

Abstract
Purpose:
The purpose of this study is to estimate the unknown burden of retinopathy of prematurity (ROP) blindness from nine states of India using demographic, incidence and treatment data from an ongoing statewide ROP program in Karnataka called the Karnataka Internet Assisted Diagnosis of ROP (KIDROP) and to calculate the fiscal quantum of preventable blindness in these states.
Materials and Methods:
The KIDROP model is an ongoing tele-ROP service providing screening and treatment for ROP in Karnataka since 2008. Using this index strategy, an impact assessment in nine other states was constructed, the number of potential blind babies enumerated, the fiscal quantum of blindness prevented in blind person-years (BPYs), and the increase in burden with improving survival and institutional deliveries calculated.
Results:
The total population in the ten study states is 681.5 million. The eligible babies for ROP screening annually are 467,664. The number of babies admitted to neonatal units is 188,561 of which 160,277 are likely to survive and require screening. Based on KIDROP data, ROP would develop in 35,886 of these infants, and 1281 babies would require treatment annually. The fiscal quantum of BPY saved in these ten states is USD 108.4 million annually, with a further increase of USD 106.8 million with improving infant survival and higher admission rates for delivery.
Conclusion:
A KIDROP like model can provide ROP screening in low-resource settings, remote centers, and regions with few ROP specialists. Expanding the model to other states with similar demographics can prevent over USD 100 million of blindness burden annually.
Keywords: Blind person-years, cost-utility, infant blindness, Karnataka Internet Assisted Diagnosis of Retinopathy of Prematurity, middle-income country, retinopathy of prematurity, screening, telemedicine, tele-retinopathy of prematurity
With over 3.5 million babies born premature annually, India has the dubious distinction of being the nation with the largest number of premature births.[1] With this burden has come the increased risk of blindness from retinopathy of prematurity (ROP), a disease currently experiencing its “third epidemic” in middle-income countries like India.[2,3] ROP blindness is bilateral and permanent and occurs due to incomplete vascularization of the retina, fibrovascular proliferation, and eventual retinal detachment if left untreated. A high birth rate, declining infant mortality, improved survival of low birth weight babies, expanding neonatal units in the rural areas, lack of uniform neonatal care, and the lack of universal screening for ROP and other ocular conditions are some of the reasons that have led to the increased vulnerability of these babies to blindness.
Until recently, ROP in India was reported and believed to exist only in urban neonatal units with an incidence varying from 37% to 54%.[4,5] We reported ROP from semi-urban[6] and rural units[7,8] of Southern India and found that the incidence varied from 22.4% to 41.5%. With over 65% of India's population existing in villages,[9] and <100 ROP specialists nationwide as per the Indian ROP society, there is an unmet need of delivery of ROP care. This leaves a vast majority of rural infants, unscreened and at a potential risk for untreated ROP.[6,8,10] Strategies to provide ROP screening services in rural India have become an important unmet public health challenge.[11]
Index strategy: Karnataka Internet Assisted Diagnosis of Retinopathy of Prematurity
To address this lack of ROP screening service especially in the rural and outreach communities, we developed a tele-ROP platform in 2008, which continues to serve in rural and remote areas of the South Indian state of Karnataka.[7,8,10,11,12,13,14,15,16] Under this program, namely, the Karnataka Internet Assisted Diagnosis of ROP (KIDROP), called the “index strategy” in the manuscript hereafter, nonphysician “technicians” travel to different rural and semi-urban neonatal units on a fixed timetable to perform ROP screening using digital imaging and a tele-ROP platform. Examinations are performed on-site, using a portable, wide field, and digital retinal camera (Retcam Shuttle, Clarity MSI, USA). The images are also uploaded on a secure, indigenous, tele-ROP platform that are accessed by experts on their smartphones to provide near real-time diagnosis.[10,13]
The technicians have been trained using the score for training and accreditation of technicians (STAT) score, to grade and report these images using a priority-weighted algorithm to aid follow-up decisions.[8,10,13] This decision is first made by the on-site Level 3 technician and is then confirmed by the remote ROP specialist who views and reports these images in near real time.[10] This provides the infant's diagnosis to the rural mother before she returns to her residence, which could often be in another district.[15] A baby is scheduled for treatment within 48 h of being “diagnosed to require treatment” (i.e., Type 1 ROP). Laser treatment is performed in most cases in the remote center itself under the supervision of the treating pediatrician by the remote ROP expert or local trained ROP specialists thereby obviating the need for the baby to travel to the city. In some cases, the babies are shifted to the closest center for laser treatment.
