

Abstract
Background:
Navicular injuries can result in persistent pain, posttraumatic osteoarthritis, and diminished performance and function.
Purpose:
To determine the epidemiology of navicular fracture in players participating in the National Football League (NFL) Scouting Combine and evaluate the impact of a navicular injury on the NFL draft position and NFL game play compared with matched controls.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data were collected on players who previously sustained a navicular injury and participated in the NFL Combine between 2009 and 2015. The epidemiology of navicular injury was determined through an evaluation of the number of injuries, surgeries, and collegiate games missed as well as the position played, a physical examination, the surgical technique, and imaging findings. Players with a previous navicular injury (2009-2013) were compared with a set of matched controls. NFL performance outcomes included the draft position, career length ≥2 years, and number of games played and started within the first 2 years.
Results:
Between 2009 and 2015, 14 of 2285 (0.6%) players were identified as having sustained a navicular injury. A total of 11 of 14 (79%) athletes had sustained an overt navicular fracture, while 3 of 14 (21%) were diagnosed with stress reactions on magnetic resonance imaging. Eight patients who sustained a navicular fracture underwent surgery. There was evidence of ipsilateral talonavicular arthritis in 75% of players with a navicular fracture versus only 60% in the uninjured foot (odds ratio, 1.3; P = .04). Fifty-seven percent of players with navicular injury (72.7% of fractures) were undrafted versus 30.9% in the control group (P = .001). Overall, 28.6% of players with navicular fracture played ≥2 years in the NFL compared with 69.6% in the control group (P = .02).
Conclusion:
A previous navicular fracture results in a greater risk of developing posttraumatic osteoarthritis. Although only a low prevalence of navicular injury in prospective NFL players was noted, players with these injuries had a greater probability of not being drafted and not competing in at least 2 NFL seasons when compared with matched controls without an injury history to the NFL Combine.
Keywords: navicular, National Football League, football (American), epidemiology
Tarsal navicular fractures are difficult to diagnose and can cause significant disability, especially in athletes.8,23,24 These fractures can occur both in the acute setting from trauma as well as in the chronic setting because of repetitive stress.9 Patients with navicular stress fracture usually present with tenderness directly over the “N-spot,” or the high point of the navicular.23 Many on-field sports activities, such as cutting, sprinting, and jumping, are known to exacerbate the symptoms of a navicular fracture.11 Necessary treatment for navicular injuries is frequently delayed, as these injuries are regularly misdiagnosed as tendinitis on initial clinical presentation.23 When left untreated, a navicular stress fracture can worsen and result in fracture propagation, displacement, resorption, and degenerative changes that may compromise outcomes.23,24
The osseous anatomy, kinematics, and blood supply of the tarsal navicular contribute to its characteristic injury patterns.13,19 The navicular is a pear-shaped bone located within the medial column of the foot13; it articulates distally with the 3 cuneiforms and proximally with the talar head.23 Aside from the considerable load placed on the medial column of the foot, there is approximately 37° of motion at the talonavicular joint, which accounts for about 80% of hindfoot motion.1,8 During foot strike, the navicular bone must absorb compressive stress from the first and second metatarsocuneiform joints and talar head as well as a distractive load from the contraction of the posterior tibialis at its attachment on the medial tuberosity.11 A watershed area of the navicular blood supply is located in the center of the bone, predisposing this region to stress fractures and nonunion.9
The classification of Saxena et al,25 ranging from type 1 to type 3 for navicular stress fractures, was developed to describe injury severity on computed tomography (CT). A type 1 fracture is a dorsal cortical break, a type 2 injury is a dorsal fracture that propagates into the navicular body, and a type 3 fracture penetrates a second (often plantar) cortex. Saxena and Fullem24 have shown that the time for return to activity after a navicular stress fracture is approximately 4 months, independent of the treatment choice. Type 1 injuries can usually be managed nonoperatively with nonweightbearing, while type 2 and 3 injuries are usually treated via internal fixation.24
The annual National Football League (NFL) Scouting Combine, a week-long program made up of a variety of rigorous physical examinations and exercises, allows professional American football teams to evaluate the best collegiate talent entering the NFL.3,15 The combine is held directly before the NFL draft, during which the collegiate football players can be chosen by NFL franchises to join their respective team. The NFL Combine’s physical examinations and collection of medical history information help teams to determine if a player’s injury history could possibly be detrimental to his NFL performance or career longevity, which ultimately affects the player’s rank during the draft selection process. To date, no study has evaluated the effect of sustaining a navicular fracture on the NFL draft status or future NFL performance and career longevity of an athlete.
