||
| Irritable bowel syndrome | 5.9% | 5.0% | 0.73 |
| Celiac or gluten sensitivity | 7.8% | 1.9% | 0.06 |
| Acid reflux or GERD | 28.9% | 35.0% | 0.50 |
| Lactose intolerance | 15.4% | 12.4% | 0.64 |
| Food allergy | 18.0% | 9.5% | 0.13 |
| Report that their RA symptoms are improved by* | |||
| Exercising regularly | 88.2% | 82.3% | 0.39 |
| Good night's sleep | 98.1% | 82.7% | <0.01 |
| Vitamin/mineral supplements | 55.8% | 26.9% | <0.01 |
| Warm room temperature | 52.9% | 30.4% | <0.01 |
Presented as median (IQR) or %
P values from Fisher's exact test or Wilcoxon rank-sum test
Data missing for BMI (n=25), smoking (n=15), seropositive (n=29), DAS28-CRP3 (n=21), CDAI (n=15), MDHAQ (n=15), RADAI (n=15), irritable bowel syndrome (n=5), celiac or gluten sensitivity (n=5), acid reflux or GERD (n=2), lactose intolerance (n=3), food allergy (n=9), exercise (n=5), sleep (n=2), vitamin/mineral (n=5), room temperature (n=3)
Includes corticosteroid monotherapy and combination therapy with DMARDs
Includes methotrexate, leflunomide, sulfasalazine, hydroxychloroquine. This category includes subjects taking one nbDMARD only
Includes TNF inhibitors, abatacept, rituximab, tocilizumab, tofacitinib as monotherapy or combination therapy
Participants who reported that a good night's sleep (p<0.01), warm room temperature (p<0.01), and vitamin/mineral supplements (p<0.01) improve RA symptoms were more likely to report that foods affect RA.
Discussion
We examined a sample of 217 RA patients in an RA registry to learn how foods affect their RA symptoms. Nearly one-quarter of RA subjects with longstanding disease reported that foods impacted their RA symptoms, either making RA better, worse, or better with some foods and worse with other foods. This group reporting an effect on symptoms was younger (though the median age was still >50 years), and was also more likely to report that other lifestyle/environmental factors improve their RA. Other RA characteristics, including medications, disease duration, and disease activity scores did not differ based on reporting that foods affect RA.
One similar survey on this topic was conducted from 1985-1990 among 704 private practice RA patients.12 In that cohort, specific foods affected RA symptoms in 27.6% of subjects. Foods only worsened RA in 10.7% of respondents, only improved RA in 5.5%, and some foods worsened while other foods improved RA in 9.8%. Similar to the present study, subjects who reported that foods affect RA symptoms were younger, and other traits did not differ between individuals who reported that foods affect RA and those who did not. Our study additionally tested for differences by medication use, self-reported flares, clinician- or patient-reported disease activity measures, or beliefs about other lifestyle factors.
Subgroups of RA patients may differ in whether foods affect RA symptoms. We hypothesized that subjects using bDMARDs would be less likely to report that foods affect RA, due to the potent effect of these medications. However, we did not detect a difference in responses based on use of bDMARDs, nor based on use of nbDMARDs or corticosteroids. The literature is conflicting on whether caffeine leads to decreased efficacy of methotrexate via inhibitory effects on extracellular adenosine.7,13 Among the 54.8% of subjects using methotrexate in our study, none reported that caffeinated coffee or tea made their RA worse (data not shown). In the era of potent DMARD therapy, it is interesting that a similar percentage of RA subjects report that diet impacts their RA compared to results from 25 years ago when NSAIDs, gold, corticosteroids, and hydroxychloroquine were among the mainstays of therapy.
A sizeable percentage of RA patients in this longitudinal registry reported that foods affect their RA symptoms. While many of the foods included in the diet survey are popularized as “inflammatory” or “anti-inflammatory,” the effect of many of these foods on inflammation has not been formally studied in RA, to our knowledge. Our study did not test whether specific foods affect RA disease activity, and we did not find a cross-sectional association between RA disease activity scores and self-reported change in RA symptoms from food. It is possible that certain foods on our survey do have anti-inflammatory effects in RA; for example, a recent randomized trial in juvenile idiopathic arthritis tested the effect of etanercept, etanercept plus daily blueberry juice, and etanercept plus placebo juice on disease activity and circulating interleukin (IL)-1 levels.14 At six months, the etanercept plus blueberry juice group had reduced IL-1 levels and a significantly higher percentage of subjects achieved ACR20, 50, and 70 compared to the other two groups. However, we are unable to draw conclusions about the effect of blueberries on RA disease activity in this survey study.
Additionally, we uncovered that approximately one-third of subjects feel vitamin/mineral supplements and warm room temperature improve RA symptoms. These findings have not been investigated or supported by the literature to date. Our study indicates that there is a substantial amount of patient interest in diet and RA symptoms, and highlights the need for prospective dietary studies before RA-specific recommendations can be made.
The present study was cross-sectional, and assessed self-reported impact of only 20 specific foods. We were thus unable to assess dietary patterns in relation to RA symptoms or disease activity scores. Subjects were participants in a single-center RA registry at a large, academic medical center, were highly educated, and predominantly White; therefore, our findings may not generalize to other RA populations. Prospective studies of specific foods and dietary patterns in relationship to disease activity scores are needed, especially in the era of potent DMARD therapy.
In conclusion, we found that 24.0% of subjects in a prospective, longitudinal RA registry reported that foods affect their RA symptoms, and 24.3% avoid foods due to worsening of their RA. Among a list of 20 specific foods, blueberries and spinach were most often noted to improve RA, while soda with sugar and desserts were most commonly reported to worsen RA. While we cannot draw strong conclusions based on this survey, past work has shown that greater consumption of sugar-sweetened beverages is associated with increased risk for developing RA.15 A potential link between sugar consumption and inflammation in rheumatoid arthritis warrants further study.