Currently, five teams each comprising trained and accredited Level 3 technicians, a project manager and a driver, screen Neonatal Intensive Care Units (NICUs), covering one district headquarters every day, as per a weekly schedule. Subdistrict level babies are referred to these “imaging centers” using a low-cost referral strategy called “Red Card for ROP.”[12] An average of 1250–1500 km is traveled every week by each team. The optimal daily travel allowance for a single team does not exceed 300 km of “radius of neonatal care” calculated as the furthest distance traveled from the headquarters in a single day.
With the Supreme Court of India judgment bringing ROP screening into the medico-legal focus,[17] it has now become imperative for all neonatal units to provide for appropriate ROP screening. Currently, this has not been achieved in the country, with a majority of neonatal units or special newborn care units (SNCUs) across rural India not being covered for ROP care. This calls for an urgent assessment and strategy for nationwide expansion. Since the KIDROP model was validated and verified to “prove that a community-based approach is possible for ROP, by using human resource skill appropriately (task shifting)” by a Center for Disease Control (CDC, Atlanta, USA) guideline report,[18] we used this index strategy and applied it to study the feasibility of expanding this program to other states with similar demographics.
Materials and Methods
Nine states in India were selected for the study. These states were selected based on discussion with ROP specialists and where ROP screening services are either inadequate, or the need was perceived to be significant. Homogeneity of ethnicity across these states in India makes comparisons possible. The regional need in each of these states was determined by personal communications with ophthalmologists, pediatricians, government and nongovernment organizations who have either been trained by our institute in ROP management or who have approached KIDROP for assistance to setup similar programs in their respective states.
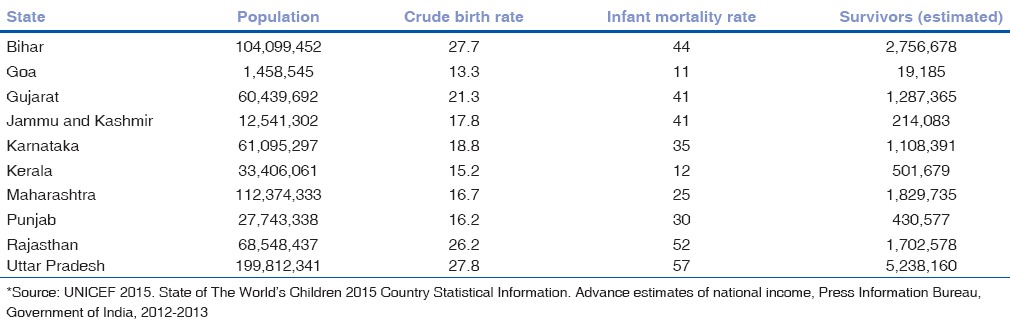
To determine the number of babies who would require ROP screening in these states, we first estimated the number of survivors from the available crude birth rate, population, and infant mortality rate (IMR) of these states.[9,19] Since the national guidelines for ROP screening recommends infants with <2000 g birth weight to be enrolled,[20] the number of babies requiring screening for each state was estimated using the estimated number of babies weighing <2000 g in the general population [Table 1].[21,22]
Table 1.
Calculating the number of babies in at risk states using the national statistics*
In the absence of regional data, the incidence of any stage ROP and treatment requiring disease was estimated using the current incidence of ROP from our program in rural, semi-urban, and urban areas.[6,8,10] A single KIDROP “team” comprised a program manager, two technicians, and a driver. Equipment included the wide-field camera for screening (RetCam Shuttle, Clarity MSI, USA) and laser console for treatment in a portable mobile vehicle. The maximum optimal distance of travel for a unit was 300 km of flat terrain, from the headquarters on any single day. The distance and the changing requirements of the local terrain, including varying conditions such as the desert and sandy regions, hilly and snowed-in areas, inadequate road access, and travel logistics were used to calculate the number of units or teams, and the distances traveled in these selected states.