The purposes of this study were to (1) determine the epidemiology of navicular fracture in players participating in the NFL Scouting Combine and (2) evaluate the impact of navicular injury on the NFL draft position and NFL game play as compared to matched controls.
Methods
Approval for this study was obtained from the institutional review board and the NFL Players Association and the NFL Physicians Society Research Committee. The charts of all players who participated in the NFL Combine from 2009 to 2015 were reviewed to identify those with a self-reported history or radiographs indicating a previous navicular injury. Epidemiological data were recorded for all players with a history of navicular injury from 2009 to 2015, including the position played, number of college games missed, and treatment methods used. Imaging studies, including plain radiography, magnetic resonance imaging (MRI), and CT, were analyzed for the fracture type using the classification described by Saxena et al25 to determine the presence of residual nonunion or delayed union in the fracture group. Imaging was also performed to determine the foot type (pes cavus or pes planus) as well as the presence of any arthritis in either the affected or contralateral foot, as bilateral imaging was available for 13 of 14 athletes with a history of navicular injury, although this is not established NFL Combine protocol. The presence of talonavicular arthritis on the affected and noninjured contralateral foot was determined based on any sign of irregularity on plain radiographs. Arthritis was only graded for presence, not severity.
Performance data were collected from all players with a history of navicular injury who participated in the NFL Combine between 2009 and 2013. NFL performance outcomes were evaluated through an analysis of the draft position, career length ≥2 years, and number of games played and games started within the first 2 years.5,6,26 Players who participated in the 2014 and 2015 NFL Combines were excluded from the outcomes analysis because they were unable to compete in at least 2 NFL seasons at the time of data collection. NFL performance outcomes were then compared to a control group composed of players who missed <2 games in college, played the same position, and did not undergo previous surgery or have a documented injury (N = 1028). All NFL performance data were obtained from STATS.com.
Statistical Analysis
Odds ratios were calculated using logistic regression to assess the risk of sustaining a navicular injury by each playing position. Two-sample, 2-tailed t tests were completed to assess differences in outcomes between positions (offensive vs defensive players), treatment groups (nonoperative vs operative), cases and controls, radiographic outcomes (healed fracture vs nonunion), and radiographic injury classifications.
Results
A total of 2285 football players participated in the NFL Scouting Combine between 2009 and 2015. There were 15 navicular injuries identified in 14 athletes, demonstrating an incidence of 0.6% of collegiate football players participating in the combine during this time frame. Eleven athletes sustained an overt navicular fracture (1 player had bilateral fractures), while 3 were diagnosed with a stress reaction on MRI. Athletes with a stress reaction were managed nonoperatively (ranging from 2-3 days of rest to 6 weeks of boot immobilization), and follow-up imaging in each athlete showed a healed navicular joint with no evidence of recurrent navicular stress fractures. Eight of the 11 patients (72.7%) who sustained a navicular fracture underwent surgical management to treat the fracture. In contrast, 3 of the 11 (27.3%) were managed nonoperatively. The athlete with bilateral fractures was managed nonoperatively for the initial fracture and underwent surgical management for the contralateral fracture. Although the exact method of nonoperative management was not detailed through the available data, a standard functional boot for immobilization in combination with a nonweightbearing protocol is usually recommended. Overall, 3 of the 8 players treated surgically (37.5%) had 1 screw, 4 (50.0%) had 2 screws, and 1 (12.5%) had 3 screws implanted for surgical repair. More than half of all radiographs demonstrated lateral to medial screw positioning (n = 5 [62.5%]) (Table 1). Two patients treated surgically required revision surgery, including 1 for nonunion (Figure 1) and 1 for a refracture around the original screw (Figure 2).
TABLE 1.
Clinical Characteristics and Radiographic Findings of Navicular Fracture (n = 11)a
| n (%) | |
|---|---|
| Interval since original injury | |
| <6 mo | 2 (18.2) |
| 6-12 mo | 2 (18.2) |
| 1-3 y | 3 (27.3) |
| >3 y | 4 (36.4) |
| Surgical management | 8 (72.7) |
| <30 d of injury | 2 (25.0) |
| 30-90 d of injury | 4 (50.0) |
| >90 d of injury | 2 (25.0) |
| No. of screws | |
| 1 | 3 (37.5) |
| 2 | 4 (50.0) |
| 3 | 1 (12.5) |
| Direction of screws | |
| Lateral to medial | 5 (62.5) |
| Medial to lateral | 2 (25.0) |
| Dorsal to plantar and lateral to medial | 1 (12.5) |
| Repeat surgeryb | 2 (25.0) |
aOne athlete had 2 independent navicular fractures involving the right and left foot; the surgical side was used when describing management.
bOne player underwent revision surgery for nonunion, while 1 other player underwent revision surgery for a refracture.
