

Abstract
Purpose:
The purpose of the study is to present anterior segment optical coherence tomography (AS-OCT) as an alternative method of evaluating Kayser–Fleischer (KF) ring in Wilson disease (WD) not only by ophthalmologists but also by other clinicians dealing with WD.
Materials and Methods:
This was a retrospective case series of six WD patients with KF ring. Evaluation of KF ring was done by naked eye examination using torch light, slit lamp biomicroscopy (SL), and AS-OCT. SL examination was done using a narrow slit of the superior cornea. AS-OCT was done using the Optovue RTvue Premier™ device (Fremont, CA, USA).
Results:
AS-OCT revealed KF ring as an intense hyperreflective band at the level of Descemet membrane (DM). Color scale of AS-OCT showed KF ring as greenish/greenish yellow/orange yellow/yellowish/red band. Validation of AS-OCT findings was done by second ophthalmologist, medical gastroenterologist, surgical gastroenterologist, and neurophysician. After seeing the first observation, they could identify the AS-OCT features in all pictures with ease.
Conclusions:
This is the first observation of KF ring in WD on AS-OCT. On AS-OCT, KF ring is visualized as intense hyperreflectivity at the level of DM in the peripheral cornea. Further, studies are needed to evaluate the usefulness of AS-OCT in WD management.
Keywords: Copper, Kayser–Fleischer ring, optical coherence tomography, slit lamp biomicroscopy, Wilson disease
Wilson disease (WD) is a genetic disorder, in which there is an inherited defect in the biliary excretion of copper due to which copper accumulates in the liver, brain, cornea, and other organs resulting in hepatic, neurological/psychiatric, eye, and other manifestations.[1,2] The accumulated copper on Descemet membrane (DM) of the peripheral cornea is called Kayser–Fleischer (KF) ring. KF ring is named after German ophthalmologists Bernhard Kayser (1902) and Bruno Fleischer (1903), who described it independently.[3] Diagnosis of WD is based on at least two of the following: Detection of KF rings on slit lamp biomicroscopy (SL) examination, typical neurological/hepatic symptoms, and/or a low serum ceruloplasmin.[4,5] WD has an autosomal recessive mode of inheritance with a worldwide frequency between 1 in 35,000 and 1 in 1,00,000 live births and a carrier rate of 1 in 90.[2]
The identification of KF ring remains the most important clinical sign for the diagnosis of WD. In the absence of KF ring, WD is difficult to diagnose and even centers with expertise consider diagnosis as a challenge in some cases. KF ring may present as the first detectable manifestation of WD.[6] Detection of KF ring in presymptomatic cases of WD may lead to early diagnosis and subsequent management. The ring is seen in the peripheral cornea as greenish yellow or golden brown deposit on DM.[7,8] It is almost always bilateral, starts superiorly first and then inferiorly, and later becomes circumferential.[9,10] SL of the cornea by a skilled observer is considered the most reliable method of detecting KF ring.[2]
In this case series, we present the evaluation of KF ring by anterior segment optical coherence tomography (AS-OCT) in WD. OCT is a noncontact optical device that provides cross-sectional images of the eye and does quantitative analysis of ocular tissues.[11]
Materials and Methods
Retrospective case series of six WD patients with KF ring was seen during the study period from August 2015 to October 2015. The Institutional Ethics Committee approved the study. Demographic data, presence of liver manifestations, involvement of central nervous system, other manifestations, history of consanguinity, sibling history, and presence of KF ring were noted for all the patients. Evaluation of KF ring was done by naked eye using torch light, SL, and AS-OCT. SL examination was done using a narrow slit of the superior cornea. AS-OCT was done using Optovue RTvue Premier™ (Fremont, CA, USA). The AS-OCT of Optovue RTvue is converted from a retinal scanner using 830 nm. The method of acquiring AS-OCT pictures of the cornea is as follows. The cornea anterior module lens was attached to the OCT machine. Red external fixation light emitting diode (LED) on headrest was used to illuminate the cornea. CL-line scan of 8 mm length (horizontal and vertical) was selected. Cornea image in between the two red-guided lines was located, and the “auto” scan was selected. The scan has a predetermined setting of illumination of 685 units, brightness of 127, and contrast of 255, for dark eyes. The observation of KF ring findings on AS-OCT was validated by second ophthalmologist, medical gastroenterologist, surgical gastroenterologist, and neurologist to see for inter- and intra-observer variability.
Results
The demographic data, laboratory test results, systemic involvement, other organ involvement, and family history are shown in Table 1. In the naked eye examination using a torch light, KF ring was seen as a yellowish deposit in the peripheral cornea. In SL examination, KF ring was seen as greenish/yellowish green/yellowish deposit at the level of DM in the peripheral cornea. Table 2 shows the KF ring findings on SL examination and AS-OCT. The KF ring on AS-OCT was visualized as an intense hyperreflective band at the level of DM in the peripheral cornea [Figs. 1a and 2a]. The color scale of AS-OCT showed KF ring as greenish/greenish yellow/orange yellow/yellowish/red band [Figs. 1b and 2b].