Amortized costs including equipment, compensation of the teams, and recurring costs were estimated by auditing KIDROP's financial statements and were used to calculate the “total cost” of the program implementation. To estimate the “burden of blindness” in financial equivalents, we used the unit of “blind person years” (BPYs), elucidated in the global initiative for the elimination of avoidable blindness, Vision 2020, Right to Sight, World Health Organization.[21] The financial burden was calculated by multiplying the average life expectancy (from the time of blindness) with the per capita income of the region or country. In this manuscript, we have computed the “burden of blindness” by multiplying the number of babies requiring treatment with the average life expectancy with the per capita income from national data available at the time of submission.[22]
Mathematical calculations and assumptions
Estimating blindness burden
Using the neonatal indices most appropriate to the Indian scenario from Blencowe et al.,[23] we estimated the blindness burden in the study states. The admission to neonatal care and further survival was estimated for each of the states. The development of treatment warranted disease as well as the “blind without treatment” was calculated using the early treatment for ROP[24] risk score of blindness without treatment.[25]
Estimating blind person years in the current scenario
The current rate of treatment warranted ROP and blind without treatment published by Vinekar et al. for the Indian scenario was used to estimate the BPYs in each of the states.[8]
Estimating the scope of improvement: Highest institutional delivery and lowest mortality
The “scope for improvement” was calculated in terms of the increase in BPYs when all the states would be as high as the best state (i.e., Kerala) in terms of institutional deliveries, declining birth rate, and lowest infant mortality.
The KIDROP program adheres to the guidelines of the Declaration of Helsinki with approval by the Institutional Review Board and the Institute Ethics Committee.
Results
The total population in the ten states, (including Karnataka, i.e., the index state) enrolled in this study is 681.5 million. To estimate the number of babies born from these states, we used their respective birth rates and calculated the number of survivors after discounting for the IMRs of each state. This varied from 19,185 in Goa to 5,238,160 in Uttar Pradesh and is detailed in Table 1.
The number of babies developing ROP was then assessed by first estimating the number of babies born <2000 g (467,664 infants) and then the number who would be admitted to the SNCUs or the NICUs by computing the admission rates of these states (20%–80%) which was 188,561 infants. Using the estimated 85% survival rate of these infants, we estimated that annually 160,277 infants would survive and therefore require ROP screening.
Using the incidence of ROP from rural Karnataka's multicenter study, i.e., 22.39% for any stage ROP and 3.57% for treatment-requiring ROP, the incidence was extrapolated to the other nine states. Using these measures, there would be 35,886 infants with ROP (any stage) and 1281 babies who would require treatment annually [Table 2].
Table 2.
Blind person years saved if treatment of retinopathy of prematurity was provided in the 10 study states
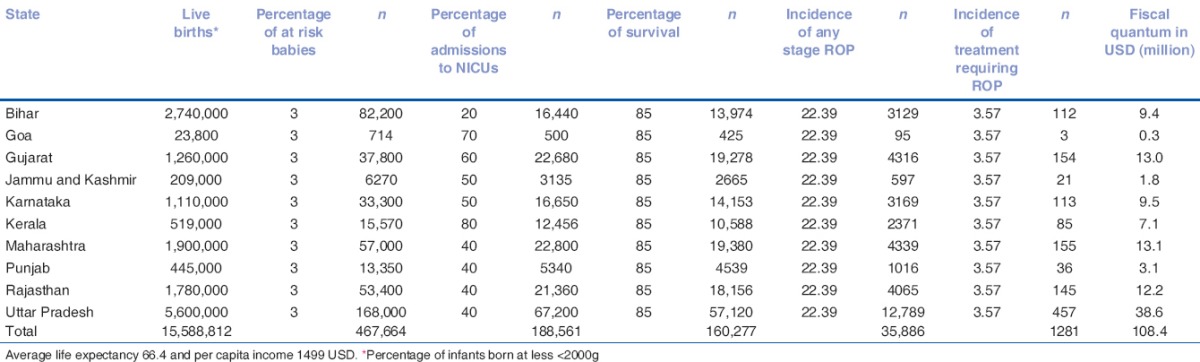
To calculate the BPYs in fiscal equivalents, we multiplied the number of babies going blind with the per capita income (USD 1499) and the average life expectancy (66.4 years). In Karnataka, with this index strategy, the fiscal quantum of BPY saved is USD 9.5 million, and for the ten study states, it is USD 108.4 million.