Figure 1.
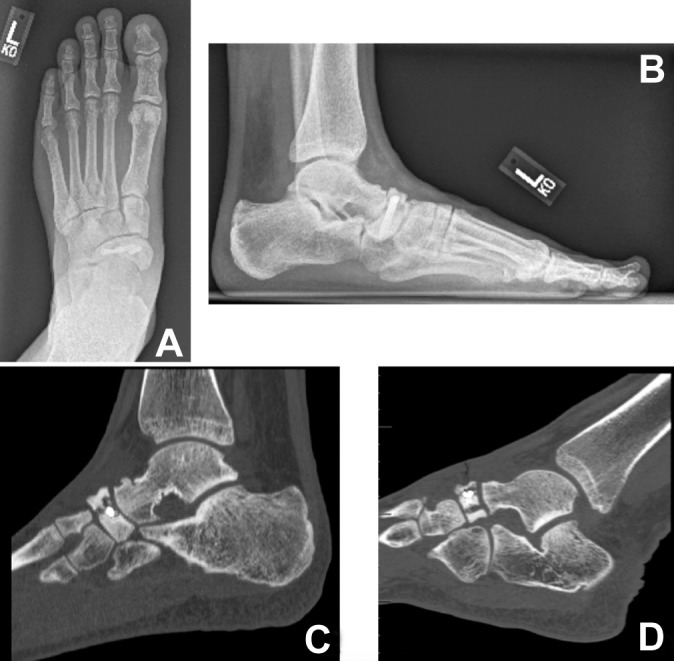
(A) Anteroposterior and (B) lateral radiographs of a player’s left foot after screw fixation of a navicular fracture. Two screws were placed from lateral to medial. Evidence of nonunion can still be seen on the (B) lateral radiograph along with (C, D) sagittal cuts of a computed tomography scan.
Figure 2.

(A) Anteroposterior radiograph of a player’s right foot after 2 screws were placed lateral to medial. (B) The coronal computed tomography scan demonstrates that the fracture is still present. The (C) coronal and (D) axial cuts of the scan, 2 months later, demonstrate a refracture around the screws.
An analysis of radiographic imaging revealed 9 healed (Figure 3) or partially healed (defined as residual nonunion or delayed union of the fracture site) fractures, 2 nonunions, and 1 refracture. Of the 10 players who had adequate imaging to determine classifications (2 were excluded), the breakdown by fracture type included 1 (10%) type 1 fracture, 2 (20%) type 2 fractures, and 7 (70%) type 3 fractures. There was no difference (P = .463) with regard to the draft status when comparing fracture types. There was evidence of ipsilateral talonavicular arthritis in 75% of the players with a history of navicular fracture as compared to only 60% in their contralateral uninjured foot (odds ratio, 1.3; P = .04) (Table 2).
Figure 3.

(A) Anteroposterior and (B) lateral radiographs of a player’s left foot after 2 screws were placed lateral to medial. The (C) coronal and (D) sagittal cuts of a computed tomography scan demonstrate a well-healed fracture.
TABLE 2.
Radiographic Findings at the NFL Combine (n = 12)a
| n (%) | |
|---|---|
| Status at NFL Combine | |
| Healed | 5 (36.4) |
| Partially healedb | 4 (36.4) |
| Nonunion or refracture | 3 (27.3) |
| Classification of navicular injury (n =10)c | |
| Type 1 | 1 (10.0) |
| Type 2 | 2 (20.0) |
| Type 3 | 7 (70.0) |
| Other radiographic findings | |
| Arthritis of injured foot | 9 (75.0) |
| Contralateral osteoarthritisd | 6/10 (60.0) |
| Pes cavus | 2 (16.7) |
| Pes planus | 2 (16.7) |
aOne athlete had 2 independent navicular fractures involving the right and left foot. NFL, National Football League.
bDefined as residual nonunion or delayed union of the fracture site.
cClassification could not be determined in 2 players from available imaging.
dOne player did not have contralateral radiographs, and 1 player did not have an uninjured contralateral side for evaluation.