Table 1.
Demographic data, manifestations, and family history of Wilson disease patients with Kayser–Fleischer ring
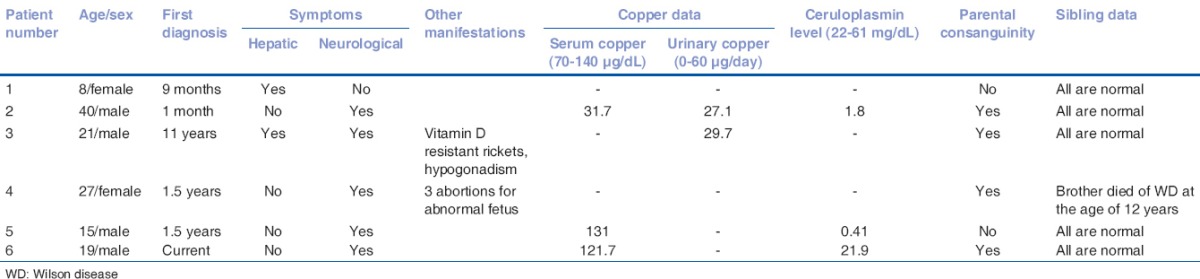
Table 2.
Kayser–Fleischer ring on slit lamp biomicroscopy examination and anterior segment optical coherence tomography
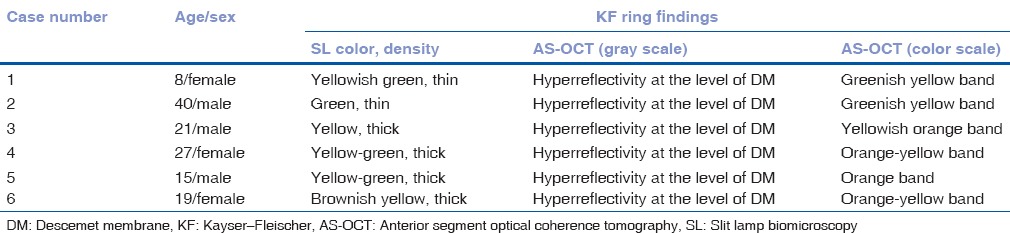
Figure 1.

(a) Anterior segment optical coherence tomography gray scale analysis of Kayser–Fleischer ring of patient four showing hyperreflectivity (arrow) at the level of Descemet membrane. (b) Color scale of anterior segment optical coherence tomography of Kayser–Fleischer ring of patient four showing orange-yellow band (arrow) at the level of Descemet membrane
Figure 2.

(a) Anterior segment optical coherence tomography gray scale analysis of Kayser–Fleischer ring of patient five showing hyperreflectivity (arrow) at the level of Descemet membrane. (b) Color scale of anterior segment optical coherence tomography of Kayser–Fleischer ring of patient five showing predominantly orange band (arrow) at the level of Descemet membrane
Anterior segment optical coherence tomography of control
Gray scale of AS-OCT in control (healthy individual) showed no hyperreflectivity at the level of DM in peripheral cornea [Fig. 3a]. The color scale also did not show any color band at the level of DM in the peripheral cornea of the same eye [Fig. 3b].
Figure 3.

(a) Anterior segment optical coherence tomography gray scale analysis of control showing no hyperreflectivity at the level of Descemet membrane. (b) Anterior segment optical coherence tomographic color scale analysis of control showing no hyperreflectivity band at the level of descended membrane
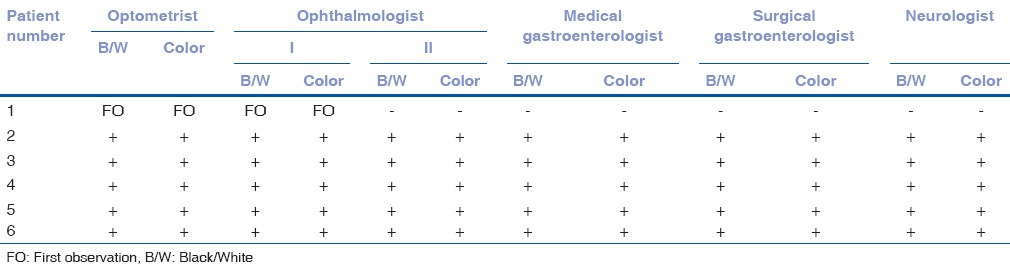
Table 3 gives the validation of AS-OCT findings of KF ring by other clinicians. They could identify the AS-OCT features of KF ring in all pictures with ease.
Table 3.