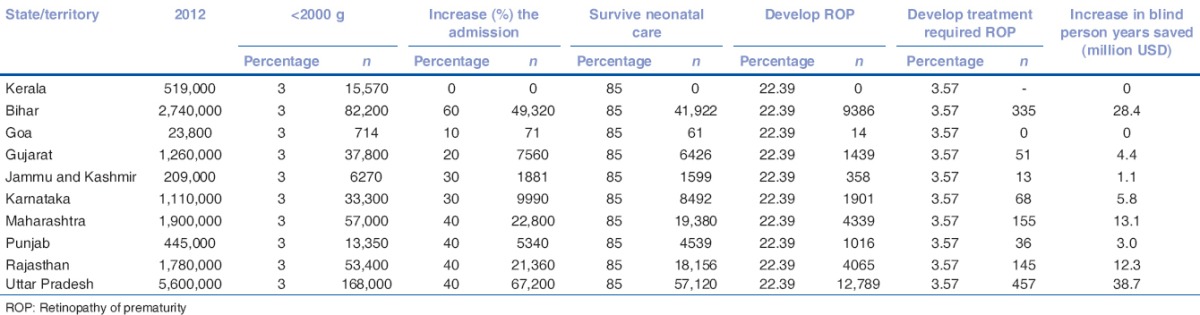
To estimate the increase in the number of preterm babies who would survive if there were an increase in the proportion of institutional deliveries, we used Kerala as the “model” state (which currently has 80% institutional deliveries). The delivery rate of each study state was proportionally increased to equal Kerala, and the number of babies and the increase in percentage from their existing was computed (increase in % of admission) [Table 3]. The increase in the fiscal quantum of BPYs saved was 106.8 million USD when the rate of institutional delivery in all our chosen states increased to 80% with 85% survival rate [Table 3].
Table 3.
Increase in blind person years burden encountered if study states improved in increase in neonatal Intensive Care Unit admission and infant survival
Discussion
Over the past two decades, India has made laudable progress in infant health-care indices. The IMR has dropped from 81/1000 live births in 1990 to 47/1000 live births in 2011, and there is a further reduction in this trend.[1,9,19] This has led to an increase in surviving neonates, including low-birth weight and preterm babies, even in rural centers. These factors have added to the unmet challenge of ROP screening.[11] The problem is worse with inadequate awareness of ROP among pediatricians, gynecologists, and even ophthalmologists along with the dismal lack of sufficiently trained ROP specialists and adequate infrastructure.
To address this felt need of ROP service, particularly in the outreach centers, an imaging-based screening model with telemedicine was conceived. Since 2008, nonphysician technicians have been trained to use a portable RetCam Shuttle (Clarity MSI, USA) and validated against ROP experts performing indirect ophthalmoscopy. An indigenously developed 20-point score (STAT score) graded their ability (Level 1–3) to image and determine follow-up based on a three-way algorithm.[8,10,13] Infants were followed up based on the findings of each examination with adherence to the national ROP guidelines.[20] A baby was followed up until a mature retina was imaged on two consecutive visits, one of these between 41 and 45 weeks of postmenstrual age.[8,10] Images were also uploaded on a secure tele-ROP platform and accessed and reported by remote experts on their smartphones (iPhone, Apple Inc., USA). The sensitivity, specificity, positive predictive value, and negative predictive value for the treatment grade disease were 95.7, 93.2, 81.5, and 98.6, respectively. The kappa for technicians to decide discharge of babies was 0.94 (P < 0.001). A Level 3 technician missed only 0.4% of infants needing treatment.[10]
The relevance of imaging-based ROP screening programs for India was assessed in a report that validated the KIDROP model based on the CDC guidelines, by the National Health and Medical Research Council, Government of Australia.[18] The report had important observations that have led to the scaling up of this model across other states. The report observed that (1) there were insufficient ROP experts in the government sector to provide service to the SNCUs. Further, “a transition allowing government doctors to screen for ROP using indirect ophthalmoscopy without monitoring or surveillance would be perilous.” This is similar to the experience in Mexico where only 31.2% of centers were compliant for ROP services when it had the ophthalmologist led indirect ophthalmoscopy model, 34.4% were not compliant, and the remaining 34.4% had no program at all.[26] (2) A community approach to ROP screening would be possible using human resource skills appropriately using “task shifting,” suggesting that nonphysicians employed in imaging would address the lacunae of experts. (3) Using the example of the Polio Program in India, the government should engage private expertise in ROP to screen in government centers using the model of public-private partnerships. (4) The role of photodocumentation in babies requiring treatment and for monitoring outcome has medico-legal significance. (5) With the Supreme Court of India judgment,[17] ROP care is now mandated. Sub-optimal management could expose the government to medico-legal liability.