Of the 14 athletes who previously sustained a navicular injury, 8 were offensive and 6 were defensive players. Defensive back was the most common player position represented among athletes participating in the NFL Combine with a history of navicular injury (odds ratio, 3.0; P = .03), although only 3 defensive backs had a previous navicular injury. In contrast, a significantly greater percentage of offensive players (n = 7 [87.5%]) went undrafted after sustaining a navicular fracture as compared to defensive players (n = 1 [16.6%]) (P = .002). Overall draft results and comparisons between offensive and defensive players are seen in Table 3.
TABLE 3.
Draft Results of NFL Combine Players With Navicular Injury (2009-2015)a
| Navicular Injury, n (%) | Fracture, n (%) | Stress Reaction, n (%) | Total Missed Games, Mean ± SD | Navicular Missed Games, Mean ± SD | No College Missed Games, n (%) | Surgery, n (%) | Undrafted, n (%) | Overall Pick, Mean ± SD | |
|---|---|---|---|---|---|---|---|---|---|
| All (N = 2285) | 14 (0.6) | 11 (78.6) | 3 (21.4) | 6.1 ± 4.8 | 3.6 ± 4.4 | 6 (42.9) | 8 (57.1) | 8 (57.1) | 105.0 ± 55.4 |
| Offense (n = 1175) | 8 (0.7) | 8 (100.0) | 0 (0.0) | 4.9 ± 4.6 | 4.1 ± 4.7 | 3 (37.5) | 7 (87.5) | 7 (87.5) | 107 ± – |
| Defense (n = 1028) | 6 (0.6) | 3 (50.0) | 3 (50.0) | 7.7 ± 5.0 | 2.8 ± 4.4 | 3 (50.0) | 1 (16.7) | 1 (16.6) | 104.6 ± 61.9 |
aOne athlete had 2 independent navicular fractures involving the right and left foot. The percentage of undrafted was significantly greater for offensive players versus defensive players (P = .002). NFL, National Football League.
NFL performance outcomes for the study players were then evaluated based on the treatment type and were compared to matched controls. The 11 players with a history of navicular fracture had an increased likelihood of being undrafted (n = 8 [72.7%]) compared to the 1028 matched controls (n = 318 [30.9%]) (P = .001). There was no difference (P = .784) in the position drafted for the remaining 3 players who were drafted with a diagnosis of a stress reaction on MRI (100.0) and the control group (112.3). When analyzing players divided into nonoperative and operative treatment groups, the 8 who underwent surgery were found to be more likely to remain undrafted compared to both the nonoperative group (n = 7 [87.5%] vs n = 1 [33.3%], respectively; P = .04) and the control group (n = 7 [87.5%] vs n = 318 [30.9%], respectively; P = .002) (Table 4).
TABLE 4.
Draft Results of NFL Combine Players With Navicular Fracture (n = 11) by Operative Versus Nonoperative Managementa
| All, n (%) | Navicular Missed Games, Mean ± SD | Undrafted, n (%) | Overall Pick, Mean ± SD | |
|---|---|---|---|---|
| Players with a previous navicular fracture | 11 | 4.5 ± 4.5 | 8 (72.7) | 100.0 ± 11.5 |
| Operative management | 8 (73.0) | 4.1 ± 4.7 | 7 (87.5) | 107.0 ± 0.0 |
| Nonoperative management | 3 (27.0) | 5.6 ± 4.9 | 1 (33.3) | 97.0 ± 14.1 |
| Control | 1028 | — | 318 (30.9) | 112.3 ± 69.1 |
aOperative management was associated with an increased percentage of undrafted athletes compared to nonoperative treatment (P = .04).
After excluding players from the 2014 and 2015 NFL Combines, there remained 7 players with a history of navicular fracture available for the analysis of NFL performance outcomes in their first 2 seasons. The total number of NFL games played and games started in the first 2 seasons of all players’ NFL careers were recorded for these 7 players (Table 5). In all athletes, players with a navicular fracture were more likely to remain undrafted compared to controls (P < .001) and less likely to compete in the NFL for at least 2 years (28.6% vs 69.6%, respectively; P < .01). Similarly, players with navicular fracture played in fewer games in their first 2 NFL seasons compared to controls, although this difference was not statistically significant (P = .07).
TABLE 5.