Assessing the inter- and intra-observer variability of Kayser–Fleischer ring analysis by anterior segment optical coherence tomography
Discussion
OCT is a noncontact device that provides cross-sectional images and quantitative analysis of the ocular tissues.[11] AS-OCT has been found to be useful in eye clinics practicing corneal and AS surgeries.[12] In this case series of WD patients, KF ring was evaluated by AS-OCT. KF ring on the gray scale of AS-OCT was observed as hyperreflectivity of DM in the peripheral cornea. KF ring was observed as a greenish/greenish yellow/orange yellow/yellowish/red band on the color scale of AS-OCT.
AS-OCT can be an important alternative tool for KF ring evaluation in WD management. Ophthalmologists get referrals commonly from medical gastroenterologists and neurophysicians to look for KF ring in undiagnosed liver disease or in patients with central nervous system features/psychiatric manifestations. An ophthalmologist who has not seen KF ring before may miss an early KF ring. The gray scale of AS-OCT can pick KF ring as hyperreflectivity at the level of DM in the peripheral cornea. In case if an early KF ring is missed on SL examination and AS-OCT shows hyperreflectivity at the level of DM, the ophthalmologist can go back to look at KF ring carefully with SL.
The validation of AS-OCT findings was done by other clinicians. The observation of KF ring findings on AS-OCT was validated by second ophthalmologist, medical gastroenterologist, surgical gastroenterologist, and neurologist. After seeing the first observation, clinicians could identify the AS-OCT features in all pictures with ease. Physicians other than ophthalmologists dealing with WD will be able to see KF ring on AS-OCT.
To conclude, this is the first observation of KF ring in WD on AS-OCT. A literature search by PubMed did not reveal references to it. On AS-OCT, KF ring is visualized as intense hyperreflectivity at the level of DM in the peripheral cornea. Further studies are warranted to evaluate the usefulness of AS-OCT in the WD management.
Financial support and sponsorship
The study was partly funded by the KIMS Foundation and Research Centre and the Ophthalmology department of KIMS Hospitals.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The contribution by all the authors is acknowledged along with the technical team of the ophthalmology department. We thank the patients and their family members for participating in the study.
References
- 1.Behari M, Pardasani V. Genetics of Wilsons disease. Parkinsonism Relat Disord. 2010;16:639–44. doi: 10.1016/j.parkreldis.2010.07.007. [DOI] [PubMed] [Google Scholar]
- 2.European Association for Study of Liver. EASL Clinical Practice Guidelines: Wilson's disease. J Hepatol. 2012;56:671–85. doi: 10.1016/j.jhep.2011.11.007. [DOI] [PubMed] [Google Scholar]
- 3.Harry J, Tripathi R. Kayser-Fleischer ring. A pathological study. Br J Ophthalmol. 1970;54:794–800. doi: 10.1136/bjo.54.12.794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sternlieb I. Perspectives on Wilson's disease. Hepatology. 1990;12:1234–9. doi: 10.1002/hep.1840120526. [DOI] [PubMed] [Google Scholar]
- 5.Bandmann O, Weiss KH, Kaler SG. Wilson's disease and other neurological copper disorders. Lancet Neurol. 2015;14:103–13. doi: 10.1016/S1474-4422(14)70190-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Liu M, Cohen EJ, Brewer GJ, Laibson PR. Kayser-Fleischer ring as the presenting sign of wilson disease. Am J Ophthalmol. 2002;133:832–4. doi: 10.1016/s0002-9394(02)01408-3. [DOI] [PubMed] [Google Scholar]
- 7.Sullivan CA, Chopdar A, Shun-Shin GA. Dense Kayser-Fleischer ring in asymptomatic Wilson's disease (hepatolenticular degeneration) Br J Ophthalmol. 2002;86:114. doi: 10.1136/bjo.86.1.114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tauber J, Steinert RF. Pseudo-Kayser-Fleischer ring of the cornea associated with non-Wilsonian liver disease. A case report and literature review. Cornea. 1993;12:74–7. doi: 10.1097/00003226-199301000-00013. [DOI] [PubMed] [Google Scholar]
- 9.Innes JR, Strachan IM, Triger DR. Unilateral Kayser-Fleischer ring. Br J Ophthalmol. 1986;70:469–70. doi: 10.1136/bjo.70.6.469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Suvarna JC. Kayser-Fleischer ring. J Postgrad Med. 2008;54:238–40. doi: 10.4103/0022-3859.41816. [DOI] [PubMed] [Google Scholar]
- 11.Izatt JA, Hee MR, Swanson EA, Lin CP, Huang D, Schuman JS, et al. Micrometer-scale resolution imaging of the anterior eye in vivo with optical coherence tomography. Arch Ophthalmol. 1994;112:1584–9. doi: 10.1001/archopht.1994.01090240090031. [DOI] [PubMed] [Google Scholar]
- 12.Ramos JL, Li Y, Huang D. Clinical and research applications of anterior segment optical coherence tomography-a review. Clin Exp Ophthalmol. 2009;37:81–9. doi: 10.1111/j.1442-9071.2008.01823.x. [DOI] [PMC free article] [PubMed] [Google Scholar]