These are some of the reasons that have promoted interest in tele-ROP-based models. In this manuscript, we attempted to assess the blindness burden that exists in nine other Indian states that have an ROP problem, and assess the “increase” in this burden that is likely to occur with further improvement of neonatal standards and higher institutional deliveries. The KIDROP strategy would save the index state USD 9.5 million in BPYs. The benefit in ten states would be USD 108 million with a further increase of USD 106 million with improving standards.
The current limitation of expanding the program to other states, even with government support and multiple public-private partnerships, would be (1) the cost of the infant retinal camera (i.e., the RetCam). Currently, in India, the device is sold at approximately USD 110,000. The ten study states would require approximately 55 KIDROP like units. This would cost approximately 11 million USD at the cost of USD 200,000/unit, based on KIDROP's estimated costs. Low-cost and indigenously developed cameras need to be evolved. (2) Training and accrediting of “infant imagers” needs to be standardized. The STAT score is one such objective training module.
Conclusion
In the current scenario, increasing the number of ROP trained ophthalmologists across the nation may not be possible in a short interval. With the sudden increase in the number of neonatal units across rural India, improving neonatal standards and higher proportion of institutional deliveries are placing an increasing number of preterm infants at risk of unscreened ROP blindness. Expansion of an imaging based, tele-ROP network like KIDROP maybe one of the options to address this lacuna. Collective cost-benefit analysis of this program from other states would help assess its utility in different regional settings.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to acknowledge KIDROP team members, Praveen Sharma, Sivakumar Munusamy, Krishnan AN, Muralidhar Gayakwad, Ravishankar Kandagal, Madhava Padaki and Someshwar Matad for their participation and support in this study.
References
- 1.Howson CP, Kinney MV, Lawn JE. March of Dimes, PMNCH, Save the Children, WHO. Born Too Soon: The Global Action Report on Preterm Birth. Geneva: World Health Organization; 2012. [Google Scholar]
- 2.Gilbert C, Rahi J, Eckstein M, O’Sullivan J, Foster A. Retinopathy of prematurity in middle-income countries. Lancet. 1997;350:12–4. doi: 10.1016/S0140-6736(97)01107-0. [DOI] [PubMed] [Google Scholar]
- 3.Gilbert C, Fielder A, Gordillo L, Quinn G, Semiglia R, Visintin P, et al. Characteristics of infants with severe retinopathy of prematurity in countries with low, moderate, and high levels of development: Implications for screening programs. Pediatrics. 2005;115:e518–25. doi: 10.1542/peds.2004-1180. [DOI] [PubMed] [Google Scholar]
- 4.Charan R, Dogra MR, Gupta A, Narang A. The incidence of retinopathy of prematurity in a neonatal care unit. Indian J Ophthalmol. 1995;43:123–6. [PubMed] [Google Scholar]
- 5.Vinekar A, Dogra MR, Sangtam T, Narang A, Gupta A. Retinopathy of prematurity in Asian Indian babies weighing greater than 1250 grams at birth: Ten year data from a tertiary care center in a developing country. Indian J Ophthalmol. 2007;55:331–6. doi: 10.4103/0301-4738.33817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hungi B, Vinekar A, Datti N, Kariyappa P, Braganza S, Chinnaiah S, et al. Retinopathy of prematurity in a rural Neonatal Intensive Care Unit in South India – A prospective study. Indian J Pediatr. 2012;79:911–5. doi: 10.1007/s12098-012-0707-y. [DOI] [PubMed] [Google Scholar]
- 7.Vinekar A. IT-enabled innovation to prevent infant blindness in rural India: The KIDROP experience. J Indian Bus Res. 2011;3:98–102. [Google Scholar]
- 8.Vinekar A, Jayadev C, Mangalesh S, Shetty B, Vidyasagar D. Role of tele-medicine in retinopathy of prematurity screening in rural outreach centers in India – A report of 20,214 imaging sessions in the KIDROP program. Semin Fetal Neonatal Med. 2015;20:335–45. doi: 10.1016/j.siny.2015.05.002. [DOI] [PubMed] [Google Scholar]