Impact of Navicular Fracture on NFL Playa
| Players With Navicular Fracture | Controls | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All, n (%) | Undrafted, n (%) | Overall Pick, Mean ± SD | ≥2 y, n (%) | GP, Mean ± SD | GS, Mean ± SD | All, n | Undrafted, n (%) | Overall Pick, Mean ± SD | ≥2 y, n (%) | GP, Mean ± SD | GS, Mean ± SD | |
| Offense | 6 | 5 (83.3) | 107.0 ± 0.0 | 2 | 15.0 ± 9.9 | 3.0 ± 2.8 | 346 | 118 (34.1) | 114.5 ± 68.3 | 220 (63.6) | 22.3 ± 7.9 | 10.5 ± 10.2 |
| OL | 1 (16.7) | 1 (100.0) | — | 0 (0.0) | — | — | 111 | 30 (27.0) | 103.2 ± 67.1 | 71 (64.0) | 21.1 ± 8.3 | 14.2 ± 11.2 |
| RB | 2 (33.3) | 2 (100.0) | — | 0 (0.0) | — | — | 49 | 17 (34.9) | 127.7 ± 67.0 | 34 (69.4) | 22.4 ± 6.2 | 5.7 ± 8.0 |
| TE | 2 (33.3) | 2 (100.0) | — | 1 (50.0) | 22.0 ± 0.0 | 5.0 ± 0.0 | 32 | 8 (25.0) | 140.0 ± 59.4 | 26 (81.3) | 24.6 ± 7.3 | 9.0 ± 6.7 |
| WR | 1 (16.7) | 0 (0.0) | 107.0 ± 0.0 | 1 (100.0) | 8.0 ± 0.0 | 1.0 ± 0.0 | 106 | 41 (38.7) | 113.0 ± 69.7 | 70 (66.0) | 23.7 ± 7.4 | 9.0 ± 9.1 |
| Defense | 1 | 1 (100.0) | — | 0 (0.0) | — | — | 355 | 81 (22.8) | 108.6 ± 70.1 | 268 (75.5) | 24.2 ± 7.6 | 10.5 ± 10.5 |
| LB | 1 (100.0) | 1 (100.0) | — | 0 (0.0) | — | — | 74 | 17 (23.0) | 115.6 ± 68.6 | 54 (73.0) | 25.1 ± 7.2 | 12.3 ± 11.9 |
| All players | 7 (100.0) | 6 (85.7) | 107.0 ± 0.0 | 2 (28.6) | 15.0 ± 9.9 | 3.0 ± 2.8 | 701 | 199 (28.4) | 111.3 ± 69.3 | 488 (69.6) | 23.3 ± 7.8 | 10.5 ± 10.4 |
aExcludes athletes who attended the National Football League (NFL) Combine in 2014 and 2015. ≥2 y, played in the NFL for a minimum of 2 years; GP, total games played in the first and second years of the NFL; GS, total number of games started in the first and second years of the NFL; LB, linebacker; OL, offensive lineman; RB, running back; TE, tight end; WR, wide receiver.
Discussion
Several studies have evaluated the rate of return to sport and time until return to sport after a navicular injury.24,27 This study, however, represents the first evaluation, to our knowledge, of the impact that a navicular injury can have on the careers of elite football players. In this series, 57% of players who sustained a navicular injury (72.7% of fractures) went undrafted as compared to only 30.9% in the control group (P = .001). In addition, only 28.6% of players with a history of navicular fracture played at least 2 years in the NFL after the draft versus 69.6% in the control group (P = .02). Radiographic analysis also revealed a 15% higher chance of having demonstrable degenerative changes in the talonavicular joint if an athlete had a history of navicular fracture (seen in the injured foot of 75% of such players vs 60% in the contralateral uninjured foot; odds ratio, 1.3; P = .04). Although the severity of arthritic changes was not assessed, this finding suggests that such injuries impose substantial long-term implications regarding progressive midfoot disease. These results underline the significant detrimental impact that navicular injury may have on the ability to perform at the professional level as well as the durability of any athlete competing at an elite level.