Significance and Innovations.
24% of RA subjects with longstanding RA noted that specific foods affect their RA symptoms. Self-reported change in RA symptoms did not differ based on medication use or disease activity scores.
Younger age and reporting that other lifestyle factors (sleep, room temperature, vitamin/mineral supplements) improve RA symptoms were associated with changes in RA symptoms from foods.
Among a list of 20 pre-specified foods, many of which have been popularized in the lay press as “inflammatory” or “anti-inflammatory,” blueberries and spinach were most often reported to improve RA symptoms, while soda with sugar and desserts were most often reported to worsen RA symptoms among subjects who reported eating those foods.
Acknowledgments
Financial support: Dr. Tedeschi's work on this project was supported by NIH-L30AR070514. The Brigham RA Sequential Study receives funding from UCB, Crescendo Biosciences, Bristol-Myers Squibb, Amgen, DxTerity. Drs. Weinblatt and Shadick receive salary support from research grants to their institution from Bristol-Myers Squibb, UCB, dXterity, Crescendo Bioscience, Amgen. Dr. Solomon's work on this project was supported by NIH-K24AR055989 and salary support from research grants to his institution from Astra Zeneca, Bristol-Myers Squibb, Amgen, Lilly, Pfizer, Genentech.
References
- 1.Panush RS, Carter RL, Katz P, Kowsari B, Longley S, Finnie S. Diet therapy for rheumatoid arthritis. Arthritis and Rheumatism. 1983;26:462–71. doi: 10.1002/art.1780260403. [DOI] [PubMed] [Google Scholar]
- 2.Kremer JM, Lawrence DA, Petrillo GF, et al. Effects of high-dose fish oil on rheumatoid arthritis after stopping nonsteroidal antiinflammatory drugs. Clinical and immune correlates. Arthritis and Rheumatism. 1995;38:1107–14. doi: 10.1002/art.1780380813. [DOI] [PubMed] [Google Scholar]
- 3.Tedeschi SK, Costenbader KH. Is there a role for diet in the therapy of rheumatoid arthritis? Current Rheumatology Reports. 2016;18:23. doi: 10.1007/s11926-016-0575-y. [DOI] [PubMed] [Google Scholar]
- 4.Arthritis Foundation. Anti-Inflammatory Diet. [Accessed May 29, 2015]; at http://www.arthritis.org/living-with-arthritis/arthritis-diet/anti-inflammatory/anti-inflammatory-diet.php.
- 5.Arthritis Foundation. 8 Food Ingredients That Can Cause Inflammation. [Accessed July 29, 2016];2016 at http://www.arthritis.org/living-with-arthritis/arthritis-diet/foods-to-avoid-limit/food-ingredients-and-inflammation.php.
- 6.Cleveland Clinic. How an Anti-Inflammatory Diet Can Relieve Pain as You Age. [Accessed July 15, 2016];2016 at https://health.clevelandclinic.org/2015/11/anti-inflammatory-diet-can-relieve-pain-age/
- 7.Nesher G, Mates M, Zevin S. Effect of caffeine consumption on efficacy of methotrexate in rheumatoid arthritis. Arthritis and Rheumatism. 2003;48:571–2. doi: 10.1002/art.10766. [DOI] [PubMed] [Google Scholar]
- 8.van der Giesen FJ, van Lankveld W, Hopman-Rock M, et al. Exploring the public health impact of an intensive exercise program for patients with rheumatoid arthritis: a dissemination and implementation study. Arthritis Care & Research. 2010;62:865–72. doi: 10.1002/acr.20138. [DOI] [PubMed] [Google Scholar]
- 9.Lee YC, Chibnik LB, Lu B, et al. The relationship between disease activity, sleep, psychiatric distress and pain sensitivity in rheumatoid arthritis: a cross-sectional study. Arthritis Research & Therapy. 2009;11:R160. doi: 10.1186/ar2842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cohen E, Bolus R, Khanna D, et al. GERD symptoms in the general population: prevalence and severity versus care-seeking patients. Dig Dis Sci. 2014;59:2488–96. doi: 10.1007/s10620-014-3181-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Keith JN, Nicholls J, Reed A, Kafer K, Miller GD. The prevalence of self-reported lactose intolerance and the consumption of dairy foods among African American adults are less than expected. J Natl Med Assoc. 2011;103:36–45. doi: 10.1016/s0027-9684(15)30241-8. [DOI] [PubMed] [Google Scholar]
- 12.Tanner SB, Callahan LF, Panush RS, Pincus T. Dietary and allergic associations with rheumatoid arthritis. Arthritis and Rheumatism. 1990;3:189–95. [Google Scholar]
- 13.Benito-Garcia E, Heller JE, Chibnik LB, et al. Dietary caffeine intake does not affect methotrexate efficacy in patients with rheumatoid arthritis. The Journal of Rheumatology. 2006;33:1275–81. [PubMed] [Google Scholar]
- 14.Zhong Y, Wang Y, Guo J, Chu H, Gao Y, Pang L. Blueberry improves the therapeutic effect of etanercept on patients with juvenile idiopathic arthritis: Phase III study. Tohoku J Exp Med. 2015;237:183–91. doi: 10.1620/tjem.237.183. [DOI] [PubMed] [Google Scholar]
- 15.Hu Y, Costenbader KH, Gao X, et al. Sugar-sweetened soda consumption and risk of developing rheumatoid arthritis in women. The American Journal of Clinical Nutrition. 2014;100:959–67. doi: 10.3945/ajcn.114.086918. [DOI] [PMC free article] [PubMed] [Google Scholar]