- 9.Suryanarayana MH, Agrawal A, Prabhu KS. Inequality-adjusted Human Development Index for India's States. India: UNDP; 2011. [Google Scholar]
- 10.Vinekar A, Gilbert C, Dogra M, Kurian M, Shainesh G, Shetty B, et al. The KIDROP model of combining strategies for providing retinopathy of prematurity screening in underserved areas in India using wide-field imaging, tele-medicine, non-physician graders and smart phone reporting. Indian J Ophthalmol. 2014;62:41–9. doi: 10.4103/0301-4738.126178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dutta S, Raghuveer T, Vinekar A, Dogra MR. Can we stop the current epidemic of blindness from retinopathy of prematurity? Indian Pediatr. 2016;53(Suppl 2):S80–4. [PubMed] [Google Scholar]
- 12.Vinekar A, Avadhani K, Dogra M, Sharma P, Gilbert C, Braganza S, et al. A novel, low-cost method of enrolling infants at risk for retinopathy of prematurity in centers with no screening program: The REDROP study. Ophthalmic Epidemiol. 2012;19:317–21. doi: 10.3109/09286586.2012.698358. [DOI] [PubMed] [Google Scholar]
- 13.Vinekar A, Jayadev C, Bauer N. Need for telemedicine in retinopathy of prematurity in middle-income countries: E-ROP vs. KIDROP. JAMA Ophthalmol. 2015;133:360–1. doi: 10.1001/jamaophthalmol.2014.4913. [DOI] [PubMed] [Google Scholar]
- 14.Vinekar A, Avadhani K, Braganza S, Shetty B, Dogra M, Gilbert C. Outcomes of a protocol-based management for zone 1 retinopathy of prematurity: The Indian twin cities ROP screening program report number 2. Am J Ophthalmol. 2011;152:712. doi: 10.1016/j.ajo.2011.06.011. [DOI] [PubMed] [Google Scholar]
- 15.Vinekar A, Jayadev C, Dogra M, Shetty B. Improving follow-up of infants during retinopathy of prematurity screening in rural areas. Indian Pediatr. 2016;53(Suppl 2):S151–4. [PubMed] [Google Scholar]
- 16.Vinekar A, Jayadev C, Mangalesh S, Kurian M, Dogra M, Bauer N, et al. Initiating retinopathy of prematurity screening before discharge from the neonatal care unit: Effect on enrolment in Rural India. Indian Pediatr. 2016;53(Suppl 2):S107–11. [PubMed] [Google Scholar]
- 17.Supreme Court Judgement. [Last accessed on 2017 Mar 09]. Available from: http://www.supremecourtofindia.nic.in/FileServer/2015-07-02_1435823185.pdf .
- 18.CDC. Developing an Effective Evaluation Report. 2013. [Last accessed on 2017 Mar 09]. Available from: https://www.cdc.gov/eval/materials/Developing-An-Effective-Evaluation-Report_TAG508.pdf .
- 19.UNICEF. State of the World's Children 2015 Country Statistical Information. UNICEF. 2015 [Google Scholar]
- 20.Pejaver RK, Vinekar A, Bilagi A. National Neonatology Foundation's Evidence Based Clinical Practice Guidelines. Retinopathy of Prematurity (NNF, India, Guidelines) 2010:253–62. [Google Scholar]
- 21.World Health Organization. The Global Initiative for Elimination of Avoidable Blindness. (WHO/PBL/97.61 Rev 1) Geneva: World Health Organization; 1997. [Google Scholar]
- 22.Government of India. Advance Estimates of National Income. Bureau, Government of India. 2012-2013 [Google Scholar]
- 23.Blencowe H, Lawn JE, Vazquez T, Fielder A, Gilbert C. Preterm-associated visual impairment and estimates of retinopathy of prematurity at regional and global levels for 2010. Pediatr Res. 2013;74(Suppl 1):35–49. doi: 10.1038/pr.2013.205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Early Treatment for Retinopathy of Prematurity Cooperative Group. Revised indications for the treatment of retinopathy of prematurity: Results of the early treatment for retinopathy of prematurity randomized trial. Arch Ophthalmol. 2003;121:1684–94. doi: 10.1001/archopht.121.12.1684. [DOI] [PubMed] [Google Scholar]
- 25.Zin A, Gole GA. Retinopathy of prematurity-incidence today. Clin Perinatol. 2013;40:185–200. doi: 10.1016/j.clp.2013.02.001. [DOI] [PubMed] [Google Scholar]
- 26.Zepeda-Romero LC, Gilbert C. Limitations in ROP programs in 32 Neonatal Intensive Care Units in five states in Mexico. Biomed Res Int 2015. 2015:712624. doi: 10.1155/2015/712624. [DOI] [PMC free article] [PubMed] [Google Scholar]