In 2010, Torg et al27 concluded via a meta-analysis that nonweightbearing cast immobilization for either a complete or incomplete nondisplaced navicular stress fracture had a 96% success rate, with an average time to return to sport of 4.9 months as well as no difference in the return-to-sport time between the surgical and nonsurgical populations. Similar to the study by Torg et al, Saxena and Fullem24 found no difference in clinical outcomes between patients with navicular fractures who were treated nonoperatively (n = 19) or operatively (n = 22). Nonetheless, surgery was advocated for all patients with a type 2 or 3 fracture. Return to activity in this series was similar for both patient populations, at 3.9 months on average. Fifteen of the 16 competitive athletes returned to full competition, although the study was not limited to professional athletes. Our series, on the other hand, identified an increased likelihood of being undrafted by the NFL after surgical treatment of a navicular fracture as compared to nonoperative management. However, the validity of this finding is difficult to evaluate, as the nonoperative group was made up of only 3 players and players may have undergone surgery because they initially failed nonoperative management or exhibited more severe fracture patterns.
Mallee et al17 reviewed 200 cases of navicular stress fractures, with 98.5% of these injuries seen in athletes. Patients managed nonoperatively returned to sport 22 weeks after the injury, while a return of 16 weeks was seen in those who underwent surgical intervention.17 Potter et al21 reported on the long-term outcomes of navicular fractures and confirmed no difference in functional outcomes or pain scores between surgical and nonsurgical management at an average 10-year follow-up. A review of the above studies led Ramadorai et al22 to conclude that “high-quality studies are needed to determine the optimal treatment of tarsal navicular stress fractures.”
Prior studies have demonstrated that a player’s durability, career length, and future injury risk may be partly determined by the injury history. A previous analysis of NFL Combine participants from 1987 to 2000 revealed that the average number of diagnoses per player was 2.45, with the average number of procedures being roughly 1 for every 2 players (0.53 per player).4 Brophy et al5 determined that a history of meniscectomy, but not anterior cruciate ligament reconstruction, shortened the career of an NFL player and that the combination of anterior cruciate ligament reconstruction and meniscectomy may be more detrimental to an athlete’s career than either surgery alone. Similarly, shoulder stabilization procedures have been shown to shorten the expected career of an NFL football player, in particular for linemen and linebackers.6 Larson et al16 found that an increased alpha angle of the femur is an independent predictor of future groin pain in NFL Combine participants. Furthermore, pre-existing lumbar spine disease results in a lower likelihood to be drafted by an NFL team and a shorter career length, but there was no decrease in performance for these athletes during their abbreviated careers.26 In our study, navicular fracture represented a small number of the total injury count reported at the NFL Combine (0.6%); however, athletes who sustained these injuries were twice as likely to remain undrafted and less than half as likely to be able to compete in at least 2 NFL seasons compared to matched controls. With the objective of providing better counsel, it may be pertinent to advise potential NFL athletes that a previous navicular injury is potentially detrimental to the durability of an NFL career as well as performance in the NFL.
Restoring the anatomic relationships surrounding the tarsal navicular is imperative to re-establishing normal gait mechanics after an injury.9 Foot pronation (heel strike cushioning) and supination (push-off) require normal talonavicular joint motion. The talonavicular joint also functions with the subtalar joint to allow for inversion and eversion of the hindfoot when on sloped surfaces.9 Previously described anatomic risk factors for a navicular stress fracture include a long second metatarsal, metatarsal adduction, and equinus contracture because they tend to increase stress across the midfoot and forefoot.10,14,20 It has also been theorized that patients with pes cavus have an increased risk of stress fractures because of stiffness and rigidity. Similar to our study, in which no singular foot characteristic was broadly associated with navicular stress fracture, other studies have not been able to demonstrate a direct causal relationship between any specific anatomic abnormality and the occurrence of this pathology.7,14,18 Another hypothesized risk factor is dynamic navicular motion, as in “navicular drop” (plantar) or “navicular drift” (medial).2,12 Navicular drop is a method to measure pronation and medial column function by calculating the perpendicular distance between the navicular tuberosity and the line between the calcaneus and first metatarsal. However, this study did not evaluate the role of navicular drop after a navicular fracture.
Lastly, this study does have several potential limitations. First, the number of players with a verified navicular injury on imaging was low (n = 14). However, we believe that the comparison to a large matched control group compensated for this limitation while also allowing for a relevant association between prior navicular injury and its effect on playing time in the NFL. Second, all data were compiled through a retrospective review of charts collected at the NFL Scouting Combine. As a result, some injuries may have been missed if they were not discovered at this event. However, each player is subject to multiple physical examinations with meticulous histories performed by multiple subspecialty-trained orthopaedic surgeons over the course of the NFL Combine; therefore, we suspect that this notably reduced the possibility of a missed injury. We found that the defensive back position was the most commonly played position among athletes who participated in the NFL Scouting Combine and who had a history of navicular injury. These defensive backs continued to perform at a level that warranted invitation to the NFL Combine, which likely means that they were able to recover sufficiently from this injury. It is possible, however, that other position players who sustain a navicular fracture do not recover from this injury sufficiently to perform at a level deserving of an invitation to the NFL Combine, and thus, we were unable to evaluate this group of collegiate athletes. In all, only players who were able to successfully recover and perform well enough to earn an invitation to the NFL Combine were evaluated, limiting our assessment of the risk of navicular fracture by position. Furthermore, the relatively limited number of patients in the navicular injury group could also have confounded the NFL performance outcomes analysis. Finally, competition at the NFL level is incredibly selective and dependent on many player characteristics; moreover, many players sustain a variety of injuries that span not only the foot but also other anatomic locations. As a result, it is difficult to draw definitive conclusions regarding the degree to which an athlete’s injury history affects his draft position, number of NFL games played or started, or overall career length. Ultimately, the draft position, along with the number of NFL games played and started during the initial portion of a player’s career, may be partially affected by the perception or expectation of a poor outcome by team physicians and trainers despite proper function and a lack of symptoms after an injury. Nonetheless, this study attempts to control for these variables through comparative use of a matched control group.
Conclusion
A previous navicular fracture results in a greater risk of developing posttraumatic osteoarthritis. Although only a low prevalence of navicular injury in prospective NFL players was noted, players who sustained navicular fracture in college had a greater probability of not being drafted and not competing in at least 2 NFL seasons when compared to matched controls without an injury history to the NFL Combine.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: C.W.D. has stock/stock options in CreOsso, Extremity Medical, and Wright Medical Technology; is a paid consultant for Extremity Medical and Wright Medical Technology; is a paid speaker or presenter for Extremity Medical and Wright Medical Technology; and receives royalties from Extremity Medical, Saunders/Mosby–Elsevier, Springer, and Wolters Kluwer Health. M.T.P. is a paid consultant for Arthrex and the Joint Restoration Foundation (AlloSource) and receives royalties from Arthrex and SLACK.
Ethical approval for this study was obtained from the Partners Human Research Committee (protocol 2015P002224/MGH).
References
- 1. Astion DJ, Deland JT, Otis JC, Kenneally S. Motion of the hindfoot after simulated arthrodesis. J Bone Joint Surg Am. 1997;79(2):241–246. [DOI] [PubMed] [Google Scholar]
- 2. Barton CJ, Kappel SL, Ahrendt P, Simonsen O, Rathleff MS. Dynamic navicular motion measured using a stretch sensor is different between walking and running, and between over-ground and treadmill conditions. J Foot Ankle Res. 2015;8:5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Berri DJ, Simmons R. Catching a draft: on the process of selecting quarterbacks in the National Football League amateur draft. J Product Anal. 2009;35(1):37–49. [Google Scholar]
- 4. Brophy RH, Barnes R, Rodeo SA, Warren RF. Prevalence of musculoskeletal disorders at the NFL Combine: trends from 1987 to 2000. Med Sci Sports Exerc. 2007;39(1):22–27. [DOI] [PubMed] [Google Scholar]
- 5. Brophy RH, Gill CS, Lyman S, Barnes RP, Rodeo SA, Warren RF. Effect of anterior cruciate ligament reconstruction and meniscectomy on length of career in National Football League athletes: a case control study. Am J Sports Med. 2009;37(11):2102–2107. [DOI] [PubMed] [Google Scholar]
- 6. Brophy RH, Gill CS, Lyman S, Barnes RP, Rodeo SA, Warren RF. Effect of shoulder stabilization on career length in National Football League athletes. Am J Sports Med. 2011;39(4):704–709. [DOI] [PubMed] [Google Scholar]
- 7. Burne SG, Mahoney CM, Forster BB, Koehle MS, Taunton JE, Khan KM. Tarsal navicular stress injury: long-term outcome and clinicoradiological correlation using both computed tomography and magnetic resonance imaging. Am J Sports Med. 2005;33(12):1875–1881. [DOI] [PubMed] [Google Scholar]
- 8. Coulibaly MO, Jones CB, Sietsema DL, Schildhauer TA. Results and complications of operative and non-operative navicular fracture treatment. Injury. 2015;46(8):1669–1677. [DOI] [PubMed] [Google Scholar]
- 9. DiGiovanni CW. Fractures of the navicular. Foot Ankle Clin. 2004;9(1):25–63. [DOI] [PubMed] [Google Scholar]
- 10. Fitch KD, Blackwell JB, Gilmour WN. Operation for non-union of stress fracture of the tarsal navicular. J Bone Joint Surg Br. 1989;71(1):105–110. [DOI] [PubMed] [Google Scholar]
- 11. Gross CE, Nunley JA. Navicular stress fractures. Foot Ankle Int. 2015;36(9):1117–1122. [DOI] [PubMed] [Google Scholar]
- 12. Hoffman SE, Peltz CD, Haladik JA, Divine G, Nurse MA, Bey MJ. Dynamic in-vivo assessment of navicular drop while running in barefoot, minimalist, and motion control footwear conditions. Gait Posture. 2015;41(3):825–829. [DOI] [PubMed] [Google Scholar]
- 13. Jones MH, Amendola AS. Navicular stress fractures. Clin Sports Med. 2006;25(1):151–158. [DOI] [PubMed] [Google Scholar]
- 14. Kitaoka HB, Luo ZP, An KN. Contact features of the talonavicular joint of the foot. Clin Orthop. 1996;(325):290–295. [DOI] [PubMed] [Google Scholar]
- 15. Kuzmits FE, Adams AJ. The NFL Combine: does it predict performance in the National Football League? J Strength Cond Res. 2008;22(6):1721–1727. [DOI] [PubMed] [Google Scholar]
- 16. Larson CM, Sikka RS, Sardelli MC, et al. Increasing alpha angle is predictive of athletic-related “hip” and “groin” pain in collegiate National Football League prospects. Arthrosc J Arthrosc Relat Surg. 2013;29(3):405–410. [DOI] [PubMed] [Google Scholar]
- 17. Mallee WH, Weel H, van Dijk CN, van Tulder MW, Kerkhoffs GM, Lin C-WC. Surgical versus conservative treatment for high-risk stress fractures of the lower leg (anterior tibial cortex, navicular and fifth metatarsal base): a systematic review. Br J Sports Med. 2015;49(6):370–376. [DOI] [PubMed] [Google Scholar]
- 18. McCormick JJ, Bray CC, Davis WH, Cohen BE, Jones CP, Anderson RB. Clinical and computed tomography evaluation of surgical outcomes in tarsal navicular stress fractures. Am J Sports Med. 2011;39(8):1741–1748. [DOI] [PubMed] [Google Scholar]
- 19. McInnis KC, Ramey LN. High-risk stress fractures: diagnosis and management. PM R. 2016;8(3 Suppl):S113–S124. [DOI] [PubMed] [Google Scholar]
- 20. Pavlov H, Torg JS, Freiberger RH. Tarsal navicular stress fractures: radiographic evaluation. Radiology. 1983;148(3):641–645. [DOI] [PubMed] [Google Scholar]
- 21. Potter NJ, Brukner PD, Makdissi M, Crossley K, Kiss ZS. Navicular stress fractures: outcomes of surgical and conservative management. Br J Sports Med. 2006;40(8):692–695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Ramadorai MUE, Beuchel MW, Sangeorzan BJ. Fractures and dislocations of the tarsal navicular. J Am Acad Orthop Surg. 2016;24(6):379–389. [DOI] [PubMed] [Google Scholar]
- 23. Sangeorzan BJ, Benirschke SK, Mosca V, Mayo KA, Hansen ST. Displaced intra-articular fractures of the tarsal navicular. J Bone Joint Surg Am. 1989;71(10):1504–1510. [PubMed] [Google Scholar]
- 24. Saxena A, Fullem B. Navicular stress fractures: a prospective study on athletes. Foot Ankle Int. 2006;27(11):917–921. [DOI] [PubMed] [Google Scholar]
- 25. Saxena A, Fullem B, Hannaford D. Results of treatment of 22 navicular stress fractures and a new proposed radiographic classification system. J Foot Ankle Surg. 2000;39(2):96–103. [DOI] [PubMed] [Google Scholar]
- 26. Schroeder GD, Lynch TS, Gibbs DB, et al. Pre-existing lumbar spine diagnosis as a predictor of outcomes in National Football League athletes. Am J Sports Med. 2015;43(4):972–978. [DOI] [PubMed] [Google Scholar]
- 27. Torg JS, Moyer J, Gaughan JP, Boden BP. Management of tarsal navicular stress fractures conservative versus surgical treatment: a meta-analysis. Am J Sports Med. 2010;38(5):1048–1053. [DOI] [PubMed] [Google Scholar]